Article Text

Abstract
Background Vitamin B12 and folic acid (referred to as vitamin supplementation) improves the toxicity profile of pemetrexed containing regimens. Low baseline vitamin B12 and folate levels are reflected in a raised total homocysteine level (HC). Studies have suggested that pretreatment HC levels predict neutropenia toxicity. We have tested supplementation with vitamin B12 and folate in non-pemetrexed platinum-based regimens to decrease treatment-related toxicity and looked for a correlation between toxicity and change in homocysteine levels.
Patient and method Eighty-three patients with advanced lung cancer and malignant mesothelioma were randomly assigned to receive platinum-based chemotherapy with (arm A) or without (arm B) vitamin B12 and folic acid supplementation. The primary end point was grade 3/4 neutropenia and death within 30 days of treatment. Secondary end points included quality of life, overall survival (OS) and the relationship between baseline and post supplementation HC levels and toxicity.
Results In the intention-to-treat population, no significant difference was seen between the two groups with respect to chemotherapy-induced grade 3/4 neutropenia and death within 30 days of chemotherapy (36% vs 37%; p=0.966, emesis (2% vs 6%; p=0.9) or OS (12.3 months vs 7 months; p=0.41). There was no significant difference in survival rates by baseline HC level (p=0.9). Decrease in HC with vitamin supplementation was less frequent than expected. High baseline HC levels decreased with vitamin supplementation in only 9/36 (25%) patients (successful supplementation). Post hoc analysis showed that patients in arm A who were successfully supplemented (9/36=25%) had less neutropenic toxicity (0% vs 69%; p=0.02) compared to unsupplemented patients.
Conclusions The addition of vitamin B12 and folic acid to platinum-containing regimens did not overall improve the toxicity, quality of life or OS. Rates of grade 3/4 neutropenia at 36/37% was as predicted. Further studies to increase the rate of successful supplementation and to further test the biomarker potential of post supplementation HC levels in predicting chemotherapy-induced neutropenia in platinum-based chemotherapy are warranted.
Trial registration number: EudracCT 2005-002736-10 ISRCTN8734355.
- Lung Cancer
- Lung Cancer Chemotherapy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
-
In this un-blinded, randomised, phase II study 83 patients with advanced lung cancer and malignant mesothelioma were assigned to receive platinum-based chemotherapy with or without vitamin B12 and folic acid supplementation.
-
No significant difference was seen between the two groups with respect to chemotherapy-induced grade 3/4 neutropenia and death within 30 days of chemotherapy (36% vs 37%; p=0.966) emesis (2% vs 6%; p=0.9) or overall survival (12.3 months vs 7.0 months; p=0.41).
-
High baseline homocysteine levels decreased with vitamin supplementation in only 9/36 (25%) patients. Post hoc analysis showed that patients in arm A who were successfully supplemented had less neutropenic toxicity compared to unsupplemented patients (0% vs 69%; p=0.02).
Background
Folate and vitamin B12 supplementation with chemotherapy
Up to half of lung patients with cancer with advanced disease can be malnourished, on the basis of body mass index.1 There a number of potential reasons for this including poor diet, cancer-induced nausea, paraneoplastic processes and as a result of chronic smoking. Palliative chemotherapy is associated with grade 3/4 rates of neutropenia between 20% and 40%. There appears to be little difference in rates between the different carboplatin and cisplatin regimens commonly used in non-small cell lung cancer (NSCLC).2 ,3 The incidence of toxicity is similar when the same regimens are used in malignant mesothelioma (MM).4 The incidence is higher in regimens used in small cell lung cancer (SCLC) and in second-line NSCLC.5 ,6
Some preclinical trials have highlighted the impact of folate supplements on chemotherapy-induced toxicity and clinical response. Branda et al7 found that survival was significantly better in folate-supplemented rats receiving cyclophosphamide and 5-FU and this group developed less host toxicity compared to their folate deficient counterparts. The authors of the study hypothesised that the mechanism behind the interaction between folate metabolism and chemotherapy may be secondary to the relationship between folate status and glutathione level, which has been shown to correlate with chemotherapy toxicity.8 ,9
Pemetrexed containing regimes have been established as the standard of care for the treatment of MM and non-small cell lung cancer (NSCLC). The use of vitamin B12 and folic acid has been shown to decrease toxicity.4 This is logical given the inhibitory actions of pemetrexed in the folate pathway. In Vogelzang et al's trial of pemetrexed and ciplatin versus cisplatin alone in mesothelioma the incidence of grade 3 and 4 neutropenia in the cisplatin/pemetrexed arm was reduced from 41.4% to 23.2% (p=0.011) with vitamin supplementation. Febrile neutropenia was reduced from 5.2% to 0.6% (p=0.53).4 Interestingly however vitamin supplementation also appeared to benefit patients receiving cisplatin alone. There has been little further investigation of the role of folate and vitamin B12 supplementation in non-pemetrexed containing regimes despite this clinical and preclinical data.
Homocysteine levels as a marker of folate and vitamin B12 supplementation
Niyikiza et al carried out an analysis of pemetrexed-treated patients to identify predictive factors for severe toxicity. The results showed that pretreatment total plasma homocysteine (HC) levels significantly predicted severe thrombocytopenia and neutropenia and subsequent supplementation with vitamin B12 and folate reduced the incidence and severity of such toxicities without affecting efficacy. The normal range in this study was 7.5–11.5 μM/L in line with reports from cardiovascular study populations.10 High baseline homocysteine levels are associated with folate and vitamin B12 deficiency.11 Patients with high baseline HC level were found in other studies to have a high risk of severe haematological toxicity and vitamin-supplemented patients tended to improve or lower their concentrations of HC.10–12 Since total plasma HC level is affected by a series of genetic, physiological, lifestyle and clinical factors, Refsum et al13 have proposed that, in routine clinical setting, significant change in total plasma HC should be defined as a change of greater than 25% to 30% between samples collected on two occasions.
In this single centre, unblinded phase II randomised study, the aim was to assess the impact of vitamin B12 and folic acid supplementation on non-pemetrexed-based chemotherapy-related neutropenic events and to determine the potential role of using total plasma HC level before and after vitamin B12 and folic acid supplementation (using 30% reduction of HC level as a cut-off for successful supplementation) as a predictive biomarker of toxicity.
Patients and methods
Patients with NSCLC, SCLC or mesothelioma, who were suitable for platinum-based chemotherapy, were eligible for inclusion into the study if they fulfilled the following criteria: age>18 years, histologically or cytologically confirmed NSCLC, SCLC or mesothelioma; an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0–2; adequate organ function defined as an absolute neutrophil count >1.5×109/L, white cell count >3×109/L, platelet count >100×109/L, serum creatinine ≤1.25 upper level of normal, creatinine clearance >50 mL/min (EDTA) or >60 mL/min (Cockroft and Gault formula) for cisplatin or >40 mL/min for carboplatin; estimated life expectancy of at least 12 weeks. Patients were excluded if they had an active infection, inability or unwillingness to take vitamin supplementation, had taken any vitamins within the past 28 days or receiving concomitant radical chemotherapy and radiotherapy or antiepileptic treatment. All patients provided a signed informed consent before screening for the trial.
Patients were randomly assigned in a 1:1 ratio to arm A (with vitamin supplementation) or arm B (chemotherapy alone, no vitamin supplementation), which represented treatment with or without vitamin supplementation, respectively. Randomisation was carried out by telephone through the Institute of Cancer Research Clinical Trial and Statistics unit. Computer-generated permuted blocks were used and stratification was by centre. Block sizes were 4 and 6 (random). Vitamins were given on day of randomisation and chemotherapy was scheduled to begin at least 7 days later.
All eligible patients with NSCLC, SCLC and MM received platinum-based treatment with cisplatin dosed at 75 mg/m2 or carboplatin area under the curve (AUC5). One of the following regimens was adopted for this study at the discretion of the investigator: mitomycin-C plus vinblastine, vinorelbine, docetaxel, gemcitabine or etoposide with cisplatin or carboplatin. A total of up to six cycles of chemotherapy were administered and patients were allowed to receive full supportive care therapies concomitantly, except for growth factors as a prophylactic measure, during the study. Palliative radiation therapy was permitted for irradiating small areas of painful metastases that could not be managed adequately using systemic or local analgesia. Study treatment was discontinued if other forms of specific anti-tumour therapy were needed.
Patients randomised to arm A received oral folic acid 400 μg daily for at least 1 week prior to the first cycle of treatment and continued until 3 weeks after the last dose of chemotherapy. Vitamin B12 1 mg was administered as an intramuscular injection before treatment and every 9 weeks until 3 weeks after last dose. Compliance with vitamins was assessed at each treatment cycle by direct questioning by the research nurses. Patients randomised to arm B received no vitamin supplementation and patients were assessed three weekly to ensure additional ‘over the counter’ vitamin supplementation was not taken.
Blood samples for HC levels were taken after consent during screening (before randomisation) on two occasions and after at least 1 week of vitamins that is, on the day of initiation of systemic therapy. Success of supplementation was determined by comparing the two values and was defined as at least a 30% decrease in the HC level. CT scans were obtained at screening and every 6 weeks during the study, 21 days after the last dose of chemotherapy and at follow-up every 3 months.
All participants completed EORTC QLQ-C30 (V.3) and Lung module QLQ-LC13 prior to start of chemotherapy, at 6 weeks and every 3 months post treatment as appropriate until relapse or until 1 year post randomisation.
Safety was monitored by physical examination, haematology and biochemistry tests; assessment of ECOG PS and adverse event reporting, based on the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), V.3.0, before each cycle of chemotherapy. Full blood count including measurement of absolute neutrophil count was assessed at Day 1 and Day 8–10 of every chemotherapy cycles. All serious adverse events and suspected unexpected serious adverse reactions (SUSARs) were reported to the chief investigator within 24 h, as well as to the Royal Marsden Research and Development office in accordance with the Royal Marsden Hospital Standard Operating Procedures. In addition all SUSARs were reported to the main Regional Ethics Committee and the Medicine and Health Related Agency within the required timeframes.
Statistical analysis
The primary end point of the trial was to detect a reduction in neutropenia with the addition of vitamins to chemotherapy. The end points were analysed in an intention-to-treat population. In order to detect a clinically meaningful reduction in neutropenia from a predicted incidence of 40% to an incidence of 10%, with 90% power, a total of 84 patients were required that is, 42 per treatment arm.
The maximum grade of neutropenia experienced from the start of treatment until 30 days after the final course of treatment was calculated and tabulated by randomised treatment and compared by means of χ2 (5% level of significance was used). The proportion of patients on each treatment arm experiencing grade 3–4 neutropenia was reported as a percentage with 95% CIs. Non-neutropenic toxicity was tabulated by type of toxicity and by the worst grade experienced by each patient and summarised by the proportion of patients experiencing a grade 3–4 toxicity. Analysis was as for the primary end point (χ2) but a 1% level of significance was used because of the large number of treatment comparisons.
Death within 30 days of last chemotherapy was assessed by the principal investigator with the information available. Overall survival (OS) for treatment groups was measured from randomisation until death from any cause. Patients that were alive or lost to follow-up were censored at last follow-up date. OS was illustrated by means of Kaplan-Meier curves and the log rank statistic was used to compare survival between treatment groups.
Differences in HC levels at baseline between treatment groups A and B, and change from baseline HC levels between treatment groups A and B were assessed by the Mann-Whitney test.
QOL questionnaires were scored according to the EORTC QLC30 scoring manual. Changes from baseline (pretreatment) in the functional scales (physical, role, emotional, cognitive, social) and in global health scale were calculated at each timepoint (6 weeks and 3 monthly after the end of treatment). Difference between treatment groups for mean change from baseline was assessed by the Mann-Whitney test at each time point.
In a post hoc analysis the patients with a high baseline HC levels and a ≥30% reduction with vitamin supplementation were considered to be ‘successfully supplemented’. HC level and toxicity differences were compared between groups and tested using Fishers exact test.
The study was undertaken with institutional review and ethics approval and in accordance with the Principles of Good Clinical Practice (GCP), the European Union and GCP Directives (2001/20/EC; 2005/28/EC) and the Medicines for Human Use (Clinical Trials) and Blood Safety and Quality (Amendment) Regulations 2008 (Statutory Instrument 2008 No. 941). The study was approved by the The Royal Marsden Local Research Ethics Committee and was run on only one site. REC reference number 05/Q0801/178
Results
Between September 2006 and February 2011 there were 84 patients recruited into the study; 41 to chemotherapy with vitamin supplementation (arm A) and 43 to chemotherapy alone (arm B). One patient had myeloma and was therefore excluded. As a result, a total of 83 patients were considered for the final analysis (figure 1—consort diagram). In table 1, patient characteristics are shown and were balanced for disease subtype, chemotherapy used and first-line and second-line therapies. There were 77 patients analysed for toxicity (the primary end point) and 78 for QOL, OS and HC (figure 1).
Patient characteristics
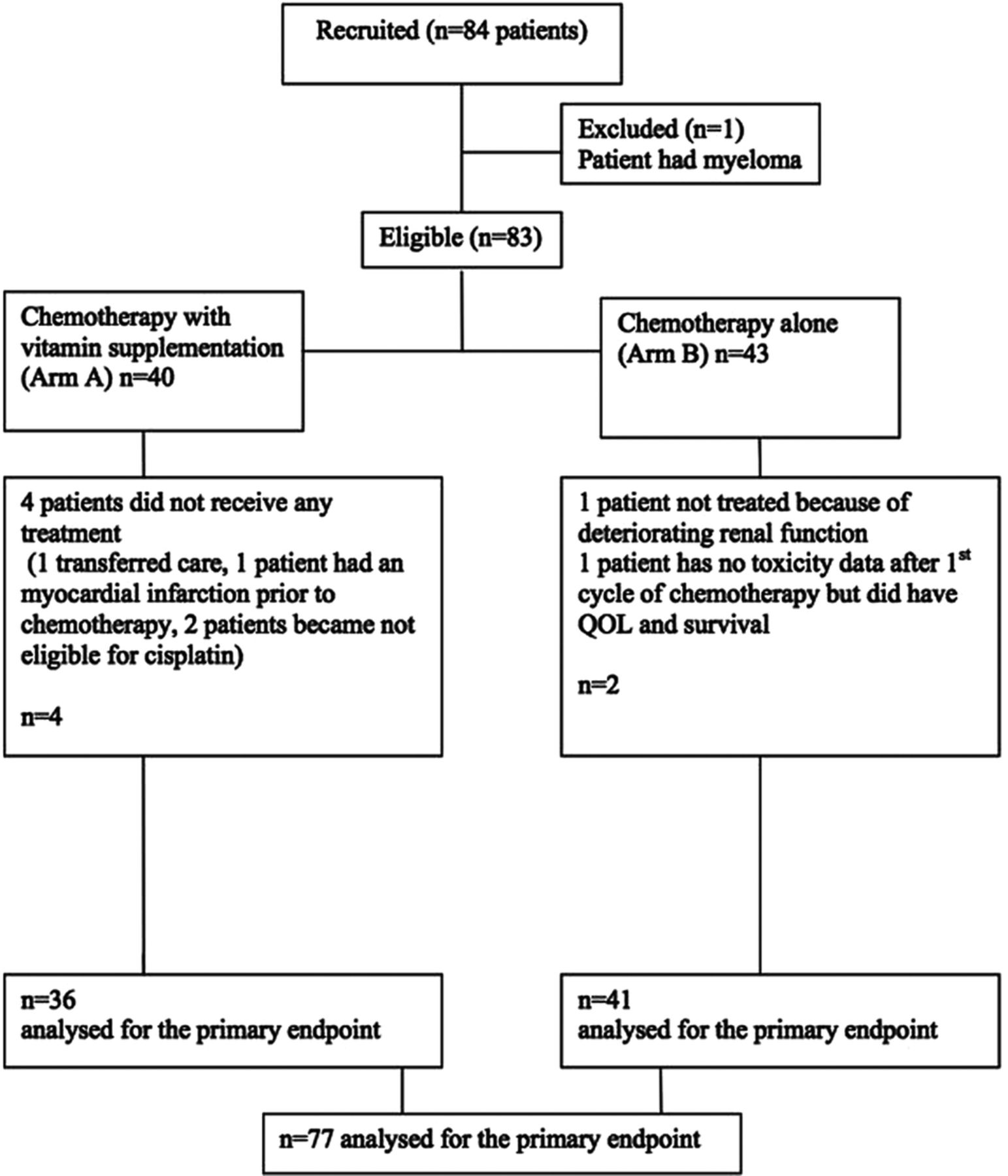
Consort diagram.
Primary end point
The primary end point was the difference in grade 3/4 neutropenia and death within 30 days of treatment between the treatment arms. χ2 Test for trend showed no significant difference between the arms (p=0.631). The proportion of patients experiencing grade 3/4 neutropenia or death within 30 days of treatment was 36% in arm A (95% CI 26 to 48%) and 37% in arm B (95% CI 22 to 53%). There were 3 deaths within 30 days of treatment in arm A and one death in arm B. As a confirmatory analysis, rates of grade 3/4 neutropenia and death within 30 days of treatment versus less than 3 neutropenia toxicity were compared between treatment arms using a χ2 test which was also non-significant (p=0.966), table 2.
Grade 3/4 neutropenia and death within 30 days of treatment
Secondary end points
Non-neutropenic toxicities
For non-neutropenic toxicities in the secondary end points, χ2 test for trend was used to assess differences across the toxicity grades. Again as a confirmatory analysis, rates of grade 3 or more versus less than grade 3 toxicity was compared between treatments using a χ2 test, as shown in table 3 nausea/vomiting was not significantly different by grade and no severe mucositis toxicity grade 3–4 was reported. Other chemotherapy-related toxicities were not significantly different between treatment groups. In the chemotherapy alone group, the incidence of fatigue as a toxicity was significantly lower with vitamin supplementation (p=0.003). This result was further explored but not confirmed in the quality of life data.
Maximum common toxicity criteria grade 3/4 toxicities
HC Data
The median level of HC at baseline was 13 (range 7–54 μmol/L). There was no significant difference in HC baseline levels between groups (p=0.9; table 4). Baseline HC concentrations did not predict myelosuppression with regards to the neutrophil count (p=0.75). There were nine patients in arm A (25%) and two in arm B (5%) reporting successful supplementation (at least a 30% decrease of raised HC baseline level). In a post hoc analysis (successful supplementation) did predict less neutropenia when compared to the unsupplemented group (0% vs 69%; p=0.02). None of the nine successfully supplemented patients experienced neutropenia. Of the three deaths in arm A on or within 30 deaths of treatment, two occurred in the unsuccessfully supplemented group and one in the successful supplemented group.
Homocysteine (HC) levels
Survival
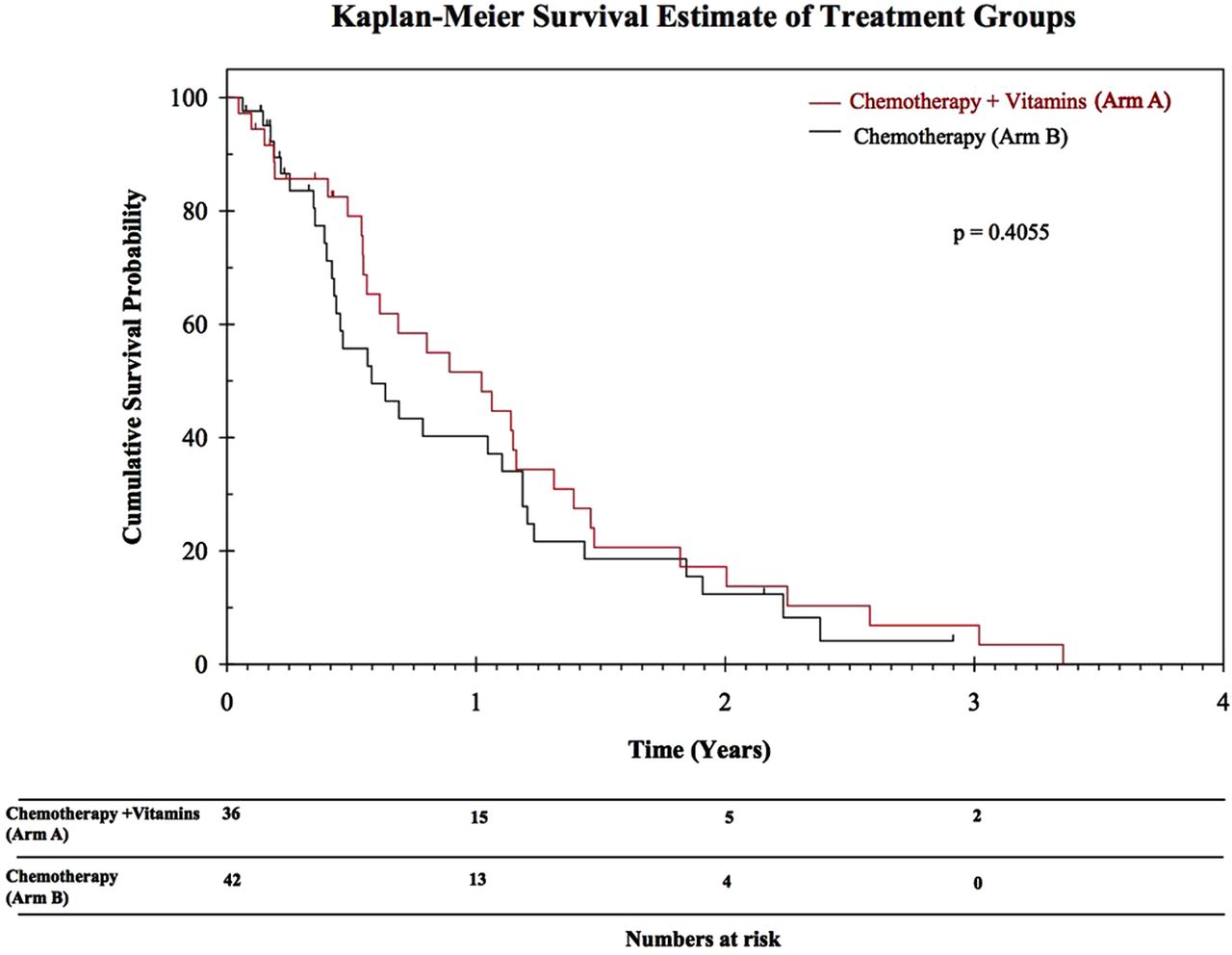
At the time of analysis, 61 out of 78 patients (78%) had died or were lost to follow-up and 17 (22%) were alive. There was no statistically significant difference in survival between the treatment groups with median survivals of 7.0 (chemotherapy alone) and 12.3 months (chemotherapy and vitamin supplementation; p=0.41; figure 2).

{kind=link}
{kind=link}
Kaplan-Meier survival estimate of treatment groups.
Quality of life
Seventy-eight patients completed the quality of life forms. The assessment did not show a significant difference between the treatment groups with regard to the mean change from baseline at 6 weeks and from the baseline at 3 months (table 5). There was no difference in fatigue levels on the quality of life scales (data not shown).
Mean changes of functional scales
Discussion
This single centre phase II study examined the impact of vitamin supplementation on toxicities associated with platinum-based cytotoxic treatment in patients with lung cancer and the potential of HC level as a biomarker for chemotherapy-induced toxicity. The study was negative for its primary end point of decreased neutropenic toxicity in the group receiving vitamin supplementation.
Although the population was mixed, the majority of patients in the study had advanced NSCLC and were receiving first-line chemotherapy. Overall, in comparison with previous studies, there was a similar rate of toxicity of 36–7% grade 3 and 4 neutropenia.2 ,3 The inclusion of second line patients and patients with SCLC increases the rates of neutropenia to around 40–66%, as previously reported.5 ,6
The parameters chosen for assessment of HC in this study were taken from the literature in patients mostly without cancer, although some series using pemetrexed treatment of various types of lung cancer was also used. Neutropenia in itself is sometimes just a paper laboratory value, toxicity not impacting on patient safety or outcome. However grade 3 and 4 neutropenia often leads to sepsis, decompensation and organ failure therefore is usually managed by delaying subsequent chemotherapy, immediate or subsequent prescription of growth factors or antibiotics. Patients with poorer performance status are at high risk of neutropenia grade 3 and 4, neutropenic sepsis and death.14 Growth factors continue to be costly in many countries and an extra burden on patients and staff administering the growth factors. It is therefore appropriate to use grade 3 and 4 neutropenia as an end point in studies of toxicity. The study was powered to show only a large difference in the rate of neutropenia between the two arms (40–10%). The supplemented patients showed no improvement in the rate of neutropenia, which was around 36–7% in both arms as predicted.
There are potential weaknesses with this study, commensurate with a small, single centre phase II study. The study was unblinded and not placebo controlled. However several points of interest are raised. First pretreatment homocysteine levels were high in this patient population suggesting vitamin depletion levels are high in this group. There may be other lifestyle factors affecting homocysteine levels in this patient population but the most likely factor is malnutrition, known to be prevalent in this patient group. As such, management and improvement of malnourishment should be considered in the holistic approach to these patients. Second, only 25% of patients in arm A showed evidence of a successful response to vitamin B12 and folic acid as determined by at least a 30% decrease in HC levels—this has not been reported before. This was a novel and unexpected finding and raises an important question as to the optimal dose of vitamin supplementation. We used the standard dose commonly prescribed in the setting of chemotherapy supplementation. Further work on dose of folic acid and vitamin B12 and monitoring of homocysteine levels may be necessary and useful.
In this study there was an unexpectedly small numbers of successfully supplemented patients, suitable for a true comparison of the intervention. In a post hoc analysis of patients in arm A who were successfully supplemented, there was less neutropenic toxicity compared to unsupplemented patients. This warrants further investigation. If confirmed as a biomarker HC levels could potentially be used to select patients for growth factor use.
In the quality of life data there was a trend to improved quality of life with vitamin supplementation in the physical domain at 6 weeks and 3 months, emotional domain at 3 months and new role, social and global health at 6 weeks. As a non-statistically significant trend this needs to be interpreted with caution. Though analysis of OS showed no statistically significant difference between the two arms it is interesting to note that the median survival of 12.3 months in the vitamin supplemented arm is higher than one might expect from this patient group.
In conclusion, we failed to demonstrate that the use of vitamin supplementation in unselected patients improves the toxicity from platinum-based chemotherapy. Future research is necessary on the dose and schedule of vitamin B12 and folate supplementation to achieve a decrease in HC levels in a greater proportion of patients than was achievable with the schedule used in this study. Interesting post hoc data was generated regarding reduction in neutropenic toxicity in the small group of successfully supplemented patients.
Acknowledgments
The authors acknowledge support from the NIHR Royal Marsden Biomedical Research Centre.
References
Footnotes
-
Contributors MOB, RG, MP, JC, SP made substantial contributions to conception and design. MOB, JB, RG, MP, SKL, KN, JC, SP were involved in acquisition of data. AM, MOB, KS, JB, RG, MP, SKL, KN, JC, KCY, PB, SP took part in analysis and interpretation of data. AM, MOB, KS, JB, RG, MP, SKL, KN, JC, KCY, PB, SP participated in writing and rewriting the paper.
-
Competing interests None.
-
Ethics approval The Royal Marsden Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.