Article Text

Abstract
Introduction Acetazolamide (AZM) is used for various conditions (eg, altitude sickness, sleep apnoea, glaucoma), but therapy is often limited by its side effect profile. Our objective was to estimate the risk of commonly reported side effects based on meta-analyses. We hypothesised that these risks are dose-dependent.
Methods We queried MEDLINE/EMBASE (Medical Literature Analysis and Retrieval System Online/Excerpta Medica dataBASE) up until 04/10/2019, including any randomised placebo-controlled trial in which adults received oral AZM versus placebo reporting side effects. Eligibility assessment was performed by two independent reviewers. Data were abstracted by one reviewer who verified key entries at a second time point. For side effects reported by >3 studies a pooled effect estimate was calculated, and heterogeneity assessed via I2; for outcomes reported by >5 studies effect modification by total daily dose (EMbyTDD; <400 mg/d, 400–600 mg/d, >600 mg/d) was assessed via meta-regression. For pre-specified, primary outcomes (paraesthesias, taste disturbances, polyuria and fatigue) additional subgroup analyses were performed using demographics, intervention details, laboratory changes and risk of bias.
Results We included 42 studies in the meta-analyses (Nsubjects=1274/1211 in AZM/placebo groups). AZM increased the risk of all primary outcomes (p<0.01, I2 ≤16% and low-to-moderate quality of evidence for all)—the numbers needed to harm (95% CI; nStudies) for each were: paraesthesias 2.3 (95% CI 2 to 2.7; n=39), dysgeusia 18 (95% CI 10 to 38, n=22), polyuria 17 (95% CI 9 to 49; n=22), fatigue 11 (95% CI 6 to 24; n=14). The risk for paraesthesias (beta=1.8 (95% CI 1.1 to 2.9); PEMbyTDD=0.01) and dysgeusia (beta=3.1 (95% CI 1.2 to 8.2); PEMbyTDD=0.02) increased with higher AZM doses; the risk of fatigue also increased with higher dose but non-significantly (beta=2.6 (95% CI 0.7 to 9.4); PEMbyTDD=0.14).
Discussion This comprehensive meta-analysis of low-to-moderate quality evidence defines risk of common AZM side effects and corroborates dose dependence of some side effects. These results may inform clinical decision making and support efforts to establish the lowest effective dose of AZM for various conditions.
- drug reactions
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
What is the risk of developing one of the common side effects of AZM and are these risks dose-dependent?
What is the bottom line?
The numbers needed to harm for paraesthesias, dysgeusia, polyuria, fatigue ranged from 2 to 18. The risk for paraesthesias, dysgeusia and possibly fatigue increase with higher AZM doses.
Why read on?
Based on a large number of randomised, placebo-controlled trials from multiple disciplines, this article provides precise estimates in clinically relevant terms (number needed to harm) for various side effects including but not limited to the ones mentioned earlier.
Introduction
Acetazolamide (AZM) is a carbonic anhydrase (CA) inhibitor that has been used since the 1950s for various medical conditions.1–7 For example, it is highly efficacious in treating glaucoma,8 9 preventing10–12 -and possibly treating13 acute mountain sickness (AMS); however, side effects are common with some studies reporting an incidence of 80%–100%2 14 (especially paraesthesias, dysgeusia, polyuria and fatigue), which limits patients’ tolerance and compliance.2 15 It has been postulated that some of the side effects may be related to the amount of metabolic acidosis caused by AZM16 (via renal bicarbonate wasting which reaches steady state within 1–2 days17 18) and plasma drug levels that are affected by weight and renal function.19–21 Based on these and other data limited by small numbers and/or observational nature there has been a notion that some of the side effects may be dose-dependent (see online supplementary e-Table 1).11 12 This perception has led to substantial efforts to find the lowest effective dose to prevent AMS for which a review from 2012 suggested 250 mg/day to be similarly effective as 750 mg/day,11 although the number needed to treat was higher for the lower dose (number needed to treat (NNT) 6 (95% CI 5 to 11) vs 3 (95% CI 3 to 5)). Of note, this study provided only very limited, semi-quantitative information about four side effects based on data from five studies. However, informed decision making about whether to use AZM (and if so which dose) is based on weighing potential benefits against risks, and thus requires robust quantitative estimates for each. Furthermore, whether efforts to find the lowest effective dose of AZM for other conditions (eg, idiopathic intracranial hypertension and sleep apnoea) are warranted depends on whether side effects are dose-dependent.
Supplemental material
Our objective is to provide precise estimates for the risk of developing one of the common side effects of AZM and to assess systematically whether this risk is dose-dependent. We assumed that the risk of most AZM side effects—unlike efficacy—is independent of the underlying condition for which it is used for and thus pooled data from trials using AZM for various conditions; we formally tested this assumption via meta-regression (see results).
Methods
This review was performed according to a pre-specified study protocol (online supplementary e-Appendix 1) and following PRISMA-reporting guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).22
Supplemental material
Patient and public involvement
Patients were not involved in the design or execution of this study.
Identification of studies
We considered any randomised controlled trial (RCT) in which adult subjects were randomised to oral AZM versus placebo reporting side effects. We excluded trials with subjects who were non-human, non-adult, unable to report side effects reliably (eg, intubated), receiving haemodialysis (rationale: substantial impact on pharmacokinetics; high prevalence of dysgeusia, paraesthesias/neuropathy, fatigue; inability to assess polyuria); we further excluded trials lacking information about side effects, administering AZM as a non-PO formulation (eg, intravenously/inhaled), or giving AZM only in combination with another systemic intervention (precluding isolated assessment of the AZM effect).
We searched MEDLINE and EMBASE from inception until 04/10/2019, and reviewed reference lists of eligible and other seminal articles. The final search strategies were:
MEDLINE: (Acetazolamide(Mesh) OR Acetazolamide(tiab)) AND (Randomised Controlled Trial(ptyp) AND Placebo)
EMBASE: (‘acetazolamide’:ti,ab,kw OR ‘acetazolamide’/exp) AND (‘placebo’:ab,ti OR ‘placebo’/exp) AND (‘randomized controlled trial’/de)
We did not place any language restrictions. We contacted the authors of two foreign language articles23 24 without success, but subsequently were able to determine the ineligibility of these reports with the help of native speakers (see acknowledgements section).
Eligibility assessment and data abstraction
Titles and abstracts of retrieved records were screened independently by two authors (CNS and AM) with final eligibility assessment based on full-text articles applying above inclusion/exclusion criteria (disagreements resolved by discussion). Data from eligible studies were abstracted by CNS using a piloted Microsoft Excel form. To minimise the risk for data abstraction errors we utilised drop-down lists in Excel whenever possible and double-checked all abstracted key data points at a second time point. We further employed sensitivity analyses to assess the impact of any decisions made during these stages (eg, imputation of zeroes in placebo arms of studies that only reported adverse events for the AZM group).
Abstracted data included demographics of study participants (eg, age, gender, body mass index (BMI)), intervention details (eg, AZM dose, days of administration, adjustment for renal function),19 pertinent labs (eg, pH,16 pCO2/HCO3,19 chloride)20 and side effects (primary outcomes: paraesthesias, dysgeusia, polyuria, fatigue). For a full list of variables and their definitions see the study protocol (online supplementary e-Appendix 1) and the data set (online supplementary e-Table 2). For each side effect we collected the number of subjects who experienced that side effect at any time during the study’s observation period versus those who did not in the AZM versus placebo group; for laboratory tests we collected the mean value in the AZM versus placebo arms (following study drug administration, ie, ignoring change from baseline).
Supplemental material
Risk of bias assessment
Risk of bias was assessed as either low, high or unclear across five domains (selection, performance, detection, attrition, reporting) at the study level but the focus was on risk of bias with regard to the reported side effects, not the primary outcomes of the studies. Overall risk of bias was defined as the ‘highest’ level of bias across these five domains; its effect on the results was assessed by checking for significant effect modification via meta-regression.
Statistical analysis
Data preparations: Placebo arms that served as comparator for two AZM arms with different doses were divided evenly into halves to avoid double-counting of the control group (unit of analysis error) while allowing assessment of effect modification by AZM dose.11 25 Studies that clearly stated that no events occurred in both the AZM and control arm were included into the primary analysis by adding a continuity correction of 0.5 to all cells (rationale: assuming dose dependency of side effects, low-dose AZM studies are more likely to have zero events in the intervention arms than high-dose AZM studies, while zero events in placebo arms are equally likely to occur in low and high-dose studies; thus exclusion of studies with zero-events in both arms would preferentially exclude low-dose trials and bias the risk estimate in low-dose AZM trials upwards, thereby reducing power to detect dose dependence).26
Risk of side effects: For all side effects reported by three or more studies we calculated a pooled effect estimate using Mantel-Haenszel methodology (rationale: we used fixed rather than random effects model to avoid small study bias). All analyses were performed using ORs due to their favourable mathematical properties compared with risk ratios; however, to aid interpretability, final results are also reported as risk ratios (calculated directly from the ORs as RR=OR/(1−ACR *(1−OR)) where assumed control risk (ACR) is estimated from the overall event rate across placebo arms) and NNT (NNT=1/|ACR−((OR*ACR)/(1−ACR+OR*ACR))|).25 27 Heterogeneity was quantified by the I2 statistic and arbitrarily categorised as low (<30%), moderate (30%–50%) or high (>50%)25 28; in case of I2 >30% attempts were made to identify and adjust for sources of heterogeneity, and a random effects model was used instead (if I2 remained >30%).
Subgroup analysis: Dose dependency was assessed for all outcomes with a pooled effect estimate based on five or more studies by testing for effect modification by total daily dose via meta-regression (one study29 reported a total daily dose of 2500 mg/day vs 125–1000 mg/day in all others; to avoid results to be driven by this outlier we divided the total daily dose into a three-level categorical variable for the primary analyses [ie <400 mg/day, 400–600 mg/day and >600 mg/day were picked to include commonly used doses while dividing studies in roughly equal numbers]). In addition, in sensitivity analyses we also assessed dosage as a linear variable. For primary outcomes (paraesthesias, dysgeusia, polyuria, fatigue) we further assessed effect modification by days of AZM administration, cumulative dose, patient/study characteristics, as well as changes in laboratory tests.
Extensive sensitivity analyses were performed to assess robustness of results for primary outcomes (eg, exclusion of studies with zero events in both arms and changes in model parameters). Publication bias was assessed via funnel plots and Egger’s test.
All analyses (including tests for publication bias) were performed using STATA V.12.1 (StataCorp) with p<0.05 denoting statistical significance.
Quality of evidence assessment
Quality of evidence for primary outcomes was assessed following Grading of Recommendations Assessment, Development and Evaluation guidelines.
Results
Included studies
We identified a total of 53 studies6 15 29–77 reporting one or more side effects (figure 1). Seven references were identified through the search of reference lists (567 68 78–80 from,12 181 from,82 and 13 from83; only 267 68 of these 7 met eligibility criteria and were included in this review). Two articles6 42 reported two treatment arms administering different AZM doses versus a placebo control; thus each report contributed two studies for analyses. Table 1 provides an overview of the 42 studies included into quantitative analyses: about one third of participants in included trials were females, with a wide range of mean age (19–74 years) and BMI (20–40 kg/m2); race was only reported in five studies in which the majority of subjects were white (79% vs 16% black vs 5% other). The majority of studies assessed the impact of AZM on acute/chronic mountain sickness (48%), intraocular pressure (17%), or sleep disordered breathing (SDB, 10%), with remainder of conditions varying widely. About half of the studies queried the side effects actively and were judged as low (24%) or unclear (33%) risk of overall bias. On average, there were 30 participants in each AZM arm (range 6–118), receiving 542 mg of AZM per day (range 125–4000 mg) for a total of 17 days (range 1–180 days). Renal function was taken into account by one third of trials, and 7% of trials provided some form of potassium supplementation (online supplementary e-Table 2 in the online supplement provides the full data set).
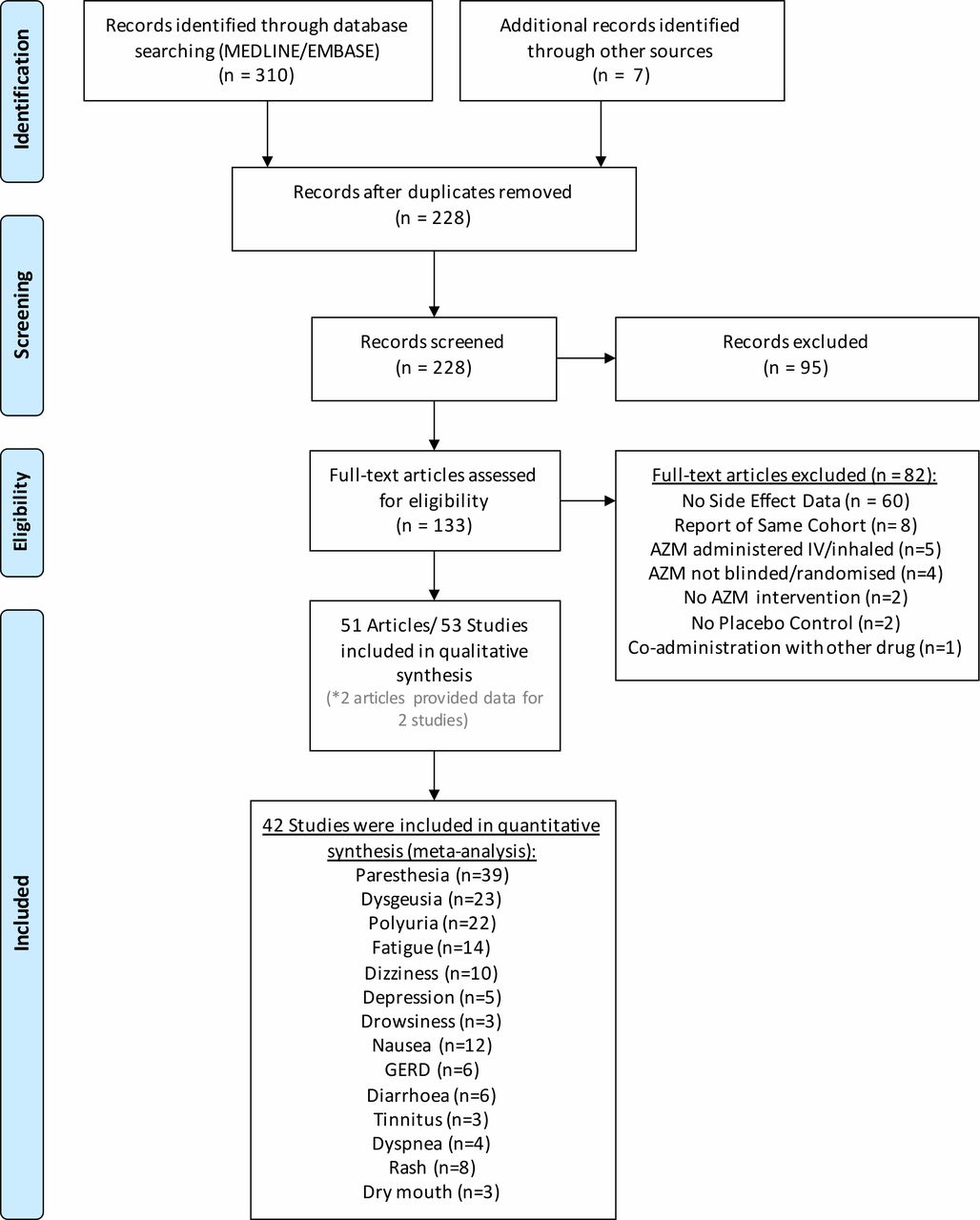
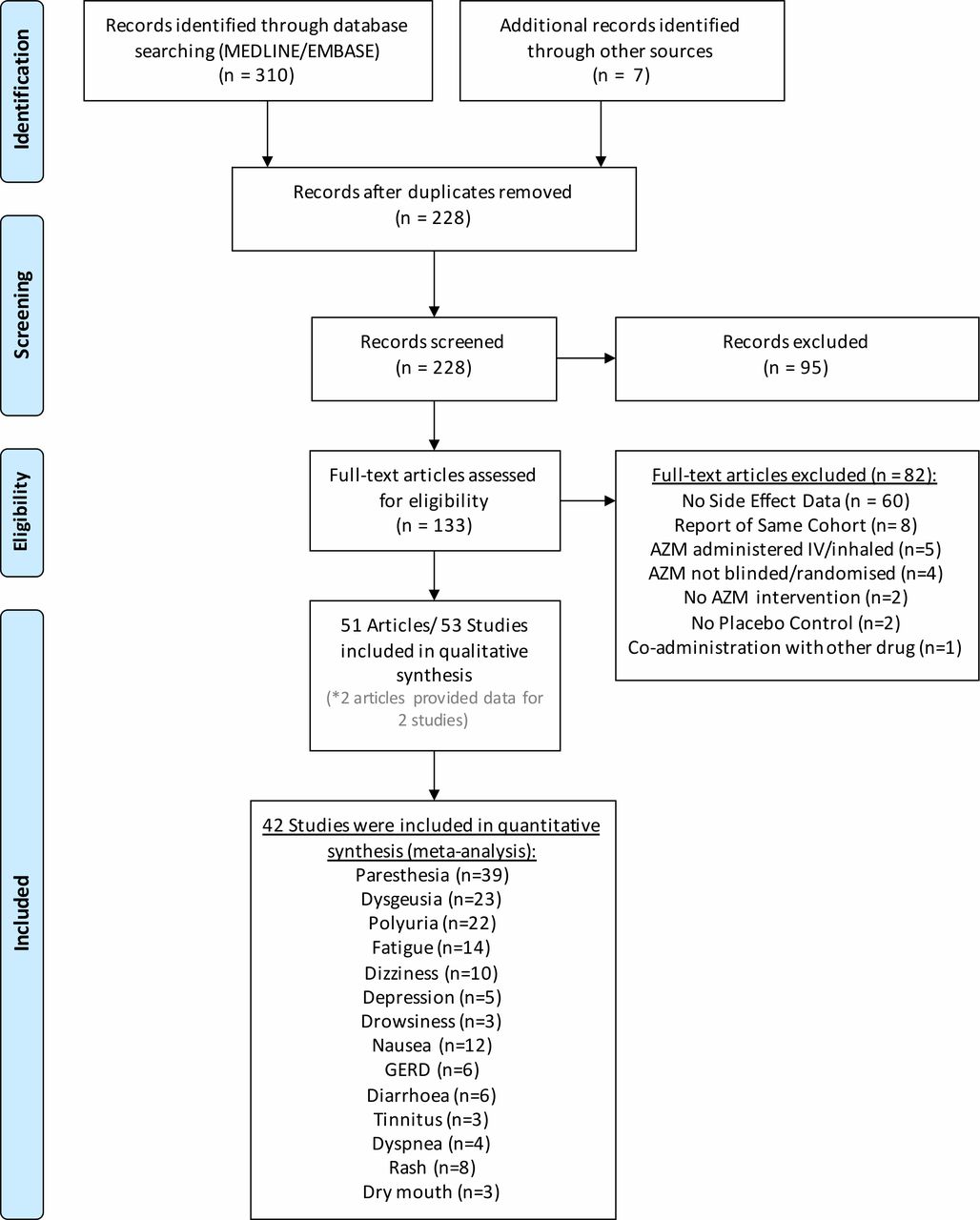{kind=link}
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart.22 Most included studies provided data for several side effects. Seven records were identified by screening reference lists from eligible and seminal articles; two reports each provided data about two studies (for details see the text). AZM, acetazolamide; GERD, gastro-oesophageal reflux disease.
Characteristics of studies included into quantitative analyses (n=42)
Primary outcomes
AZM increased the odds for all the primary outcomes (paraesthesias,6 15 29–34 37–46 48–57 59 60 62–68 dysgeusia,6 29 31 32 35 37 38 42–46 50 52 55–58 64 68 polyuria6 29 32 34 37 38 40 42–45 51 52 54 55 58 61 62 67 68 and fatigue29 31–33 35 48 50 52 54–58 68) by 1.9–12.3 times (low-to-moderate quality of evidence). For paraesthesias, dysgeusia and fatigue the odds of side effects increased by 2–3 fold for each 1-step increase in total daily dose across the three categories (400 mg vs 400–600 mg vs >600 mg) in meta-regression; however, the CI for fatigue included the ‘null’ of no increase in side effects with higher doses. There was no evidence for dose dependency of polyuria (table 2 and online supplementary e-Appendix 2).
Supplemental material
Risk of side effects (based on OR). Dose dependency was assessed by checking for effect modification by total daily dose and was only significant for paraesthesias and dysgeusia. There was a trend towards higher odds for fatigue, but this relationship did not reach statistical significance. ORs were chosen a priori as the effect measure for primary analyses due to the favourable mathematical properties, but to aid interpretation table 4 shows results translated into risk ratios and numbers need to treat
Supplemental material
In further subgroup analyses, the odds of side effects were 1.5–4 times higher in studies querying symptoms actively versus unclear/passively, but only the CI for dysgeusia excluded the null. There odds for fatigue were 1.4 times higher per 10% increase in the percentage of females but the CI was wide (0.9–2.1); furthermore, with the exception of paraesthesias odds were slightly higher with increasing AZM duration/cumulative dose but effect sizes were small and CIs all included the null (table 3). Of note, there was no evidence of effect modification by risk of overall bias.
Results from subgroup analysis. These pre-specified analyses were only performed for the four primary outcomes. The only significant effect modification was query type for dysgeusia (ie, the odds of dysgeusia were higher in trials querying actively vs unclear/passively for symptoms)
The number needed to treat for harm (ie, number of patients needed to be treated for one additional patient to be harmed)27 ranged from 2.3 for paraesthesias to 18 for dysgeusia (table 4). Results were robust based on various sensitivity analyses and there was no evidence of publication bias (Egger’s p>0.05 for all; online supplementary e-Appendix 2).
Risk of side effects expressed as RR and NNTH
Secondary outcomes
AZM increased the odds of nausea,29 35 43 50–54 57 61 62 68 gastro-oesophageal reflux disease,29 38 40 52 67 68 diarrhoea29 35 44 52 67 and depression29 44 52 57 68 by 2.6–4 fold. Furthermore, AZM increased the odds of drowsiness,52 54 64 tinnitus,29 44 48 dyspnoea29 43 53 67 and dry mouth29 48 52 by 2.3–4.7 fold but the lower confidence limit just included the null; rash29 42 44 45 48 52 54 and dizziness29 30 35 38 44 50 53 61 64 68 were slightly more common in AZM groups (ORs 1.7 and 1.2, respectively) but CIs were wide and included the null. There was no evidence of dose dependence for any of the secondary outcomes, but analyses were limited by small numbers of trials (n=5–12; table 2). The number needed to treat to cause one additional secondary side effect ranged from 12 for diarrhoea to 100 for dizziness (table 4). Side effects that were reported in less than three studies are shown in online supplementary e-Table 3: most notably hypokalaemia was reported in two studies29 48 (daily dose 500–4000 mg) occurring almost exclusively in the setting of concomitant therapy with hydrochlorothiazide or valsartan29; furthermore, two studies35 47 reported cases of metabolic acidosis but patients in both studies were hospitalised and relatively ill (acute respiratory failure or cryptococcal meningitis). Other laboratory changes reported in the literature were rare (one case of severe transaminitis29 and one case of ‘hematologic dyscrasia’ characterised by dropping white blood cell counts),29 but most studies did not routinely monitor blood tests. Interestingly, one study reported leuconychia in the setting of AZM plus naproxen at high altitude.77 Furthermore, online supplementary e-Table 3 provides a qualitative summary of four studies70 72–74 that overall suggest that AZM reduces exercise tolerance and endurance (which were assessed by very different methods precluding meaningful pooling of results).
Supplemental material
Discussion
This comprehensive meta-analysis of low-to-moderate quality evidence defines the risk of common AZM side effects and corroborates the adverse effects paraesthesias, dysgeusia and possibly fatigue are dose-dependent. Severe side effects were rare and largely confined to subgroups of patients: that is, hypokalaemia almost exclusively in patients on thiazide diuretics or angiotensin-receptor blockers29 48 which is consistent with reports from non-included studies,14 16 metabolic acidosis in ‘sicker’ hospitalised patients,35 47 dyspnoea in patients that have already an increased work of breathing due to their underlying condition43; two deaths in critically ill patients receiving AZM in the setting of underlying HIV/cryptococcal meningitis, and one case of severe transaminitis without clear risk factor.29
These data are important for a number of reasons: (1) clinical decision making is based on weighing both risks and benefits, but most published reports focus on the latter thus introducing a bias in favour of using interventions.84 85 To this end our study directly complements the results of a review in the BMJ11 assessing the efficacy of AZM for preventing AMS, and enables a balanced assessment of AZM’s value across the many conditions that it is being used for. (2) Our results provide guidance for clinicians about which AZM side effects may be avoidable by starting of low-dose AZM, or—once occurred—may respond to dose reduction. (3) Substantial work went into establishing the lowest effective AZM dose for preventing AMS11 42 86; our findings validate these efforts, and more importantly provide a strong rationale to establish the lowest effective dose for other conditions as well.
Many side effects are subjective and thus vulnerable to a placebo effect as supported by the high event rates in placebo arms noted. To address this issue we restricted our review to placebo-controlled trials; nonetheless our pooled estimates for common side effects are overall very consistent with reports from observational studies.2 16 However, we failed to confirm effect modification by factors reported in the literature (eg, renal function,19 21 weight,21 race,2 or lab changes)16 20; likely reasons include frequently missing data for these covariates, low power of meta-regression in cases of few (<10) included studies, risk for ecological fallacies when assessing patient-level factors87 and the observational nature of meta-regression (ie, potential for confounding). The latter issue also poses a potential threat to our findings of dose dependence for paraesthesias, dysgeusia and possibly fatigue, but our results are supported by several observations: (1) two placebo-controlled trials randomising patients to 250 mg versus 500/750 mg reported relatively more paraesthesias and dysgeusia in the higher dose AZM arm (results for polyuria were mixed; fatigue was not assessed).6 42 (2) AZM’s pharmacodynamic effects vary with dose18: at 1–5 mg/kg (approximately 125–350 mg) AZM mainly affects renal CA (resulting in a metabolic acidosis due to bicarbonate wasting with a compensatory increase in steady-state ventilation, likely a key factor for preventing AMS18 and improving SDB),14 88 endovascular CA (slightly increasing tissue acidosis and the arterial-alveolar carbon dioxide (CO2) gradient) and peripheral chemoreceptor CA (reducing response rate to CO2 fluctuations, which may be another important mechanism through which AZM improves SDB).89 At higher doses of 7–20 mg/kg (approximately 500–1400 mg) AZM increasingly inhibits intracellular CA in non-renal tissues such as erythrocytes and the brain resulting in progressively worsening gas exchange and tissue acidosis; while these additional effects may be desirable to some degree in select patients, for example, to augment further steady-state ventilation via acidification of tissue surrounding central chemoreceptors in the brain, they likely also mediate some of the side effects.20 The fact that renal CA is fully inhibited with small doses (<400 mg) likely explains why there is no further increase in polyuria incidence with doses beyond that. Similarly, in some but not all cases fatigue may be a result of the metabolic acidosis (secondary to bicarbonaturia due to renal CA inhibition) possibly explaining the lack of clear dose dependence in our analysis. Support for this comes from a study in which 15 of 24 glaucoma patients with a malaise complex (including fatigue, nausea, anorexia, depression, loss of libido) experienced partial or full relieve with sodium bicarbonate to treat the underlying acidosis.16 However, while for some conditions the acidosis is just a side effect (eg, glaucoma) for others it mediates the therapeutic effect (eg, AMS) and caution is warranted as this study was uncontrolled, unblinded and changes in plasma bicarbonate levels did not predict response. Independent of dose, AZM may irritate gastric mucosa as some of the gastrointestinal side effects seem to improve when AZM is taken with food,16 which may explain lack of dose dependence for nausea in our study (although the odds of gastro-oesophageal reflux disease may increase with higher doses). (3) Our results are largely consistent with findings in two systematic reviews of AZM for the prevention of AMS, both of which only assessed a few select side effects (paraesthesia, dysgeusia, polyuria in both; rash in one) semi-quantitatively and were limited by relatively small numbers of included studies,11 12 as well as another systematic review10 that reported similar risk of paraesthesia (but reported no data for other side effects). Another major limitation is that we may have missed some eligible studies by restricting our search query to only two databases. Regardless of this restriction several of our observations are reassuring: (1) we queried the two most widely used databases for medical research; (2) extensive review of reference lists including those from systematic reviews including other databases only revealed two additional eligible studies; (3) formal testing did not reveal significant evidence of publication bias.
Strengths of our study include meta-analyses based on large numbers of studies, evaluation of a wide range of side effects and robustness of results in extensive sensitivity analyses. One of the limitations of our study is that some of the side effects may vary over time63 90; however, we did not find statistically significant effect modification by AZM duration and the primary data did not allow for a more detailed time-to-event analysis. Furthermore, one of the premises of this study was that AZM side effects can limit effective therapy by reducing compliance, which is likely a complex decision making process involving type of side effect, severity, efficacy but also psychosocial factors such as partner support and coping skills.91 The primary data did not allow meaningful analyses of the relationship between side effects and compliance as in most studies it was unclear if loss to follow-up or AZM discontinuation was due to a side effect. However, several observations support this notion, for example in one of the included RCTs patients with paraesthesias were 2.5 times more likely to miss AZM doses (21% vs 8%, p=0.04)15 and some studies administering AZM 500–1000 mg/day report discontinuation rates due to side effects ranging from 26% to 35% (primarily due to fatigue and gastrointestinal symptoms rather than paraesthesias),2 16 48 contrasting with another study in which only 8% (7/86) of patients were unable to tolerate a minimum dose of 125 mg/day (ie, 92% were able to tolerate at least a very low dose of 125 mg for 6 months).29 Moreover, our study does not provide an answer as to how many patients experience any versus no side effects with AZM, because side effects tend to cluster20 and few studies report this information. In one study in which patients received a mean AZM dose of 2500 mg, 83% experienced at least one side effect with a median number of side effects per person of 5 (IQR 1–22). Another potential limitation is that only one third of included studies used a cross-over (vs parallel group) design in which subjects served as their own controls. Finally, except for two studies35 47 of hospitalised patients, our results are based on relatively healthy subjects treated in the outpatient setting and may thus not generalise to ‘sicker’ populations; furthermore, based on the number of included patients in this review, our ability to detect side effects was limited to events occurring about 1/1000 patients. Similarly some side effects may be missed if they occur only in certain conditions: for example, in select patients with central sleep apnoea AZM may convert central to obstructive apnoeas with worse hypoxaemia92; in patients with reduced pulmonary reserve (eg, severe chronic obstructive pulmonary disease) AZM-induced increase in work of breathing may cause shortness of breath or even respiratory failure; in cirrhotic patients AZM may result in encephalopathy, and in subjects with reduced renal function (eg, elderly, diabetics) impaired drug clearance may result in side effects usually only seen with high-dose AZM such as severe metabolic acidosis. Also, other side effects such as nephrolithiasis (possibly responsive to citrate supplementation) or weight loss may have been under-detected due to the generally shorter observation period in randomised trials versus observational studies. More details about such potentially severe side effects in specific situations can be found in two recent reviews.93 94
While this review focused on AZM, many of the findings may apply to other CA inhibitors such as methazolamide, ethoxzolamide, topiramate, zonisamide and occasionally even with topical drugs like dorzolamide.93 95 However, CA is ubiquitous across the human body and at least 13 different isoforms of CA exist. Thus, predicting the effects of CA inhibitors is complex,18 93 and small molecular changes between CA inhibitors may result in big differences in efficacy and side effects. Furthermore, each drug may have effects independent of CA inhibition. For example, compared with AZM, methazolamide has a similar affinity for the different CA isoforms but is more lipophilic, appears to have different effects on ventilation96 and may be better tolerated.97 98 Nonetheless, more research is needed to assess if (and how) such differences may translate into clinical care. Such research will have to take into account the different pharmacodynamic and kinetic effects relevant to CA inhibition (eg, access of drugs to the target tissue, concentration of CA isoforms in the target tissue and the degree to which uncatalysed CA reactions contribute to the function that is targeted),99 which will differ depending on the condition of interest.
Conclusion
The most common side effects of AZM are paraesthesias which may reduce therapy compliance but—based on the literature—appear less likely to result in complete therapy termination than other common side effects such as fatigue and gastrointestinal symptoms. Paraesthesias, dysgeusia and possibly fatigue are likely dose-dependent phenomena and may thus be avoidable by using low-dose AZM and respond to dose reduction; on the other hand, some gastrointestinal symptoms may reflect local irritation and thus be ameliorated by administering AZM with food. In select cases, side effects may alternatively be mitigated by use of an alternative CA inhibitor or bicarbonate supplementation. Severe side effects are rare and can largely be avoided by careful patient selection (eg, hypokalaemia occurs almost exclusively in patients co-treated with thiazide diuretics or angiotensin receptor blockers). This review complements data about AZM efficacy, thus facilitating a more balanced assessment of AZM’s clinical value. Observed partial dose dependence further supports efforts to establish the lowest effective AZM dose for the various conditions in which it is used (which likely rely on different pharmacodynamic effects); thus different conditions may require different doses.
Acknowledgments
We would like to thank Dr Jinghong Li and Dr Kamyar Afshar for their help with evaluating two foreign language articles considered for this review.
References
Footnotes
Contributors CNS serves as guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish. CNS further attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. CNS contributed to design, data acquisition, analysis, interpretation of the data and drafting of the manuscript. AM contributed to data acquisition, interpretation of the data and made critical revisions to the manuscript. RLO, JO and BAE contributed to interpretation of the data and made critical revisions to the manuscript.
Funding CNS is supported by the National Institutes of Health T32 grant HL134632. This study did not have any specific funding.
Competing interests CNS and JO have nothing to declare. RLO reports personal fees from Novartis, outside the submitted work. BAE reports grants from Heart Foundation of Australia, during the conduct of the study; grants from National Health and Medical Research Council of Australia, other from Apnimed, outside the submitted work. As an Officer of the ATS, AM relinquished all outside personal income since 2012. ResMed provided a philanthropic donation to UC San Diego in support of a sleep centre.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data are reported in e-Table 2.