Article Text

Abstract
Introduction Central airway obstruction (CAO) is a life-threatening complication of lung cancer. The prevalence of CAO in lung cancer patients is unknown. We audited CAO burden to inform our local cancer service.
Methods This is a cohort review of all new lung cancer diagnoses between 1 November 2014 and 30 November 2015. CAO was defined by CT appearance. CT scans and routine patient records were followed up to 30 November 2018 to determine the prevalence of CAO at diagnosis; the characteristics of patients with prevalent CAO; mortality (using survival analysis); and incident CAO over follow-up.
Results Of 342 new lung cancer diagnoses, CAO prevalence was 13% (95% CI 10% to 17%; n=45/342). Dedicated CT scan review identified missed CAO in 14/45 (31%) cases. In patients with prevalent CAO, 27/44 (61%) had a performance status of ≤2, 23/45 (51%) were diagnosed during an acute admission and 36/44 (82%) reported symptoms. Treatments were offered to 32/45 (71%); therapeutic bronchoscopy was performed in only 8/31 (26%) eligible patients. Median survival of patients with prevalent CAO was 94 (IQR 33–274) days. Multivariate analysis, adjusting for age, gender and disease stage, found CAO on index CT scan was independently associated with an increased hazard of death (adjusted HR 1.78 (95% CI 1.27 to 2.48); p=0.001). In total, 15/297 (5%) developed CAO during follow-up (median onset 340 (IQR 114–551) days). Over the audit period, 60/342 (18%; 95% CI 14% to 22%) had or developed CAO.
Discussions This is the first description of CAO prevalence in 40 years. Patients with prevalent CAO had a higher mortality. Our data provide a benchmark for service planning.
- bronchoscopy
- clinical epidemiology
- imaging/CT MRI etc
- lung cancer
- non-small cell lung cancer
- small cell lung cancer
- thoracic surgery
- palliative care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- bronchoscopy
- clinical epidemiology
- imaging/CT MRI etc
- lung cancer
- non-small cell lung cancer
- small cell lung cancer
- thoracic surgery
- palliative care
Key messages
We audited the prevalence and outcomes of central airway obstruction (CAO) in patients at presentation with a new diagnosis of lung cancer and over a 4-year follow-up period.
We found CAO is present in one in eight patients with a new diagnosis of lung cancer, with a further 5% developing CAO during follow-up.
CAO is associated with poor survival when adjusted for age, gender and stage of cancer, and defining optimal care for these patients needs addressing.
Background
Lung cancer is the leading cause of cancer mortality and the second most common cancer diagnosed in the UK, with >40 000 new cases per year.1 Of these, nearly 80% of patients present with advanced stage disease where treatment options are limited, performance status may rapidly decline and palliation becomes the focus of care.
Central airway obstruction (CAO) is defined as any disease process affecting the trachea, right and left main bronchus, or bronchus intermedius on imaging or by direct visualisation at bronchoscopy. It is estimated that 20%–30% of patients with lung cancer have CAO, and 40% of deaths are attributed to progressive loco-regional disease.2 3 These estimates date back >40 years, and therefore may not reflect contemporary lung cancer epidemiology.3–7 Further, in the UK, national audits of CAO treatment are not performed and therefore the burden of disease and quality of services is largely unknown. Therefore, we undertook an audit to determine the burden of CAO caused by primary lung cancer at a tertiary referral centre to guide service development within our cancer network.
Methods
Audit site and population
This cohort review of primary lung cancer patients, using routinely collected clinical, radiological and histological information, was conducted at a large teaching hospital that serves a secondary care population of 450 000 people. In addition, this centre serves as a tertiary referral centre for thoracic surgery.
Inclusion/exclusion criteria
All patients directly referred to the hospital lung cancer service and diagnosed with primary lung cancer between 1 November 2014 and 30 November 2015 were included. Patients referred from secondary centres were excluded. Patient follow-up was censored on 30 November 2018.
Audit procedures
All data (clinical, radiology and histology information from patient records) were collected on standardised forms. Information on baseline demographics, disease stage defined by the multidisciplinary team (MDT; Tumour Node Metastases classification seventh edition) and tumour histology were collected. Date of death (from all causes), where applicable, was recorded from hospital record systems.
All index staging thoracic CT scan reports were reviewed to record the presence or absence of endobronchial disease or CAO. Following this, all CT scans (both index and follow-up) underwent a focused review of the central airways. This was conducted by an interventional pulmonologist to identify unreported CAO at diagnosis and any new CAO that subsequently developed during patient follow-up. A thoracic radiologist verified all unreported CAO identified on index CT scans. Any discordance was agreed through discussion and consensus.
In patients with CAO, clinic letters, discharge summaries and MDT notes were used to determine symptoms, WHO performance status and to identify interventions performed. In addition, in patients with CAO, flexible bronchoscopy records were reviewed if available.
Definitions
CAO was defined as an identifiable narrowing of the central airways due to lung cancer, on cross-sectional imaging. The degree of CAO was estimated using CT scans and defined as the ratio of the diameter of the narrowest section of obstructed airway to the nearest proximal normal segment of the tracheobronchial tree. Severe CAO obstruction was defined as an obstruction of >50%. Disease was further defined as being predominantly intrinsic (evidence of endobronchial disease), extrinsic (external compression), or mixed in origin. Viable distal lung was defined as the presence of aerated distal lung on imaging. Cases suitable for therapeutic bronchoscopy were defined as having severe CAO and viable distal lung.
Statistical analysis
Data were analysed using SPSS (V.24). Continuous data are presented as median and IQR and categorical data as frequencies and proportions. Medians were compared using the Wilcoxon rank sum and Kruskall Wallis test. Proportions were compared using the Fisher’s exact test. The prevalence of CAO was determined as the proportion with CAO on the index CT scan. The incidence risk of CAO was determined as the proportion without CAO on the index CT scan, who developed CAO over the follow-up period of the cohort.
To explore the mortality rate in the cohort, for each patient the total follow-up time was calculated from the date of lung cancer diagnosis to the earliest of (1) the date of death (2) the date of transferring out of the lung cancer service (for any reason other than death) or (3) 30th of November 2018. Kaplan-Meier curves were used to summarise time to death, by CAO status (on index CT scan). Univariate and multivariate Cox regression was used to explore the association between CAO on index CT scan and time to death. HR and adjusted HR (aHR) with 95% CI were estimated, with p values from the likelihood ratio test.
Ethics
This was part of a service evaluation of the local burden of disease and outcomes, to inform on service structuring, management pathways, performance and the development of standards for auditing. Therefore ethical approval was not required.
Patient and Public Involvement
Patients and public were not involved in this audit of practice.
Results
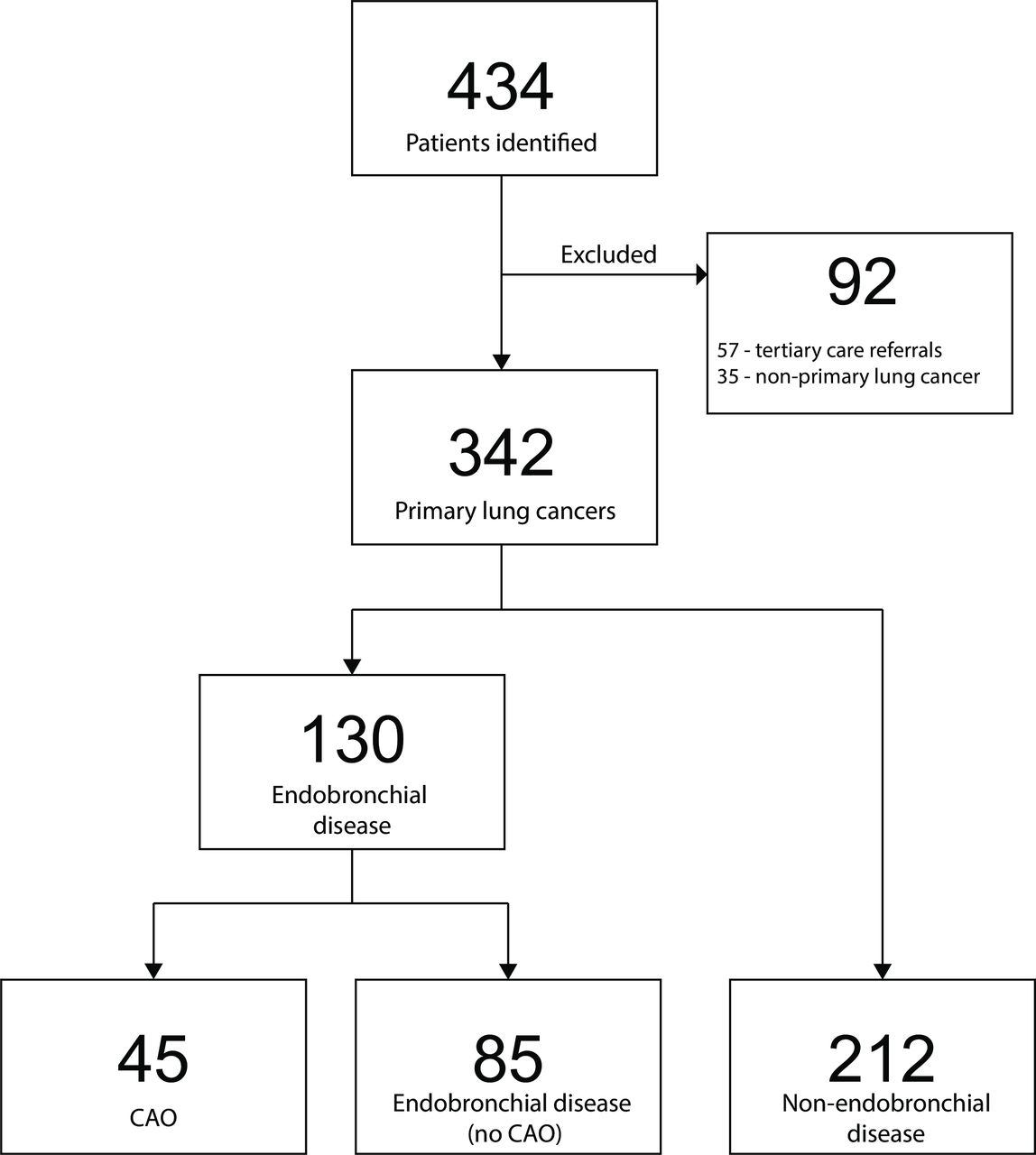
In total, 434 patients were coded as having a thoracic malignancy between 1 November 2014 and 30 November 2015; of these 342 (79%) were locally referred index primary lung cancer patients (figure 1). The median age of patients was 72 (IQR 65–78) years and females accounted for 163/342 (48%) of cases (table 1). A histological diagnosis was obtained in 242/342 (71%); non-small cell lung cancer adenocarcinoma (NSCLC-ad) was the the most common, accounting for 132/242 (55%) of cases. Stage I or II disease was present in 105/342 (31%) of cases.
Demographic, histology and follow-up data for n=342 patients admitted between 1 November 2014 and 30 November 2015 with primary lung cancer, by index CT scan findings
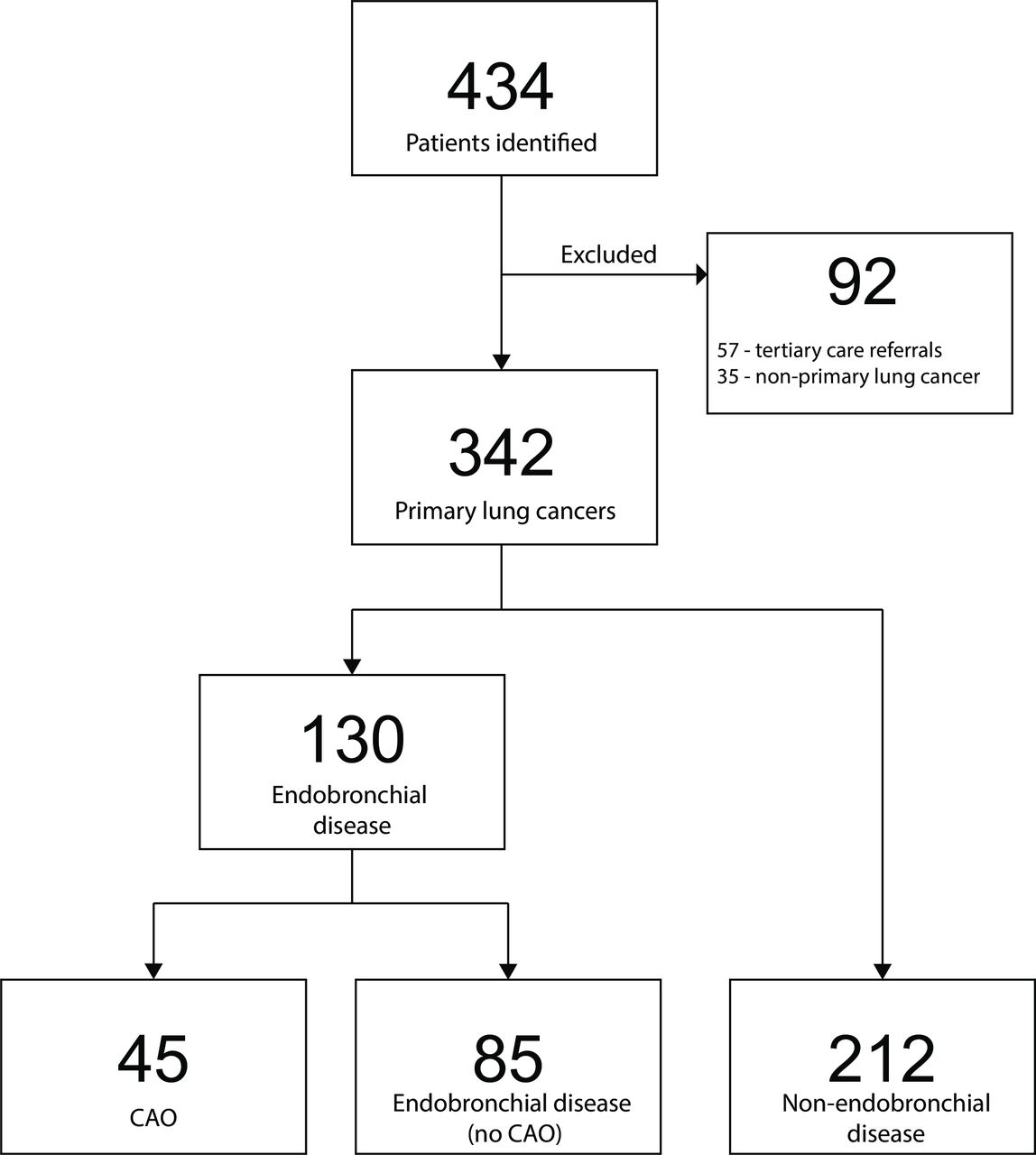
Patient cohort flow chart. CAO, central airway obstruction.
Endobronchial disease
A total of 130/342 (38%; 95% CI 33% to 43%) patients had radiological endobronchial disease (including central airways disease). Men and women were equally affected and 115/130 (88%) had stage III or IV disease. The most common cell type was NSCLC-ad (41/130 (32%)).
However, by histological type a higher proportion of endobronchial disease was seen in non-small cell lung cancer squamous cell (NSCLC-sq) (33/61 (54%)) and small cell lung cancer (SCLC) (17/31 (55%)) compared with adenocarcinoma 41/132 (31%)) (p<0.01). The most common site of lobar endobronchial disease was the upper lobes (49/85 (58%)).
Prevalence of CAO
The prevalence of CAO on index CT scans was 45/342 (13%; 95% CI 10% to 17%). Radiological reports identified 31/45 (69%) of cases, while the remainder were identified on focused review of the large airways of index CT scans (table 2).
Clinical features of n=45 patient with central airway obstruction at diagnosis
The most common site of disease was the bronchus intermedius (20/45 (44%)), with right-sided lesions accounting for 33/45 (73%) of cases. Severe CAO was seen in 34/45 (76%). The median degree of obstruction was 63 (IQR 50–100). Only 3/45 (7%) did not have distal viable lung.
Bronchoscopy was performed in 28/45 (62%) of patients; 20/28 (71%) had flexible bronchoscopy, 3/28 (11%) had rigid bronchoscopy and 5/28 (18%) had both. Histology was unavailable for 10/45 (22%) of patients. Of the 35 patients with available histology, NSCLC-sq was the most frequent 13/35 (37%); 11/35 (31%) had NSCLC-ad and 6/35 (17%) had SCLC (table 1). Intrinsic disease was observed in 28/45 (62%) of patients (table 2). Among 13/17 (76%) of patients with extrinsic compression and known histology, most were caused by NSCLC (9/13 (69%)). However, 4/6 (67%) of all SCLCs with CAO caused extrinsic compression.
Clinical features of patients with CAO
Among 44/45 (98%) of patients with CAO and available clinical information, 30/44 (68%) had a cough, 27/44 (61%) had breathlessness and 7/44 (16%) reported haemoptysis (table 2). No symptoms were reported by 8/44 (18%). The WHO performance status was obtained for 44/45 (98%) of patients. Of these 27/44 (61%) had a performance status of ≤2. In 23/45 (51%) of patients, the new diagnosis of lung cancer with CAO was made during or following a hospital admission, and 9/23 (39%) of these patients had a performance status ≤2.
Treatment
Treatment was offered to 32/45 (71%). Of these, six patients declined or were deemed unsuitable for treatment on referral. Therefore, a total of 26/45 (58%) patients received treatment (figure 2). In all, 10/31 (32%) eligible for therapeutic bronchoscopy were referred. Therapeutic bronchoscopy was performed in 8/31 (26%) of patients; of the two patients referred in whom the treatment did not occur, one was considered unlikely to benefit, and the other was too unwell on the day of the procedure. Procedures were performed by a combination of thoracic surgeons with or without an interventional pulmonologist. Of those undergoing de-bulking, four patients also received radiotherapy and one patient received chemotherapy and radiotherapy. An additional 20 patients were referred to oncology (figure 2); of whom two declined any further treatment.

Treatment modalities in patients with central airway obstruction.
Survival
The median follow-up time of all 342 patients was 303.5 (IQR 76–938) days. There were 273 deaths during 179 151 person days of follow-up giving an overall mortality rate of 1.52 (95% CI 1.35 to 1.71) per 1000 person days. Over the audit period overall survival was 44% at 1 year, 29% at 2 years, 23% at 3 years and 20% at 4 years, respectively. The overall median survival time was 193 (IQR 57–436) days.
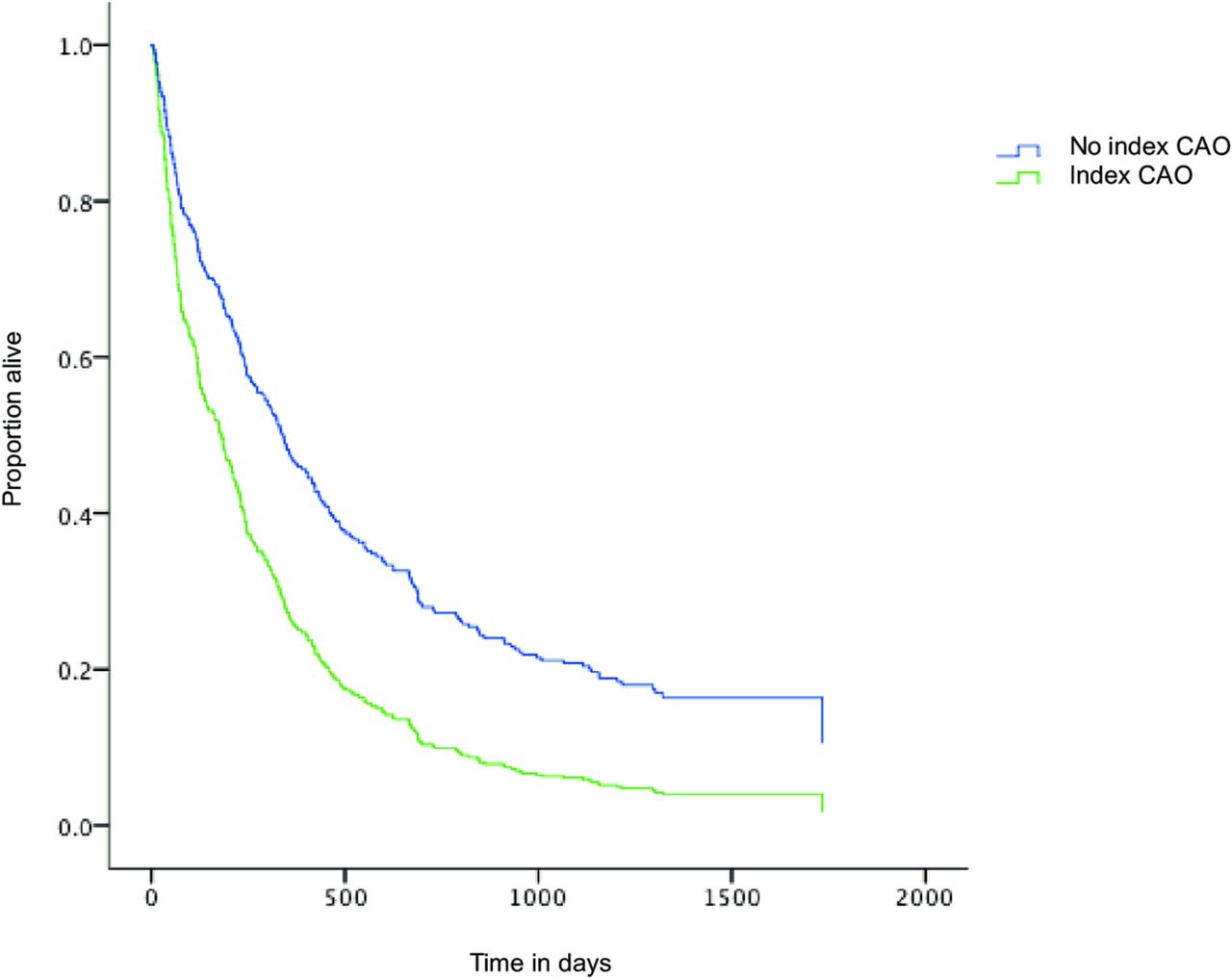
Mortality rates among patients with and without CAO on index CT scan were 4.67 (95% CI 3.48 to 6.28) per 1000 person days and 1.35 (95% CI 1.19 to 1.53) per 1000 person days, respectively (p<0.001; table 3). In patients with CAO on index CT scans, survival was 18% at 1 year, 4% at 2 years, 2% at 3 years and 2% at 4 years, respectively, with a median survival time of 94 (IQR 33–274) days (figure 3).
Univariate and multivariate analysis of factors associated with death among n=342 with primary lung cancer; using Cox proportional hazards regression
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curve for patients with and without central airway obstruction (CAO).
On univariate analysis CAO on index CT scan, age and high disease stage were associated with an increased hazard of death (table 3). On multivariate analysis, after adjusting for age, gender and disease stage, CAO on index CT scan remained independently associated with an increased hazard of death (aHR 1.78 (95% CI 1.27 to 2.48); p=0.001). Stage ≥IIIB disease was also associated with an increased hazard of death, on multivariate analysis (aHR 3.52 (95% CI 2.70 to 4.60); p<0.001).
Incidence risk of CAO
The median period of radiological follow-up for 297 patients without CAO on index CT scan was 225 (IQR 42–549) days. Over this period, a further 15/297 (5%) developed CAO in a median of 340 (IQR 114–551) days and 10/15 (75%) died within 30 days of the follow-up CT scan showing new CAO.
Patients with endobronchial disease on index CT scan developed incident CAO more frequently (7/85 (8%) with compared with 8/212 (4%) without index endobronchial disease; table 1), but this was not significant (p=0.14). The median time to disease recognition for the two groups also showed a difference, but again this did not reach statistical significance (median time to CAO 189 (IQR 93–275) days vs 619 (IQR 182–819) days for those with and without endobronchial disease, respectively (p=0.09)). Overall during the audit period, 60/342 (18%; 95% CI 14% to 22%) had or developed CAO.
Discussion
In our audit of new primary lung cancers between 1 November 2014 and 30 November 2015, the prevalence of CAO at the time of diagnosis was 13%, and of these, three quarters had severe CAO. During the follow-up period a further 5% developed CAO. As far as the authors are aware, this is the first description of CAO prevalence in the past 40 years and provides a benchmark for UK lung cancer services.
The prevalence of CAO in our audit was lower than the 20%–30% prevalence previously reported in the literature.2 The differences are likely due to different diagnostic methods and changes in lung cancer epidemiology over time, with NSCLC-ad being the most common histological type in recent years.8 Despite this, CAO remained a common finding among patients with primary lung cancer in our audit.
Descriptions by Brewer dating back more than 50 years, of patients undergoing exploratory thoracotomy, found that 24% had disease in the main bronchi, and a further 54% in the lobar bronchus.3 A case series of chest radiograph findings from the 1970s, found 20% had disease in the main bronchus and a further 49% had disease in the lobar bronchus.4 Postmortem studies in the 1970s found that 21% of patients had disease of their main bronchus,9 with NSCLC-sq accounting for 38% of cases and only 8% of cases being NSCLC-ad. Tracheal involvement at postmortem was found in 32/472 (7%) of SCLC cases, and in 1/35 (3%) of NSCLC-ad cases.10 11 Both study groups had undergone treatment prior to death. We found NSCLC-ad accounted for most endobronchial disease (32%) in our audit. However, patients with NSCLC-sq and SCLC were more likely to have endobronchial disease (including CAO), than patients with NSCLC-ad (~50% of NSCLC-sq and SCLC compared with 30% of NSCLC-ad). But, NSCLC-ad remained equally represented, due to the larger absolute numbers. Only 70% of patients in our audit had histological confirmation; but the histological subtype of cancers was similar to that seen in UK National Lung Cancer Audit data.1
A dedicated review of the central airways on CT scans increased the proportion with CAO detected by over 30%. This is consistent with previous reports and supports an argument that dedicated thoracic radiologists and interventional pulmonologists will improve disease recognition.12 Not all patients underwent bronchoscopy to confirm disease site; therefore, our CAO prevalence is likely to be an underestimate. Despite this, CT scans have a high sensitivity for CAO detection, while being the key investigation to drive subsequent investigations.13 14 We found the most common sites of CAO were the right main bronchus and bronchus intermedius. We found only one (2%) patient with CAO had tracheal disease. This is similar to previous postmortem studies but differs from therapeutic bronchoscopy case series where 20%–25% of patients were treated for tracheal disease.10 11 15–17 The latter is, however, likely to reflect patient selection for interventions.
The focus of any intervention is symptom relief.17 Most patients selected for therapeutic bronchoscopy will benefit, with over 50% experiencing a measurable change in their quality of life and potentially, performance status.17–19 This could also enable other treatment options. Endobronchial palliative treatments are more effective in those with poorer performance status.17 20 In our audit, >80% of patients with CAO had symptoms, 76% had severe obstruction and only 9% had a performance status of 0. In addition, ~50% of patients were diagnosed during an acute hospital admission which may represent an acute change in symptom burden or severity. Therefore, most patients in our audit are likely to have benefited from symptom control, with nearly 70% eligible for therapeutic bronchoscopy based on CT findings. Yet, only a third of those eligible were referred. With 38% of patients having had a poor performance status and possibly not considered for considered for further investigation or systemic treatments, combined with our finding that nearly a third of CAO cases were not identified on index CT scans highlights the need for timely CAO diagnosis and referral for care. Most patients with CAO in our audit had advanced disease; but, ~15% had ≤stage IIIA disease, indicating potentially curable disease. In patients in whom surgery is not an immediate option, aggressive endobronchial treatment should be considered to ensure early symptom relief while diagnosis and staging are completed.
We found CAO and high disease stage were independently associated with an increased mortality rate. The median survival of patients with CAO in our audit was 3 months; but 25% of patients lived >8 months. A recent study of patients with and without CAO, found no difference in the proportion that died or median survival time in the two groups.21 However, this study only included patients with advanced stage cancer (stage ≥IIIa), who had treatment, and ~80% of those without CAO had stage IV disease, with this proportion being lower (~60%) in those with CAO; this is likely to explain these results.21 Chhajed et al, found retrospectively that patients with NSCLC with CAO treated with therapeutic bronchoscopy and chemotherapy do as well as those without CAO treated with chemotherapy.22 The high mortality we found among patients with CAO on lung cancer diagnosis in our audit, again highlights the need for early disease recognition and prompt linkage to appropriate care and treatment services in this patient group.
Our audit was only conducted at a single site; however, the gender, age, stage, histological confirmation and histology distribution of our patients was similar to UK National Lung Cancer Audit data which suggests our results are generalisable.1 Further limitations included a single interventionalist review of CT scans to define CAO, with the absence a blinded second reader of all scans, to understand inter observer reliability. Further the absence of bronchoscopy combined with some missing data could result in the prevalence of disease being underestimated. However, this methodology for audit purposes, reflects the true-life approach often experienced in lung cancer services. Nonetheless, our findings, the first to report on CAO prevalence in over 40 years, support an urgent call for wider national audits to understand current practice in patients with CAO, benchmark best practice and identify methods to improve the outcomes of this vulnerable patient population. Further, tracking the epidemiology of CAO will be important to ensure adequate resources are in place, as molecular and immunological targeted therapies increase the number of patients living with advanced lung cancer.
Conclusions
We found a CAO prevalence of 13% at lung cancer diagnosis, with a further 5% of patients developing CAO during follow-up. Patients with prevalent CAO at lung cancer diagnosis had a higher mortality rate than those without CAO. Our data provide a benchmark for service planning, highlights the poor outcome associated with this disease phenotype and the need to urgently address this with well conducted interventional treatment studies.
Acknowledgments
We acknowledge the assistance from our cancer services team for their assistance with data. MA acknowledges the receipt of support from the European Respiratory Society ERS fellowship ID STRTF 2016-7508. LAT is supported by an MRC UK Clinical Research Training Fellowship. This work has been supported by the Plymouth and Cornwall Cancer Fund.
References
Footnotes
Presented at Preliminary work in this audit was presented as a poster at the British Thoracic Society Winter Meeting in 2016.
Contributors CD devised the audit and drafted the manuscript. All authors contributed to the methodology, data collection, interpretation, analysis and revision of manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.