Article Text

Abstract
Objectives The primary aim of this prospective study was to perform a comprehensive serial characterisation of monocyte and neutrophil function, circulating monocyte subsets, and bronchoalveolar lavage (BAL) fluid after lung resection. A secondary aim was to perform a pilot, hypothesis-generating evaluation of whether innate immune parameters were associated with postoperative pneumonia.
Methods Forty patients undergoing lung resection were studied in detail. Blood monocytes and neutrophils were isolated preoperatively and at 6, 24 and 48 h postoperatively. BAL was performed preoperatively and immediately postoperatively. Monocyte subsets, monocyte responsiveness to lipopolysaccharide (LPS) and neutrophil phagocytic capacity were quantified at all time points. Differential cell count, protein and cytokine concentrations were measured in BAL. Pneumonia evaluation at 72 h was assessed using predefined criteria.
Results After surgery, circulating subsets of classical and intermediate monocytes increased significantly. LPS-induced release of proinflammatory cytokines from monocytes increased significantly and by 48 h a more proinflammatory profile was found. Neutrophil phagocytosis demonstrated a small but significant fall. Factors associated with postoperative pneumonia were: increased release of specific proinflammatory and anti-inflammatory cytokines from monocytes; preoperative neutrophilia; and preoperative BAL cell count.
Conclusions We conclude that postoperative lung inflammation is associated with specific changes in the cellular innate immune response, a better understanding of which may improve patient selection and prediction of complications in the future.
- Innate Immunity
- Thoracic Surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
Lung resection is followed by a systemic innate immune response characterised by an increase in classical and intermediate monocytes, heightened pro-inflammatory responsiveness of monocytes, and reduced neutrophil phagocytic capacity.
-
Within 2 hours of lung resection, an inflammatory response evolves in the contralateral lung.
-
Pre-operative and pre-operative characteristics of the innate cellular innate immune response appear to be associated with post-operative lung inflammation, though these require validation in future studies.
Introduction
In recent years, there has been increasing recognition of a complex innate immune response to insults such as sepsis or trauma. It is generally accepted that such processes induce not only a systemic inflammatory response syndrome, but also a compensatory anti-inflammatory response (CARS).1 ,2 The magnitude and duration of both processes appear to dictate clinical outcomes, suggesting that a closely coordinated interaction between these apparently divergent responses is beneficial.3
These concepts have largely arisen from meticulous serial analysis of plasma cytokines. Far less is known about the innate cellular immune response in this context. Monocytes are known to infiltrate the lung in a diverse range of inflammatory lung conditions.4–7 Improved methods for phenotypic characterisation have led to clear demonstrations of distinct subsets of circulating murine monocytes, and a similar concept has emerged in humans with the identification of classical, non-classical and intermediate monocyte subsets.8–11 Monocyte deactivation has been associated with adverse outcomes in patients with sepsis.12–15 However, remarkably little is known about serial functional responses of monocytes and neutrophils under pathological conditions.
The aim of this study was therefore to perform the first detailed ‘within-patient’ characterisation of circulating cellular innate responses after lung resection. The setting of lung resection was chosen as there is a relatively consistent and controlled level of surgical trauma, and because thoracic surgery may be complicated by postoperative infection or acute lung injury (ALI).16–18 Secondary aims were: (1) to make preliminary analyses of whether innate immune dysfunction predicted postoperative complications (in the form of alveolar consolidation on chest X-ray (CXR) at 72 h) and (2) to take the unique opportunity to study serial cellular responses in bronchoalveolar lavage (BAL) fluid from patients having lung resection.
Materials and methods
Recruitment of patients
Patients referred for thoracic surgery with proven or clinically suspected lung cancer were enrolled prospectively. They were excluded if there was evidence of metastatic disease on routine preoperative staging. All patients were surgically staged with bronchoscopy and videomediastinoscopy prior to lung resection. Informed, written consent was obtained from all patients.
Blood sampling and preparation
Venepuncture was performed preoperatively and at 6, 24 and 48 h postoperatively. Isolation of granulocytes and mononuclear cells from whole blood was performed at each time point using dextran sedimentation and percoll gradient extraction.19 Neutrophil purity in extracted granulocyte layers was consistently >95%. Monocytes were positively selected from the mononuclear layer using magnetic beads labelled with an anti-CD14 antibody (Miltenyi Biotec, Germany). Using this technique, the monocyte purity was consistently >90%.
Flow cytometric analysis of monocyte subsets
Five-colour immunofluorescent labelling of the mononuclear layer of freshly prepared blood was performed (using antibodies specific to HLA-DR, CD14, CD16, CCR2 and CX3CR1). An unstained sample and five single stains were used to compensate the data with a mixture sample containing all five antibodies used to identify monocyte subsets.
Monocytes were identified by gating on a cell population with the characteristic forward scatter and side scatter. Within this gate, HLA-DR-positive cells were identified, and relative CD14 and CD16 expression on these was used to identify the three principal human monocyte subsets (CD14++CD16− ‘classical’ monocytes; CD14++CD16+ ‘intermediate’ monocytes; and CD14+CD16++ ‘non-classical’ monocytes). Antibodies to CCR2 and CX3CR1 were used to confirm that each of the three monocyte subsets (identified by the relative CD14/CD16 expression) had the characteristic expression profile for these receptors.
Stimulation of monocytes with lipopolysaccharide
Isolated monocytes were stimulated with lipopolysaccharide (LPS) from Escherichia coli 026:B6 (Sigma, UK), final concentration 154 ng/mL, for 18 h in duplicate in a 24-well Costar plate (Corning, Amsterdam). Supernatants were collected and frozen at −80°C until later analysis. Data were adjusted for total protein using the Bradford method (Sigma, UK).
Phagocytosis by neutrophils
Phagocytosis by freshly prepared neutrophils was evaluated by flow cytometric analysis of neutrophils exposed to serum-opsonised zymosan (from Saccharomyces cerevisiae) preconjugated with Alexa Fluor 594 (Invitrogen, UK). Following culture in suspension for 30 min, addition of trypan blue (to quench extracellular fluorescence) and multiple washes, flow cytometric analysis was performed (BD Special Order LSR Fortessa, Becton Dickinson). The data were subsequently analysed using FlowJo Software (V.7.6.3; TreeStar Inc) with the unstained sample being used as the basis of the gating for positive phagocytosis.
Bronchoalveolar lavage
BAL was performed twice in each patient at least 1 week apart, thereby allowing any BAL-induced inflammation to recede. The first BAL was performed prior to mediastinoscopy, that is, before any form of surgical trauma, thus serving as a preoperative sample. The second BAL was performed immediately after lung resection and served as an early postoperative comparator sample. BAL was performed in the lung contralateral to the tumour on both occasions, and a different lobe was lavaged at the second BAL.
BAL was performed under general anaesthesia using a standardised technique.20 Quantification of cell counts, total protein and preparation of cell-free supernatant for later analysis were performed as described previously.20
Cytokine analysis
Serum and BAL cytokines were analysed using a commercially available Cytometric Bead Array kit (BD Human Inflammatory Cytokines Kit, Becton Dickinson Biosciences).
Definition of postoperative pneumonia
Pneumonia was predefined as new alveolar infiltrates on a CXR at 72 h, reported by an experienced pulmonary radiologist blinded to study results, plus two from three of: temperature >38.0°C or <35.5°C; white cell count >11.0×109/L or <4.0×109/L; and positive microbiology on sputum culture.
Statistical analysis
Data were analysed using the Minitab 16 Software (Minitab Inc). Normality of distribution was assessed using the Anderson-Darling test. Non-normally distributed data were log10 transformed prior to further analysis. Postoperative changes were compared using the paired t test and groups compared using the two-sample Student t test. A repeated measures ANOVA/ANCOVA model was created to incorporate analysis of variance attributable to time points and the pneumonia group. To determine relative risk, Youden's test was applied to parameters that were significantly higher in patients with pneumonia to establish the optimal cut-off for predicting pneumonia. The relative risk for each parameter was then determined using Fisher's test and the likelihood ratio calculated. Statistical significance was considered to be at the p<0.05 level. The statistical programme GraphPad Prism 5 (GraphPad Software Inc) was used for this purpose.
Results
Patient characteristics
Fifty-three patients consented to take part, of whom 13 were excluded (7 had lymph node involvement at mediastinoscopy, 2 withdrew consent postoperatively, 1 was deemed medically unfit for resection after staging and 3 were excluded for practical reasons precluding full sample collection). Demographic and clinical characteristics of the 40 patients analysed are shown in table 1. Sixteen patients (40%) had a preoperative diagnosis of chronic obstructive pulmonary disease. Surgical resection was performed whenever possible via video-assisted thoracoscopic surgery (VATS) lobectomy (n=26); otherwise, posterolateral thoracotomy (n=14) was performed. Seventeen patients (42.5%) proved to have adenocarcinoma and 14 (35.0%) had squamous cell carcinoma. Details of final histological diagnoses and staging are described in the online supplementary section (table S1).
Patient characteristics
Response of circulating blood neutrophils and monocytes to lung resection
As expected, a significant postoperative leucocytosis was observed (p<0.0005 by ANOVA modelling). This largely reflected a significant rise in blood neutrophils, but there was an associated significant rise in monocytes and a fall in lymphocytes (p<0.0005 for each cell type by ANOVA modelling).
Table 2 describes the effect of LPS on blood-derived monocytes. It should be emphasised that these data are for all cytokines released from circulating CD14-positive monocytes (ie, no inferences can be drawn in relation to secretion by monocyte subsets or to intracellular expression of the cytokines described). It should also be emphasised that each time point describes the effects of LPS stimulation—basal levels of cytokine secretion from preoperative monocytes that were not stimulated with LPS are shown in the online supplementary section (table S2). ANOVA modelling revealed a significant postoperative increase in IL-8 and tumour necrosis factor (TNF) release from monocytes stimulated with LPS ex vivo (table 2). By 48 h IL-8, TNF and IL-6 secretion were increased significantly, and IL-10 secretion decreased significantly, suggesting a tendency towards monocytes exhibiting a more proinflammatory state of responsiveness.
Ex vivo monocyte responsiveness to stimulation with LPS
The response in serum cytokines over the same time course was subtly different from the response of isolated monocytes to LPS. In serum, IL-6, IL-8 and IL-10 showed very similar trends, all rising gradually to 24 h, and returning towards (but not back to) baseline by 48 h (all p<0.0005 by ANOVA modelling; details are found in the online supplementary section, table S3). No significant differences were observed in the postoperative serum levels of IL-1β, IL-12 or TNF.
Surgery was associated with a significant absolute increase in circulating populations of both classical and intermediate monocytes postoperatively, with a corresponding non-significant trend towards a reduction in the number of non-classical monocytes (figure 1A, B). The increase in classical and intermediate monocytes appeared to be established by 24 h.
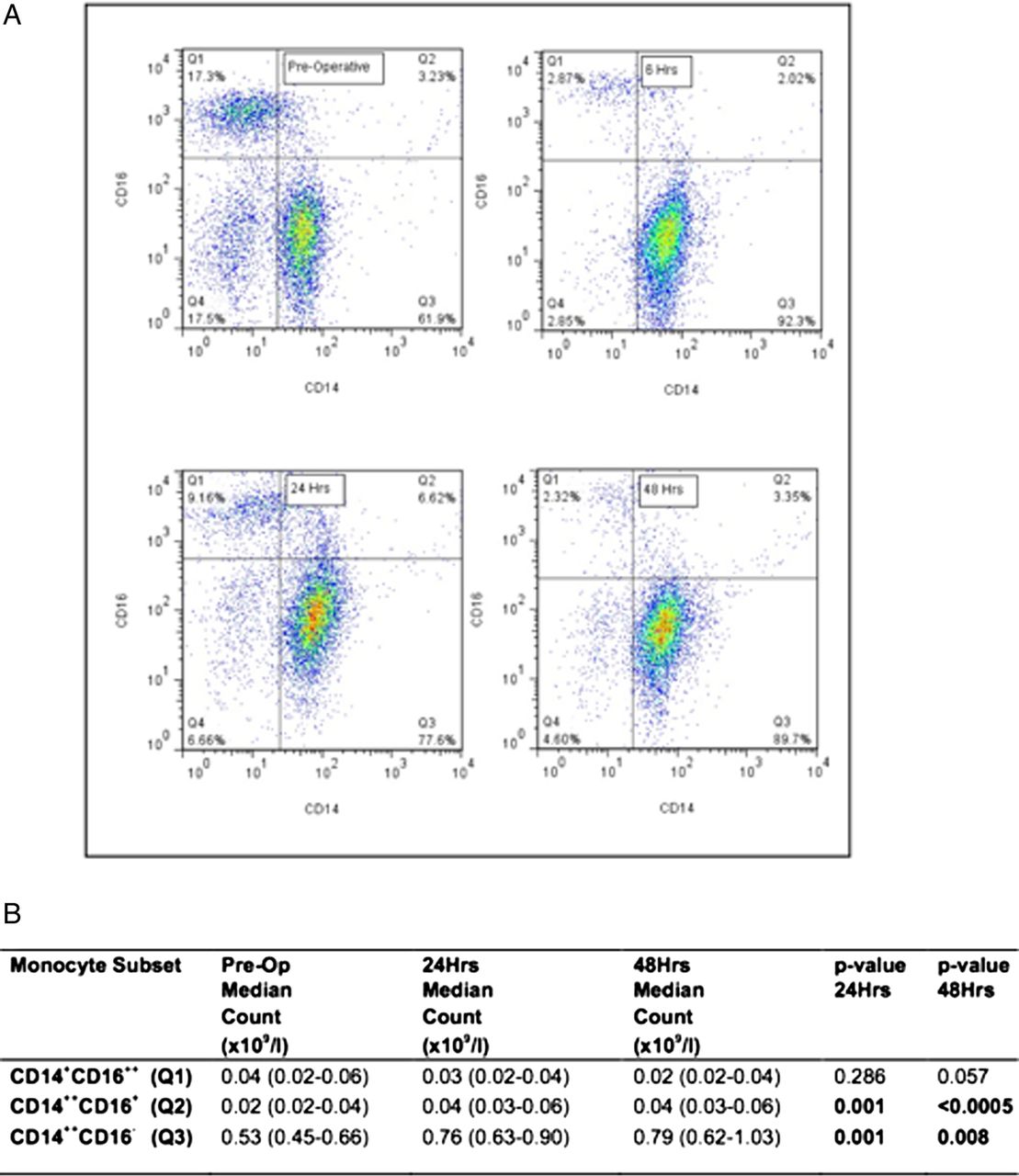
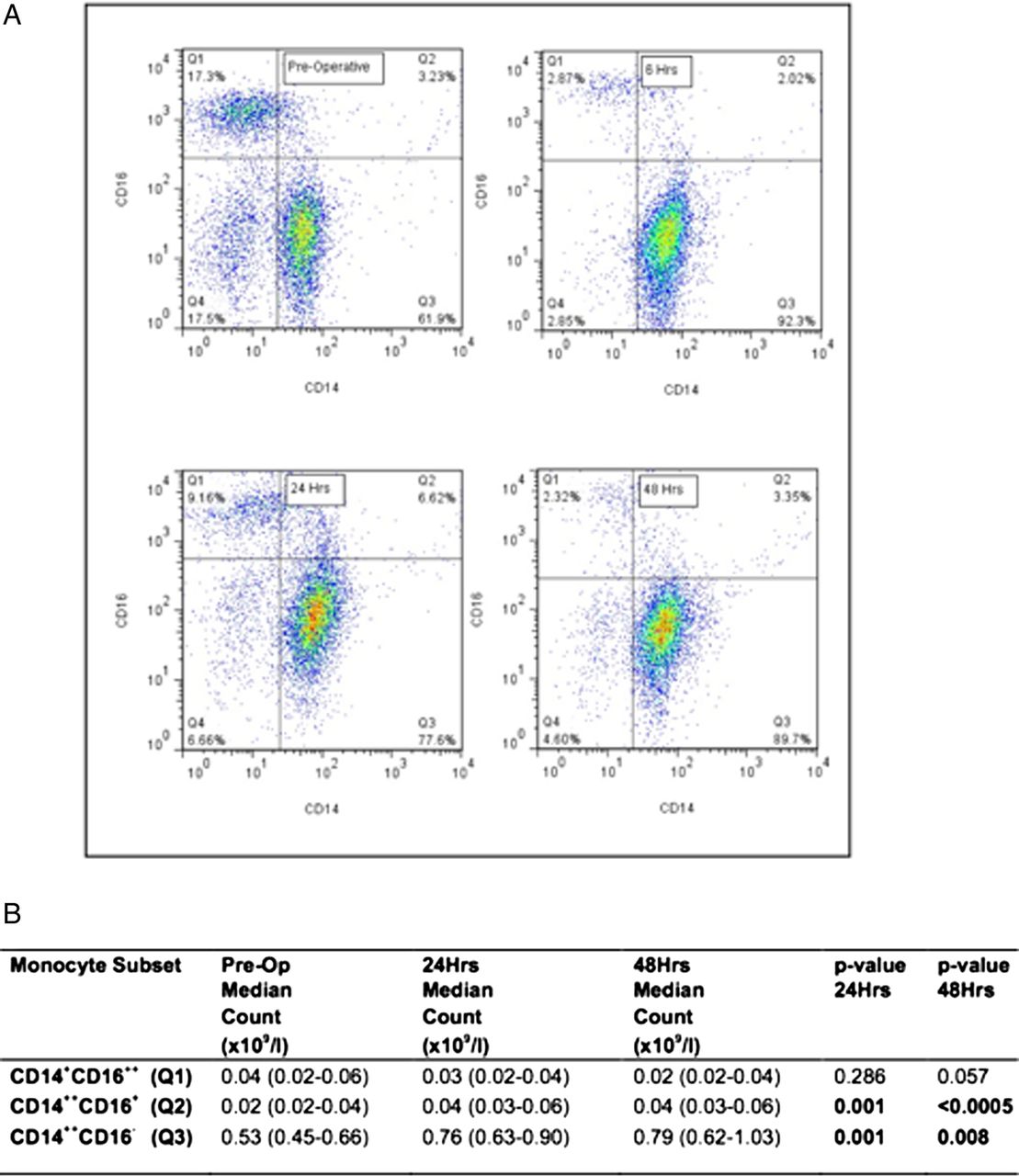{kind=link}
Postoperative changes in blood monocyte subsets. (A) Serial flow cytometry plots from a single representative patient, illustrating the quantification strategy (as outlined in the Methods section). Mononuclear cells were obtained from whole blood subjected to dextran sedimentation and discontinuous percoll gradients. The monocyte population was identified by gating on characteristic forward scatter and side scatter appearances. Within this gate, HLA-DR expressing cells were identified, and in this population staining for CD14 and CD16 defined ‘classical’ CD14++CD16− monocytes (Q3, bottom right quadrant), ‘intermediate’ CD14++CD16+ monocytes (Q2, top right quadrant) and ‘non-classical’ CD14+CD16++ monocytes (Q1, top left quadrant). As an additional quality control, expression of CCR2 and CX3CR1 was assessed, to confirm that the expected expression pattern of these receptors within each monocyte subset was observed. (B) Serial monocyte subset counts in blood. Median values are shown with the IQR in brackets. Paired t tests were used to determine postoperative change, n=39 preoperatively, n=38 at 24 h and n=27 at 48 h.
ANOVA modelling revealed a small but statistically significant postoperative reduction in the phagocytic capacity of neutrophils in suspension (the percentage of neutrophils ingesting 2 or more zymosan particles (expressed as median with IQR in parenthesis) was 84 (73–91) at baseline, 84 (68–90) at 6 h, 79 (64–86) at 24 h, and 79 (63–87) at 48 h; ANOVA for overall trend, p=0.047).
Pulmonary response to lung resection
Surgery was associated with a significant increase in total leucocyte count, total protein and levels of IL-1β, IL-6, IL-8 and IL-10 in BAL fluid retrieved from the contralateral lung in the immediate postoperative period (table 3). No evidence of infection was found in any of the BAL fluid cultures at this time point.
Postoperative changes in BAL fluid
Associations with postoperative pneumonia
Fourteen patients (35%) developed postoperative pneumonia according to the predefined criteria. There was no significant difference in the rate of pneumonia according to which form of surgery was performed (35% in patients undergoing VATS, 36% in patients having thoracotomy). No patients developed ALI/acute respiratory distress syndrome as measured by published criteria.22 The only baseline clinical factor associated with a significant difference between those who did or did not develop pneumonia was the transfer factor for carbon monoxide (60.9% predicted in those who developed pneumonia vs 77.9% predicted in those who did not, p=0.010). Further details of baseline clinical characteristics for these two subgroups are found in the online supplementary section (table S4).
We went on to test whether individual innate immune parameters were associated with the development of postoperative pneumonia (table 4 panel A). In general, serum cytokines were not associated with pneumonia, and where they were, the proportional difference was small. Similarly, neutrophil phagocytosis was not associated with pneumonia. In contrast, preoperative cell counts and elements of monocyte responsiveness appeared to be associated with pneumonia.
Associations with postoperative pneumonia
To test this further, parameters identified in table 4 panel A were used to establish which had a significant relative risk for pneumonia (table 4 panel B). In this setting, relatively higher neutrophils in blood and leucocytes in BAL appeared to be associated with pneumonia. Interestingly, relatively higher anti-inflammatory responses in LPS-stimulated monocytes (IL-12 preoperatively and IL-10 at 24 h) were associated with pneumonia, with IL-6 being the only proinflammatory cytokine to show an association.
Discussion
While several studies have assessed the serum cytokine response after thoracic surgery,23–25 our findings provide a first detailed, serial characterisation of monocyte and neutrophil function after lung resection. Elective surgery provided a particularly useful setting in which to study innate immune characteristics in the lung and blood, given the opportunity to obtain a preoperative baseline. Our data suggest that classical monocytes are mainly responsible for postoperative monocytosis. Intermediate monocytes were also significantly increased, but interestingly non-classical monocytes appeared to be numerically and proportionally decreased relative to baseline, at least as far out as 48 h. Similar numerical changes have been described after stroke.26 The fate of intermediate monocytes in this setting remains to be determined—some evidence exists for this population having inherent plasticity, with the capacity to become classical or non-classical monocytes depending on their environment.27 ,28
We also report a dynamic state of monocyte responsiveness to LPS, with IL-8 secretion increased within 6 h, and a general tendency for a more proinflammatory cytokine responsiveness to LPS at 48 h. The pattern of increased LPS-induced IL-8 secretion from monocytes postoperatively is broadly similar to that described in a smaller study of mononuclear cells from (non-thoracic) surgical patients, though we did not observe the increase in IL-1β described in that study.29 Certainly, our data suggest that, on average, monocytes have a heightened proinflammatory response to LPS in the postoperative period.
In this regard, a number of points are worth making. First, our data suggest that the monocyte response generates proinflammatory cytokines from an early stage. This is broadly reminiscent of the pattern described in serum. Second, it is intriguing that the relative risk for pneumonia was most closely associated with monocyte release of the anti-inflammatory cytokine IL-10 (table 4 panel B). With regard to associations with postoperative pneumonia, ours was very much a pilot, hypothesis-generating study, and as such the sample size was too small (and not designed) to draw conclusions on whether a relative anti-inflammatory postoperative monocyte response is predictive of subsequent pneumonia. Nevertheless, IL-10 is differentially expressed by monocyte subsets,30 and has been implicated in driving monocyte deactivation,31 which in turn is associated with increased risk of infection.12–15
Our data also suggested that higher preoperative total cell counts in BAL (predominantly macrophages) and higher levels of circulating neutrophils are associated with a higher risk of postoperative pneumonia. None of our patients had infection detected in BAL samples preoperatively. It is tempting to speculate that patients with a relatively heightened systemic and pulmonary innate immunity in the preoperative phase are more susceptible to the ‘second hit’ of surgery, and/or to low-level postoperative infective inocula, especially if their monocytes tend to yield a relatively anti-inflammatory profile to inflammatory stimuli. Interestingly, our data did not suggest that neutrophil phagocytosis contributed to risk of infection. While the change in neutrophil phagocytosis postoperatively was statistically significant, and consistent with observations after abdominal surgery,32 the levels of phagocytosis reported here are well within the normal range. This is in striking contrast to the situation in critically ill cohorts of patients, where reduced neutrophil phagocytosis (<50% of neutrophils ingesting 2 or more zymosan particles) is independently associated with increased risk of nosocomial infection.33
A unique opportunity to study early innate responses in the lung was also afforded by this study. Previous studies have described pulmonary inflammation after thoracic surgery using serial BAL.34–36 However, they have generally been confounded by short intervals between sampling, and by relatively small volumes of instillate. The present study overcame these limitations. Our results confirm that the lung contralateral to the operated tumour is inflamed extremely early in the course of thoracic surgery (ie, within the first couple of hours), with increased neutrophil influx and protein leak across the alveolar-capillary membrane. This effect may be partly attributable to one lung ventilation, which has been shown to induce inflammatory effects in the lung.35 One-lung ventilation was used in all patients in this study. Interestingly, only the preoperative BAL cell count appeared to predict postoperative pneumonia (table 4 panel B), and it remains to be determined whether the postoperative inflammatory response in the lung is exaggerated in patients who have a high preoperative cell count in BAL fluid.
We should emphasise again that our analysis of factors associated with postoperative pneumonia in this population was exploratory and hypothesis generating. As described above, the apparent association with the IL-10 release from monocytes is intriguing, but it must be emphasised that this is an isolated finding. There was not a frank CARS response in these patients. The inevitable conclusions are, first, that the contribution of, and dynamic interplay between, proinflammatory and anti-inflammatory cascades are likely to contribute to the pulmonary inflammation observed, and second, that our findings require validation in larger and multicentre cohorts. However, we believe they represent an important first step in this regard, and add to the list of factors potentially associated with complications after thoracic surgery, such as low diffusing capacity for carbon monoxide, certain gene polymorphisms and inflammatory parameters.37–39 Ultimately, this work was based on the expectation that a greater understanding of the innate immune processes associated with postoperative complications may allow stratified approaches to management (based on the expectation of postoperative risk) and/or the evolution of novel strategies for the prevention of complications through manipulation of the innate immune response.
When considering our data on postoperative risk, it must be kept in mind that our definition of ‘pneumonia’ is in the strict sense of ‘alveolar inflammation’, and the radiological consolidation could represent infiltration of inflammatory cells without infection. We did not judge it ethical to request a further routine BAL for microbiological culture in recovering surgical patients. Nevertheless, our criteria for pneumonia were predefined, alveolar shadowing on CXR was judged by an experienced thoracic radiologist, and 8 of the 14 patients with ‘pneumonia’ did have bacterial pathogens isolated from the sputum as part of their routine clinical care. Therefore, while we cannot be certain that all patients with ‘pneumonia’ had bacterial infection, we can be confident that they had alveolar inflammation. It is also important to emphasise that all patients with pneumonia made a good recovery.
In addition, a number of potential limitations should be considered when interpreting our data. Our sample size was small, as we deliberately concentrated on what we believe to be by far the most comprehensive and detailed serial analysis within individual patients in this setting. Our findings provide initial insights but require confirmation in larger cohorts. Also, most of our patients had lung cancer, a burden of tobacco exposure and variable medications including statins, all of which may potentially influence innate immunity. Nevertheless, these factors are likely to be characteristic of, and relatively consistent in, populations of patients being worked up for lung cancer resection, and so the data remain relevant in that specific context. Furthermore, as with all functional studies using neutrophils and monocytes, we cannot be certain that the ex vivo monocyte responsiveness data are representative of biological activity in vivo. In addition, our protocol did not mandate a standardised anaesthetic approach in all patients (anaesthesia was entirely at the discretion of the anaesthetic team). While we are unaware of any significant variations in anaesthetic practice, potential variations could theoretically impact particularly on our BAL data.
In summary, thoracic surgery mobilises circulating classical and intermediate monocytes, and is associated with the release of proinflammatory cytokines from blood monocytes in response to inflammatory stimuli. Monocyte responsiveness to LPS and preoperative levels of leucocytosis appears to be associated with a risk of postoperative pneumonia, but this requires further characterisation and confirmation in larger cohorts.
References
Footnotes
WSW and AJS are joint senior authors.
-
Contributors In addition ROJ designed the study, obtained clinical samples, performed experiments, analysed the data and wrote the manuscript. MB and ACM performed experiments and contributed to the writing of the manuscript. NHA designed and performed statistical analysis and contributed to the writing of the manuscript. JTM independently reviewed chest radiographs and contributed to the writing of the manuscript. WSW and AJS designed the study, analysed the data and wrote the manuscript.
-
Funding The project was funded by a Scottish Chief Scientist's Office research grant (CZB/4/604) and by the Sir Jules Thorn Charitable Trust. In addition, ROJ was supported by the Thoracic Surgery Unit Charitable Funds, Royal Infirmary of Edinburgh.
-
Competing interests AJS has received funds to attend conferences, in relation to travel, registration and accommodation, from GlaxoSmithKline and Astra Zeneca. He has given non-promotional talks for GSK. He is the chief investigator on a grant on which Becton Dickinson Biosciences are co-applicants and is also a principal investigator on grants where the chief investigator is employed by Becton Dickinson Biosciences.
-
Ethics approval The study was approved by the Local Research Ethics Committee (LREC No: 09/S1101/11).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.