Article Text

Abstract
Introduction Sarcoidosis is a multisystem granulomatous inflammatory disorder. Sarcoidosis is associated with significant morbidity and rising healthcare utilisation. Patients with sarcoidosis report higher psychological symptoms than the general population. We evaluated the association between depressive and anxiety symptoms and clinical outcomes in patients with pulmonary sarcoidosis requiring treatment.
Methods Adult patients in the Johns Hopkins Sarcoidosis Clinic diagnosed with pulmonary sarcoidosis on treatment were eligible for enrollment. Questionnaires were administered to assess depressive and anxiety symptoms, healthcare utilisation and health-related quality of life (HRQoL).
Results 112 participants were enrolled (57% women, 53% African American, median age: 57 years). 34% of participants screened positive for mild and 20% for moderate–severe depressive symptoms. 25% of participants screened positive for mild and 12% for moderate–severe anxiety symptoms. Participants with moderate–severe psychological symptoms had a higher odds of an emergency department visit in the previous 6 months (8.87 for depressive symptoms and 13.05 for anxiety symptoms) and worse HRQoL compared with participants without psychological symptoms. Participants with moderate–severe depressive symptoms had lower diffusion capacity of the lungs for carbon monoxide % predicted compared with those without depressive symptoms. There was no association between elevated psychological symptoms and the odds of hospitalisation, forced vital capacity % predicted and forced expiratory volume in 1 second % predicted.
Conclusion Psychological symptoms may be associated with worse clinical outcomes in sarcoidosis. Improving the recognition through clinic screening and referral for treatment of depression and anxiety in sarcoidosis may reduce acute healthcare utilisation and improve HRQoL.
- sarcoidosis
- psychology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Is there an association between psychological symptoms and worse clinical outcomes among individuals with sarcoidosis requiring treatment?
Improving the recognition through clinic screening and referral for treatment of depression and anxiety in sarcoidosis may reduce acute healthcare utilisation and improve HRQoL.
Sarcoidosis is one of the most common interstitial lung diseases in the USA and is associated with significant morbidity and rising healthcare utilisation.
Introduction
Sarcoidosis, a disorder of non-caseating granulomatous inflammation, is one of the most common interstitial lung diseases in the USA.1 2 Up to half of patients with sarcoidosis develop chronic disease and may require long-term or life-long treatment to prevent disease progression.3 Guidelines suggest treatment be given to individuals who have pulmonary sarcoidosis with progressive organ dysfunction and/or symptoms.4 Those with sarcoidosis requiring treatment have significantly higher morbidity including lower lung function, worse quality of life and depression compared with individuals not requiring treatment.5 6
The prevalence of depression in sarcoidosis ranges from 18% to 66%6–10 and anxiety ranges between 31% and 33%,9 11which is higher than in the general population.9 10 Other chronic diseases such as psychological disorders have been associated with a higher rate of healthcare utilisation.12 13 Healthcare utilisation among individuals with sarcoidosis almost doubled between 1998 and 2008.14 We are aware of no studies in sarcoidosis to date that have investigated the association between psychological symptoms and healthcare utilisation.
In other chronic pulmonary illnesses, psychological symptoms are associated with lower health-related quality of life (HRQoL) independent of disease severity.15–17 Depressive symptoms have been correlated with lower HRQoL in patients with sarcoidosis; however, these studies have not evaluated the association while controlling for other factors such as disease severity.10 18 19 The previous studies have included those with sarcoidosis requiring medication and those with asymptomatic sarcoidosis or sarcoidosis not requiring medication.10 18 19 Patients with sarcoidosis requiring treatment have higher rates of depressive symptoms and worse quality of life compared with asymptomatic patients6 suggesting those requiring treatment should be evaluated separately.
The purpose of this study is to evaluate the association of psychological symptoms and clinical outcomes among people with sarcoidosis requiring treatment. We hypothesised that psychological symptoms would be associated with an increased odds of healthcare utilisation, worse HRQoL and worse pulmonary function.
Materials and methods
Procedures
The study was reviewed and all recruitment procedures and study protocols were approved by the Johns Hopkins University Institutional Review Board (IRB-X 00182289). This was a cross-sectional study conducted from August 2018 to February 2019. Adults ≥18 years from the Johns Hopkins Sarcoidosis Clinic were eligible for enrollment if they had a diagnosis of pulmonary sarcoidosis and were on treatment for sarcoidosis. Treatment included corticosteroids and steroid-sparing agents. Oral informed consent was obtained from all study participants. Following enrollment, the research team administered several questionnaires assessing HRQoL, healthcare utilisation, depressive symptoms, anxiety symptoms and sociodemographic information. The medical charts were also abstracted to assess organ involvement, comorbidities, date of diagnosis and pulmonary function test results.
Measures
Depressive symptoms were assessed using the Patient Health Questionnaire depression scale (PHQ-8). The PHQ-8 is a validated measure to screen for depression.20 A score of ≥10 indicates moderate–severe depressive symptoms and is associated with clinically significant symptoms of depression where a score of ≥5 and <10 indicates mild depressive symptoms.20 Participants with scores of ≥10 were provided a mental health referral guide which included information for local mental health resources.
Anxiety symptoms were assessed using the Generalised Anxiety Disorder 7-item (GAD-7). The GAD-7 is a validated measure to screen for anxiety21 and has been used in other pulmonary diseases.22 A score of ≥10 indicates moderate anxiety and a score of ≥5 and <10 indicates mild anxiety.
Healthcare utilisation was obtained through a self-report questionnaire in which participants reported whether they were hospitalised in the 12 months prior to enrollment. Additionally, participants reported whether they had an emergency department (ED) visit in the 6 months prior to enrollment.
Results from lung function testing conducted nearest to the date of the survey completion and less than 1 year from survey completion were abstracted from the participants’ medical record. Forced expiratory volume in 1 s (FEV1), FEV1 % predicted, forced vital capacity (FVC), FVC % predicted, FEV1/FVC, diffusion capacity of the lungs for carbon monoxide (DLCO), DLCO % predicted were all abstracted, if available. Complete lung function tests within the last year were available for 58% participants.
HRQoL was assessed using both the St. George Respiratory Questionnaire (SGRQ) and King’s Sarcoidosis Health Questionnaire (KSQ). The SGRQ is an instrument containing 50 items that assesses symptoms, activity and disease impact.23–25 The SGRQ has been used in multiple pulmonary sarcoidosis clinical trials.26 27 A lower SGRQ score indicates a higher HRQoL. The KSQ is a 29-item validated measure of sarcoidosis health status.28 29 We used the 16-item lung and general health status subscale. The KSQ has been found to have moderate correlation to lung function in sarcoidosis.28 A higher score on the KSQ indicates a higher HRQoL.
Sociodemographic information was collected by questionnaire. When evaluating race/ethnicity, three participants identified as Asian, one participant identified as Panamanian, one participant identified as Puerto Rican, one participant identified as other, and one participant identified as American Indian. We limited our analysis to participants of White and African American races because of the small numbers in the other race/ethnicity categories.
Sarcoidosis organ involvement, comorbidities, medication regimen and disease duration were also collected. The sarcoidosis organ assessment tool that was recently used in the National Heart, Lung, and Blood Institute (NHLBI) supported Genomic Research in Alpha-1 Antitrypsin Deficiency and Sarcoidosis study30 was used to assess organ involvement. Organ involvement was categorised into three groups as 1, 2–4 and ≥5 organs with probable, highly probable or definite involvement included. The Charlson Comorbidity Index (CCI)31 was used to assess comorbidities. The medication regimen was abstracted from the chart and confirmed with participants at time of enrollment. Medication regimens were categorised into corticosteroid only, corticosteroid plus steroid-sparing agent (such as methotrexate or azathioprine) or steroid-sparing only. Disease duration was calculated by subtracting the date of diagnosis from the date of enrollment.
Statistical analysis
Descriptive statistics were conducted to evaluate distribution of all data, with median (IQRs) for continuous variables and frequency (percent) for categorical variables. Patients were categorised into no depressive or anxiety symptom category if PHQ-8 or GAD-7 was <5, mild depressive or anxiety symptoms if PHQ-8 or GAD-7 was between 5 and 9, and moderate–severe depressive or anxiety symptoms if PHQ-8 or GAD-7 was ≥10. We performed multiple linear regression models to assess the association between psychological symptoms (depressive and anxiety symptoms) and all continuous clinical outcomes such as HRQoL (SGRQ and KSQ), lung function (FVC % predicted, FEV1 % predicted and DLCO % predicted). Models included these a priori identified covariates: race, age, gender, education, income, organ involvement, CCI, medication regimen, disease duration, and anti-depressant use or anxiolytic use, respectively. We performed multiple logistic regressions to assess the association between healthcare utilisation (ED visits and hospitalisation both coded as presence or absence) and depressive or anxiety symptoms. All analyses were performed using Stata V.15 (College Station, TX, USA).
Patient and public involvement
There were no funds or time allocated for patient and public involvement so we were unable to involve patients. We have invited patients to help us develop our dissemination strategy.
Results
In all, 257 individuals met the inclusion criteria. Of the 257 eligible, 180 individuals were approached and of those 128 individuals were enrolled. The most common reason for not being approached was that the individual missed his or her clinic appointment (n=41). The most common reasons for not joining the study were individuals being too busy or not interested. Nine participants were excluded due to incomplete data and seven were excluded due to limited numbers as described above. A total of 112 participants were included in the analysis, which represents 44% of all eligible participants (online supplementary appendix).
Supplemental material
Demographic characteristics are presented in table 1. The study population consisted of 57% women and 53% African American with a median age of 57 years. Corticosteroids and steroid-sparing agents were prescribed to 47% of participants compared with 34% prescribed steroids only, and 19% steroid-sparing agents only. Most participants had multiple organ involvement (70% of participants had extra-pulmonary sarcoidosis). Within the cohort, 34% of the cohort screened positive for mild depressive symptoms and 20% of participants screened positive for moderate–severe depressive symptoms. Anti-depressants were prescribed to 30% of participants (table 1). Within the cohort, 25% of the cohort screened positive for mild anxiety symptoms and 13% of participants screened positive for moderate–severe anxiety symptoms (table 2). Anxiolytics were prescribed to 11% of participants (table 1). Only 29% and 14% of participants who screened positive mild depressive or anxiety symptoms, respectively, were prescribed pharmacotherapy. 55% and 23% who screened positive for moderate–severe depressive or anxiety symptoms, respectively, were prescribed pharmacotherapy.
Participant characteristics
Clinical outcomes by psychological symptoms
Association of psychological symptoms and healthcare utilisation
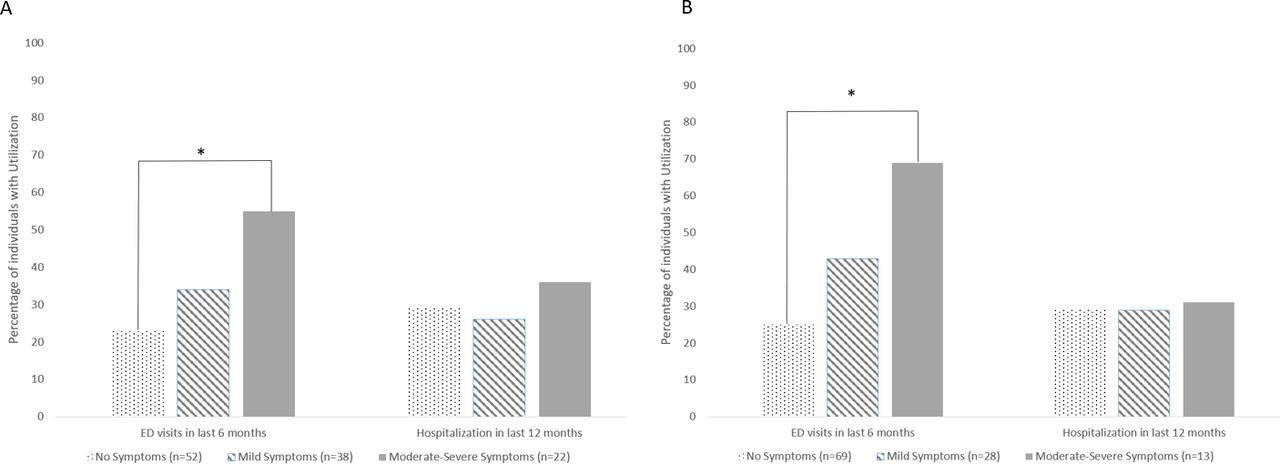
Among the cohort, 35% of participants reported an ED visit in the previous 6 months and 29% of participants reported hospitalisation in the previous 12 months. Of note, 51% of the participants who reported an ED visit in the previous 6 months did not report a hospitalisation in the prior 12 months. Additionally, 42% of participants who reported a hospitalisation in the last 12 months did not report an ED visit in the last 6 months. Participants who screened positive for moderate–severe depressive symptoms had an 8.87 higher odds of an ED visit in the last 6 months and those that screened positive for moderate–severe anxiety symptoms had a 13.05 higher odds of an ED visit in the last 6 months compared with those participants without depressive or anxiety symptoms, respectively (p<0.05) after controlling for covariates. This trend was not seen in those with mild depressive or anxiety symptoms. Neither depressive nor anxiety symptoms were associated with increased likelihood of a hospitalisation in the last 12 months (table 3, figure 1).

Healthcare utilisation by (A) depressive symptoms (B) anxiety symptoms. *p<0.05.
Association between clinical outcomes and psychological symptoms
Association of psychological symptoms and lung function
In multiple linear regressions, participants who screened positive for moderate–severe depressive symptoms had lower DLCO % predicted compared with those without depressive symptoms (p<0.05) after controlling for covariates. This trend was not seen in those with mild depressive symptoms. Additionally, there was no significant association between FVC % predicted and FEV1 % predicted based on depressive symptoms. There was no significant association between anxiety symptoms and DLCO % predicted, FVC % predicted or FEV1 % predicted.
Association of psychological symptoms and HRQoL
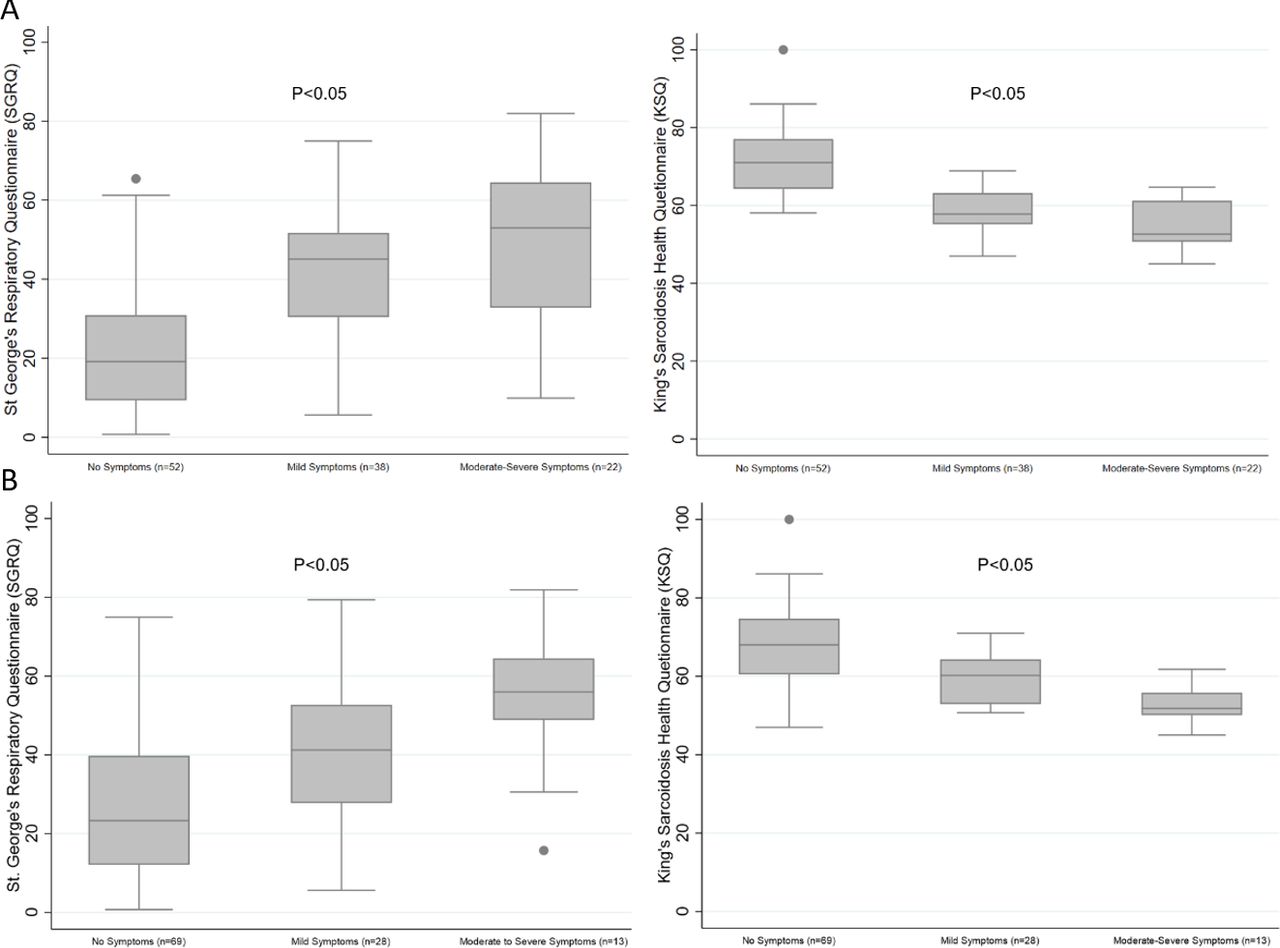
In multiple linear regressions, participants who screened positive for mild psychological symptoms and moderate–severe psychological symptoms had worse HRQoL as measured by both the SGRQ and KSQ compared with those who did not screen positive for psychological symptoms after controlling for covariates (table 3, figure 2). Additionally, we found no association between HRQoL and the prescribed treatment regimen for sarcoidosis.

{kind=link}
{kind=link}
Differences in HRQoL measures by (A) depressive symptoms (B) anxiety symptoms. Lower scores on the St. George’s Respiratory Questionnaire indicates better HRQoL. Higher scores on the King’s Sarcoidosis Health Questionnaire indicates better HRQoL. HRQoL, health-related quality of life.
Discussion
Within our cohort of participants with sarcoidosis on treatment, 54% reported some depressive symptoms and 37% reported some anxiety symptom with 20% and 13% screening positive for moderate–severe depressive or anxiety symptoms, respectively. Screening positive for moderate–severe psychological symptoms was associated with higher odds of ED visits and worse HRQoL compared with those without psychological symptoms. Screened positive for moderate–severe depressive symptoms was associated with lower DLCO % predicted; however, this association was not seen with anxiety symptoms. Screening positive for mild psychological symptoms was associated with worse HRQoL, but was not associated with the other outcomes.
The prevalence of psychological symptoms in our cohort is consistent with previous studies6–10 and similar to findings in other chronic lung diseases,32but more than double that of the general population.33 Depression and anxiety may be underdiagnosed and undertreated in this population as only 29% and 14% of participants who screened positive mild depressive or anxiety symptoms, respectively, were prescribed pharmacotherapy. Additionally, 55% and 23% who screened positive for moderate–severe depressive or anxiety symptoms, respectively, were prescribed pharmacotherapy. We did not assess how many participants were receiving psychotherapy, which may be important to consider since combination treatment with pharmacotherapy and psychotherapy is more effective than pharmacotherapy alone.34 35 In other chronic diseases, treating psychological disease such as depression and anxiety has been shown to reduced morbidity36 and should be investigated further in sarcoidosis.
Psychological diseases such as depression are risk factors for increased healthcare utilisation in other chronic diseases.12 13 Our findings of increased odds of ED visits among participants with moderate–severe psychological symptoms suggest that participants are seeking care for reasons other than a sarcoidosis-related illness, such as a barrier to outpatient care, which is seen in other diseases.37 Alternatively, depression is commonly associated with somatisation which has been linked to increased healthcare utilisation.38 Additionally, depression has been associated with higher levels of pro-inflammatory cytokines, including tumour necrosis factor and interleukin-6,39 both of which contribute to the immunopathology of sarcoidosis. Interleukin-6 has been shown to be highly expressed in sarcoidosis-affected tissues40 and is described as a potential treatment target in sarcoidosis.41 Enhanced expression of interferon-gamma (IFNγ) remains the principal immunological characteristic of sarcoidosis.42 Since treatment of depression may decrease IFNγ production,43 44 this suggests that there are potentially complex interactions between untreated sarcoidosis and depression. Lastly, treatment of sarcoidosis with corticosteroids may contribute to the development of depression due to the associated side effects despite its anti-inflammatory effects.45 There may be an association with depression and the inflammation seen in sarcoidosis, which may result in more frequent symptoms and healthcare utilisation. Future studies, which include the indication for healthcare utilisation are needed to further investigate this possible association.
Our findings of psychological symptoms being associated with worse HRQoL confirms previous studies that have found a correlation between HRQoL and depressive symptoms in sarcoidosis18 19 and an association between symptom severity and anxiety.11 However, our study included covariates such as organ involvement and comorbidities which have not been included in previous studies. We did not include measure of fatigue, which is common in sarcoidosis,46 as a covariate in our analyses. Further investigation should be done to determine whether fatigue accounts for some of the association between HRQoL and depressive symptoms. Previous studies have reported an association between corticosteroid treatment and worse HRQoL; however, those studies have compared those on treatment with corticosteroids to those not requiring treatment which may be confounding the previous findings.10 An observational study found worse HRQoL among participants with high cumulative prednisone dose compared with a lower prednisone dose group,47 but this study did not compare corticosteroid treatment to other medication regimens used in sarcoidosis. Our sample was limited to patients who were on treatment for sarcoidosis and we did not find an association between the prescribed medication regimen and HRQoL. Further investigation including evaluating the cumulative medication dose should be done to investigate the relationship between medication regimen and HRQoL.
Our results found an association between reduced lung function, specifically DLCO % predicted, and depressive symptoms. Our findings are consistent with findings in other chronic lung diseases, which have linked the association to non-adherence.48 We did not have an objective measure of adherence in our study. Future studies that include objective measures of adherence are needed to further explore whether the association between reduced lung function and depressive symptoms in sarcoidosis is due to non-adherence. The DLCO % predicted and not the other lung function parameters being associated with depressive symptoms may be related to a different inflammatory profile among individuals with isolated reduced diffusion capacity. However, future studies are needed to test this hypothesis. Additionally, the association between lower DLCO % predicted and depressive symptoms may be that individuals with lower lung function are more depressed. Previous studies in sarcoidosis have not included DLCO when assessing lung function outcomes, which should be reconsidered in the future.10 47 49
There are several limitations to our study including that it was a cross-sectional study and therefore is unable to study the directionality of associations. Future longitudinal studies are necessary to further investigate the association between depressive symptoms, adherence and clinical outcomes in sarcoidosis. Additionally, a limitation is that we used a self-report measure of healthcare utilisation; however, studies have shown self-report measures of utilisation are a valid proxy.50 Our lung function data were abstracted from medical charts and had a high amount of missing data. Lastly, we used a screener for depressive symptoms and anxiety symptoms instead of the diagnosis of clinical depression and anxiety, which may misclassify some participants. Future research should consider the use of a gold standard for depression such as a psychiatric interview.
Conclusion
Our study confirms previous findings of high rates of psychological symptoms among sarcoidosis patients. The US preventative task force recommends screening for psychological diseases such as depression.51 Given the burden of psychological symptoms in sarcoidosis and its associations with clinical outcomes, screening and treating for depression and anxiety may be especially important. Future studies are needed to understand the impact depression and anxiety may have on clinical outcomes in sarcoidosis.
References
Footnotes
Contributors MNE had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis, including and especially any adverse effects. MWS, MNE, TB, ESC, CSR and DRM substantially to the study design, data analysis and interpretation, and the writing of the manuscript. This research was supported by the American Thoracic Society Fellowship in Health Equality and the Pearl M Stetler Fellowship Award. Research reported in this publication was supported by the National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Number T32HL007534. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding This work was supported by the American Thoracic Society Fellowship in Health Equality, the National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Number T32HL007534, and the Pearl M Stetler Fellowship Award.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.