Article Text

Abstract
Introduction Ultrasound measurements of rectus femoris cross-sectional area (RFCSA) are clinically useful measurements in chronic obstructive pulmonary disease (COPD) and critically ill patients. Technical considerations as to the type of probe used, which affects image resolution, have limited widespread clinical application. We hypothesised that measurement of RFCSA would be similar with linear and curvilinear probes.
Methods Four studies were performed to compare the use of the curvilinear probe in measuring RFCSA. Study 1 investigated agreement of RFCSA measurements using linear and curvilinear probes in healthy subjects, and in patients with chronic respiratory disease. Study 2 investigated the intra-rater and inter-rater agreement using the curvilinear probe. Study 3 investigated the agreement of RFCSA measured from whole and spliced images using the linear probe. Study 4 investigated the applicability of ultrasound in measuring RFCSA during the acute and recovery phases of an exacerbation of COPD.
Results Study 1 showed demonstrated no difference in the measurement of RFCSA using the curvilinear and linear probes (308±104 mm2 vs 320±117 mm2, p=0.80; intraclass correlation coefficient (ICC)>0.97). Study 2 demonstrated high intra-rater and inter-rater reliability of RFCSA measurement with ICC>0.95 for both. Study 3 showed that the spliced image from the linear probe was similar to the whole image RFCSA (308±103.5 vs 263±147 mm2, p=0.34; ICC>0.98). Study 4 confirmed the clinical acceptability of using the curvilinear probe during an exacerbation of COPD. There were relationships observed between admission RFCSA and body mass index (r=+0.65, p=0.018), and between RFCSA at admission and physical activity levels at 4 weeks post-hospital discharge (r=+0.75, p=0.006).
Conclusions These studies have demonstrated that clinicians can employ whole and spliced images from the linear probe or use images from the curvilinear probe, to measure RFCSA. This will extend the clinical applicability of ultrasound in the measurement of muscle mass in all patient groups.
- Respiratory Muscles
- COPD Exacerbations
- Imaging/CT MRI etc
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
These studies have shown that a curvilinear ultrasound probe is as effective as a linear ultrasound probe in measuring the rectus femoris cross-sectional area.
Additionally, splicing images using a linear ultrasound probe can also be used to measure the rectus femoris cross-sectional area if an adequately sized linear probe or a curvilinear probe is not available.
Furthermore, using a curvilinear ultrasound probe to the measure rectus femoris cross-sectional area in a cohort of patients with an exacerbation of chronic obstructive pulmonary disease has demonstrated a correlation between the rectus femoris cross-sectional area, and activity.
Introduction
B-mode ultrasound imaging is a widely used technique. More recently, its clinical use has been extended to the assessment of peripheral skeletal muscle wasting, with single and sequential measurement of the quadriceps rectus femoris (RF) muscle cross-sectional area (RFCSA).1–5 RFCSA has been shown to correlate with volitional measures of quadriceps strength1 ,2 and this approach has characterised peripheral muscle wasting in patients with chronic obstructive pulmonary disease (COPD).1 ,2 This non-volitional technique, with high levels of intra-rater and interoccasion reliability,1 ,3 ,4 ,6–8 has been employed by us and by others, as a tool to assess skeletal muscle wasting in critically ill patients.3 ,9 Despite these supportive data, there are limitations to the use of this ultrasound method.
Conventionally, a higher frequency (6–10 MHz) linear ultrasound probe has been used to measure RFCSA, as the high resolution permits clear definition of the border of the quadriceps rectus femoris muscle.10 However, the linear ultrasound probe has limited depth penetration and imaging window width,1 ,10 which can adversely affects the reliability and reproducibility of the measurement. For example, in young critically ill trauma patients with substantial peripheral muscle bulk on admission,3 in those morbidly obese patients with increased subcutaneous fat and in fluid overloaded critical care patients, the image window width and depth limits acquisition of the whole RFCSA image. In contrast, the lower frequency (2–5 MHz) curvilinear ultrasound probe has greater depth penetration10 and window width but lower resolution,10 which has raised concerns about its usefulness when measuring RFCSA.
Recent systematic reviews evaluating the use of muscle ultrasound for measurement of peripheral skeletal muscle reported a paucity of studies investigating the effect of frequency and resolution on muscle area measurements.11 ,12 Indeed, previous studies comparing the use of linear and curvilinear ultrasound probes have been inconclusive, with one study suggesting that there may be a bias towards larger measurements with a linear probe,13 and another demonstrating similarity between the probes.14 One previous study has directly compared the linear and curvilinear probes to measure cross-sectional area, albeit this was a non-clinical study using vessels filled with different density media as the simulation model.15
In the current study, we hypothesised that there would be no difference in RFCSA measurements using a linear and curvilinear ultrasound probe between healthy subjects and patients with chronic respiratory disease, including interoperator and interoccasion measurements using the lower frequency probe. Additionally we hypothesised that spliced images using the linear probe would provide similar RFCSA whole image measurement. Finally, we assessed the clinical feasibility of using the lower frequency curvilinear probe in patients with COPD during the acute and recovery stage of an exacerbation.
Methods
Subjects
Ethical approval for the study was obtained from the local ethical review board (Westminster National Research Ethics Committee). All healthy subjects and patients provided written and informed consent. Healthy volunteer subjects were recruited from laboratory and clinical staff. Patients with stable chronic respiratory disease undergoing assessment for initiation of home mechanical ventilation were recruited from the Lane Fox Respiratory Unit, St Thomas’ Hospital, London, UK, and patients with COPD were recruited during hospital admission for an acute exacerbation.
Validation studies
Four separate validation studies were performed.
Study 1 investigated the agreement of RFCSA measured using linear and curvilinear probes at two-third and three-fifth of the distance between the anterior superior iliac spine (ASIS) and the superior border of the patella, in healthy subjects and in patients with stable chronic respiratory disease (n=32).
Study 2 investigated the intra-rater and inter-rater agreement using the lower frequency curvilinear probe. Intra-rater reliability measurements were made in 10 healthy subjects who had RFCSA measurements taken at two-third and three-fifth the distance between ASIS and the superior border of the patella on two separate occasions using the curvilinear ultrasound probe, within 10 days of each other, by one operator (SM). Inter-rater reliability measurements were made in 10 participants with chronic respiratory failure (7 with COPD and 3 with obesity hypoventilation syndrome), who had RFCSA measurements performed on the same day by two independent operators (SM and AT), using the curvilinear ultrasound probe. For each patient, each operator took three measurements at two-third and at three-fifth distance from ASIS to superior boder of the patella.
Study 3 investigated the agreement of RFCSA measured from whole and ‘spliced’ images using the higher frequency linear probe in healthy subjects and in those with stable chronic respiratory failure (n=32).
Study 4 investigated the clinical applicability of ultrasound measurements using the lower frequency curvilinear probe to track the change in RFCSA and, in particular, to investigate the relationship between changes in RFCSA and physical activity, during the acute and the recovery phases of an exacerbation of COPD (n=18).
RFCSA measurement protocol
Whole image aquistion—RFCSA was measured at two-third and three-fifth distance from ASIS to the superior border of the patella. The patient was placed in a semirecumbent position with a pillow under the knee. The probe was placed perpendicularly to the long axis of the femur, as previously reported, with minimal change in the angle of the probe.1 ,16 ,17 The operator positioned the probe on the surface of the thigh to avoid distorting the underlying tissue. Measurements were taken in a standardised manner—RFCSA measurements were taken by the liner probe first and then by the curvilinear probe. Real-time, B-mode ultrasound images were acquired using a 6 MHz linear probe with a 38 mm array (Sonosite S-ICU, SonoSite Inc, Japan) and 2–5 MHz curvilinear probe with a 60 mm array (Sonosite S-ICU, SonoSite Inc). The mean value of three consecutive measurements of RFCSA using each ultrasound probe was recorded.
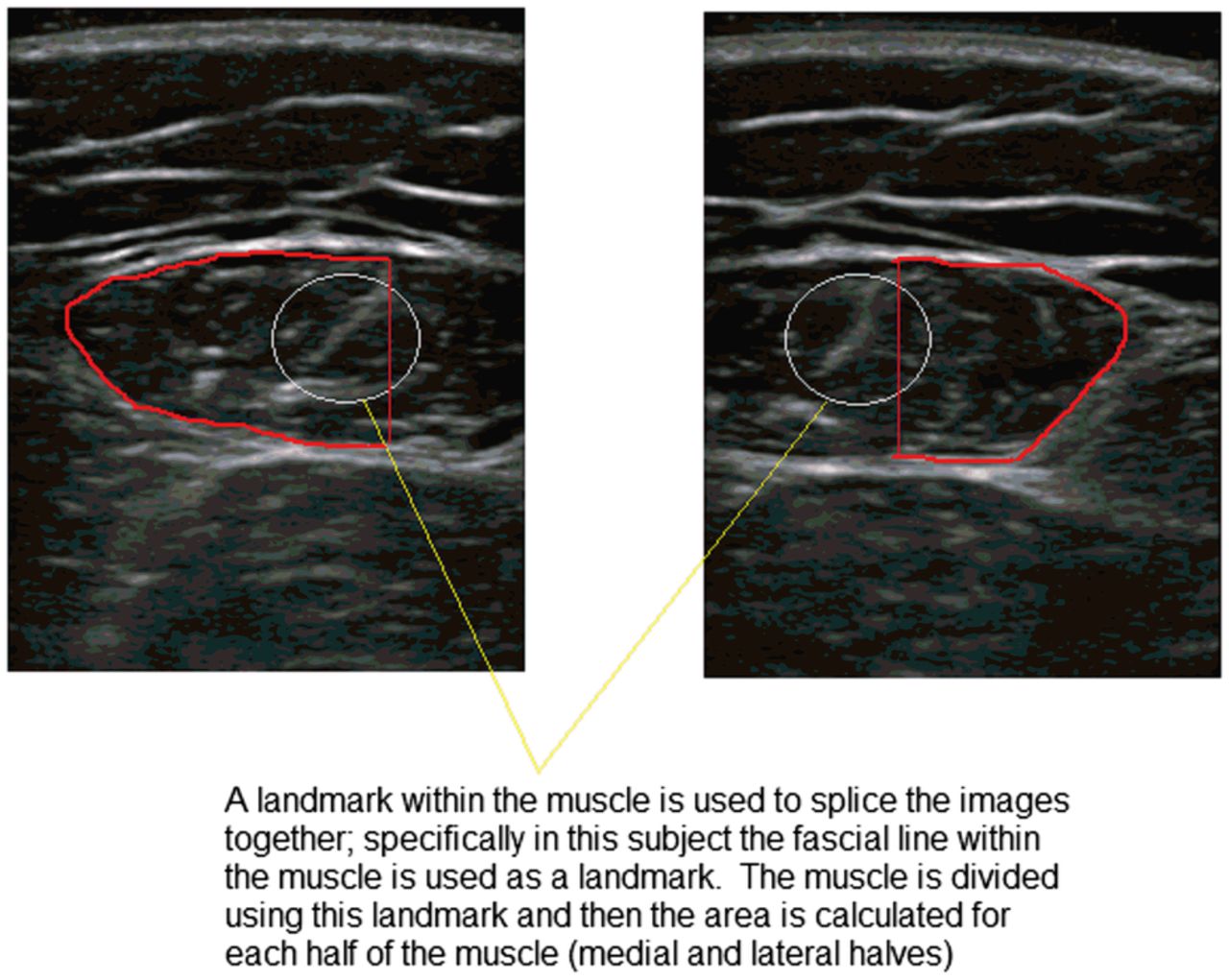
Spliced image aquistion—Whole and matched ‘spliced’ RFCSA images were acquired using the linear ultrasound probe at both two-third and three-fifth distance. RFCSA measurements were calculated off-line using the Image J program (National Institutes of Health, Maryland, USA). Both operators took images sequentially and then analysed results off-line at a later date so as to be blinded to the results. Spliced measurements involved taking two images, one of each half of the RF muscle, at the same point, for example, at three-fifth distance, one image of the lateral half of the RF muscle and at the same point an image of the medial half of the RF muscle. A landmark within the muscle was used as the point at which each half of the muscle would be measured so as to avoid overlapping of the images (figure 1). The two measurements of each half of the muscle (lateral and medial) were summated to provide the overall ‘spliced image’ cross-sectional area.
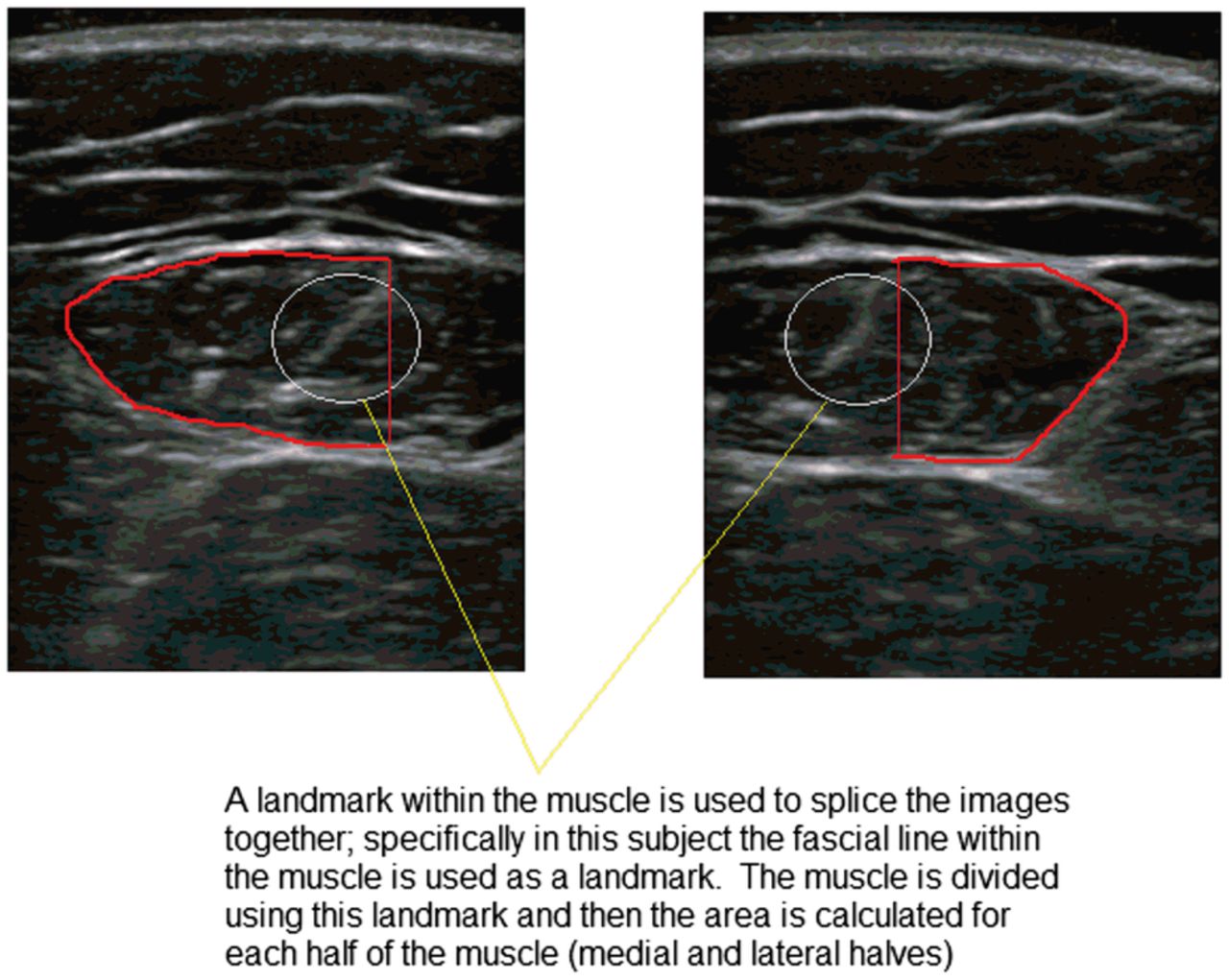
A representative example of imaging splicing.
Physical activity measurement
A subset of patients admitted with an acute exacerbation of COPD (AECOPD) also wore a uniaxial accelerometer activity monitor (Actiwatch Spectrum, Phillips Respironics, Murraysville, Pensylvania, USA) during their hospital admission, to assess the relationship between changes in RFCSA and physical activity.18–21 Patients were requested to wear the accelerometer for the duration of hospital stay as well as for 28 days following hospital discharge. Participants were asked to wear the accelerometer for 24 h/day. Data for inpatient admission were included if the accelerometer was worn for a minimum of 3 days and at least for 10 h during the daytime to allow assessment of physical activity. For follow-up data, an average of 7 days of data was used to assess physical activity.
Statistical analysis
Results are presented as mean±SD, unless otherwise stated. Statistical analysis was performed using Prism V.6 (Graphpad, California, USA). Independent t tests and Bland-Altman analysis were used to compare the two modes of scanning, and intraclass correlation coefficients (ICC) were calculated to determine agreement between the two methods.
Results
Study 1: RFCSA agreement between the linear and curvilinear probe
Participants
Fifty consecutive participants were enrolled (37 healthy subjects and 13 patients with chronic respiratory failure). Participants were not excluded on the basis of body mass index (BMI). Of those with chronic respiratory failure, 12 had COPD and 1 had restrictive lung disease. The ages of the healthy cohort and chronic respiratory failure cohort were 36±9 and 72±10 years, respectively.
Whole RFCSA image acquisition using the linear and curvilinear probes
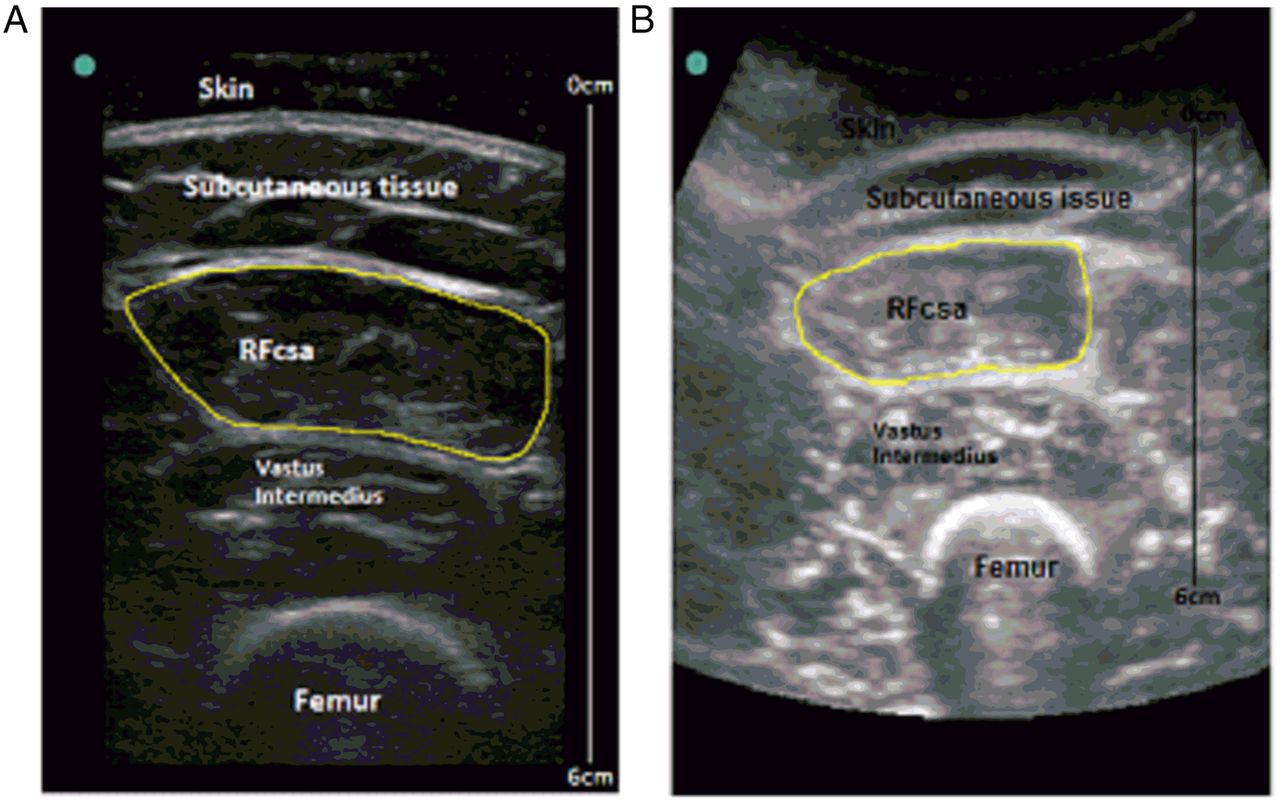
Thirty-two participants had whole RFCSA image aquisition using the linear probe visualised at the two-third and 14 at three-fifth distance from the ASIS and patella (figure 2A, B), the remaining 18 and 36 participants, respectively, could not have their RFCSA wholly visualised with the linear probe. The main reason the muscle could not wholly be visualised at three-fifth distance was due to the muscle being too large to fit the width of the probe. However, all participants had whole RFCSA image aquisition using the curvilinear probe. The age of these 32 participants was 49±21 years (patient cohort (n=13) 72±10 years; healthy cohort 32±4 years).

Rectus femoris cross-sectional area (RFCSA) image acquired using (A) linear ultrasound probe at two-third distance (same subject) and (B) curvilinear ultrasound probe at two-third distance (same subject).
RFCSA agreement measured at two-third distance from ASIS and superior border of the patella
There was no difference between RFCSA measurements using the linear and curvilinear probes at two-third distance from ASIS and superior border of the patella (308±104 mm2 vs RFCSA 320±117 mm2, 3.8% difference; p=0.80). The ICC was 0.97 (table 1). Bland-Altman analysis of linear and curvilinear RFCSA measurements demonstrated the majority of values within the 95% confidence limits of −62.4 to 39.4 with a bias of −11.6±26.0 mm2 (figure 3A). The mean coefficient of variation (CV) was 2.6% for linear images and 2.6% for images taken with the curvilinear probe.
RFCSA measurements taken by linear and curvilinear probes
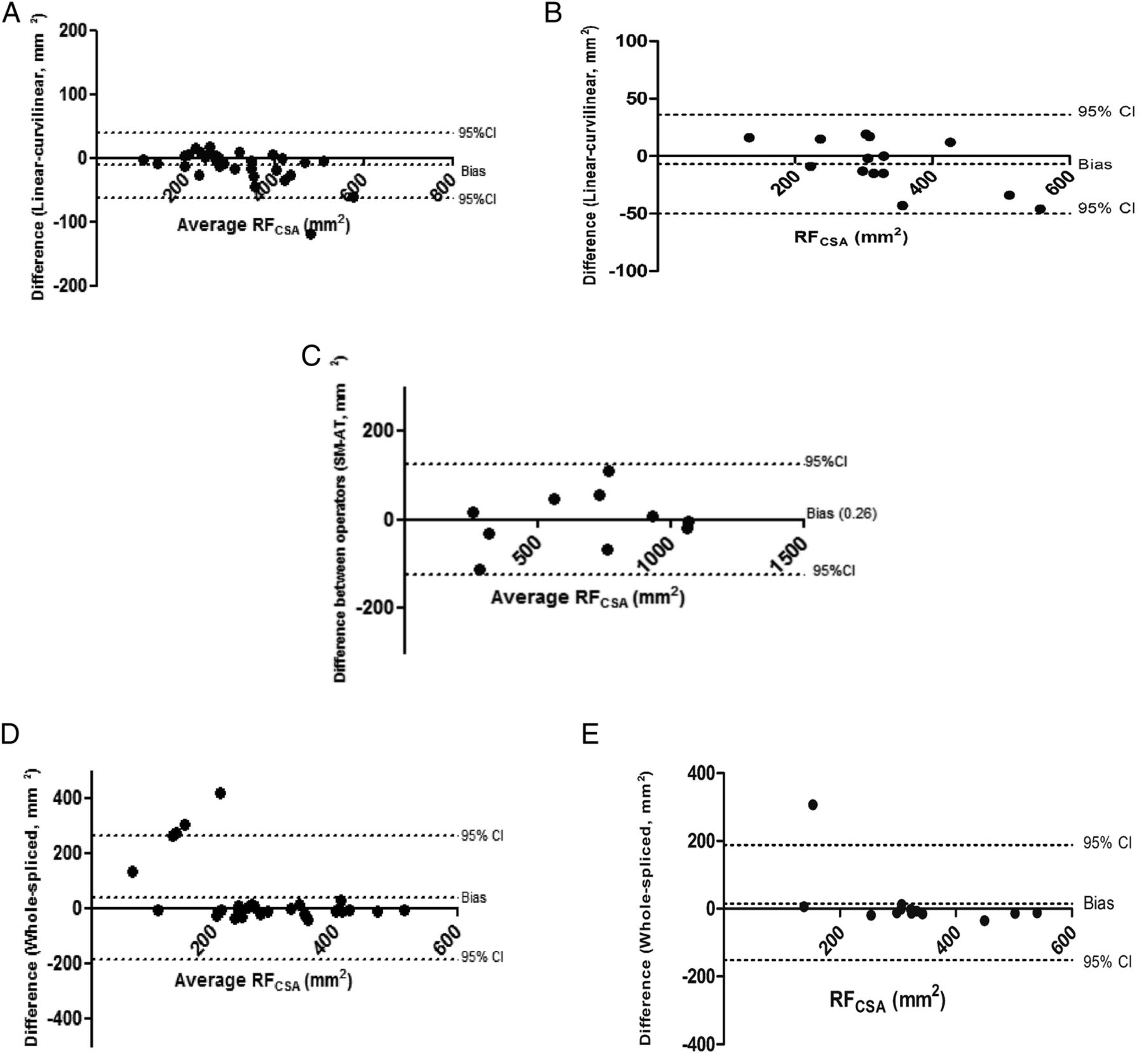
(A) Bland-Altman plot of linear probe and curvilinear probe rectus femoris cross-sectional area (RFCSA) measurements at two-third distance from anterior superior iliac spine and patella. (B) Bland-Altman plot of linear probe and curvilinear probe RFCSA measurements at three-fifth distance from anterior superior iliac spine and patella. (C) Bland-Altman plot of two independent operator measurements of RFCSA using a curvilinear probe at three-fifth distance from anterior superior iliac spine and patella. (D) Bland-Altman plot of whole and spliced RFCSA measurements using linear probe at two-third distance from anterior superior iliac spine and patella. (E) Bland-Altman plot of whole and spliced RFCSA measurements using linear probe at three-fifth distance from anterior superior iliac spine and patella.
RFCSA agreement measured at three-fifth distance from the ASIS and superior border of the patella
There was no difference between RFCSA measurements taken using the linear and curvilinear probes (327±103 vs 334±117 mm2, 2.1% difference p=0.93) at three-fifth distance from the ASIS and superior border of the patella with an ICC of 0.98 (table 1). CV for whole linear images was 2.3% and 2.2% for images taken with the curvilinear probe. Bland-Altman analysis demonstrated a bias of −7.0±22.2 mm2 (figure 3B) with all values lying within the 95% confidence limits (−50.5 to 36.5).
Comparison of healthy subjects and patient cohort at two-third distance from ASIS to the patella
At two-third distance from ASIS to the patella, the RFCSA measurement in the patient cohort was 246±79 vs 251±85 mm2 for linear and curvilinear probes, respectively (2.0% difference), with CVs of 2.7% and 4.1%. The ICC for these measurements was 0.98. For the healthy subjects the measurements taken using the linear and curvilinear probes were 351±97 and 366±115 mm2 (4.3% difference), respectively. The CV for the linear probe measurements was 2.7% and for curvilinear probe 2.4%, with an ICC of 0.95.
Study 2: Intra-rater and inter-rater agreement of RFCSA measurement using a curvilinear probe
Participants
Ten healthy subjects were recruited, eight females (32±6 years) with RFCSA measurements performed on two separate occasions.
Intra-rater agreement
RFCSA at two-third distance from ASIS to patella at visit 1 was 558±141 mm2 and at visit 2, 549±129 mm2 (1.6% difference), with a CV of 2.5%. At three-fifth distance from ASIS and patella, the RFCSA for visit 1 was 699±164 mm2 and for visit 2, 703±164 mm2 (0.5% difference), with a CV of 2.6%. Overall, the ICC for all measurements, at two-third and three-fifth distances, was 0.98 (operator SM).
Inter-rater agreement
Ten patients with chronic respiratory failure were recruited, including five males (70.2±10.3 years) with a BMI of 33.6±8.9 kg/m2. At two-third distance, the RFCSA was 531±249 mm2 (operator SM) and 513±215 mm2 (operator AT), demonstrating a 3.4% difference between the two measurements, with respective CVs for the measurements of 4.1% and 4.0%, and an ICC of 0.88. At three-fifth distance, there was no difference in RFCSA measurements between the two operators, for operator SM, the mean RFCSA was 672±249 mm2 and for operator AT, 672±302 mm2, with CVs of 3.6% and 7.9%, respectively. The ICC was 0.98. Bland-Altman analysis demonstrated satisfactory agreement between the operators (figure 3C). The overall ICC, using RFCSA data from the two-third and three-fifth distances, was 0.95.
Study 3: RFCSA agreement measured from whole and spliced images using the linear probe
Participants
Comparison of the whole and spliced image RFCSA measurement using the linear probe from the healthy subject and patient cohorts in study 1 was performed (n=32).
RFCSA measured at two-third distance from ASIS and superior border of the patella
There was no difference between the whole and spliced RFCSA measurements taken using the linear probe (308±104 vs 263±147 mm2, 14.6% difference; p=0.34), with an ICC of 0.98. CV was 3.1% for spliced linear images. Bland-Altman analysis of whole and spliced linear RFCSA measurements demonstrated the majority of values were within the 95% confidence limits of −188.4 to 262.4, with a bias of 37.0±115.0 mm2 (figure 3D).
RFCSA measured at three-fifth distance from ASIS and superior border of the patella
There was no difference between the whole and spliced linear RFCSA images (321±144 vs 327±103 mm2, 1.9% difference; p=0.82), with an ICC of 0.99. CV was 5.4% for the spliced images. Bland-Altman analysis demonstrated a bias of 15.1±88.5 mm2, again with the majority of values lying within the 95% confidence limits (−158.5 to 188.6 mm2, figure 3E)
With retrospective analysis, a difference was demonstrated in the time taken to perform the scans using the spliced method compared to using whole image acquisition (3.3±1.5 min vs 1.5±0.9 min, p=0.002).
Study 4: To investigate the relationship between RFCSA and physical activity during the acute phase and recovery phase of an exacerbation of COPD
Patients
Seventeen patients were recruited. Baseline characteristics are reported in table 2. RFCSA was measured within 48 h of admission to hospital and at 4 weeks postdischarge. RFCSA measurement at admission was 536±310 mm2 at three-fifth the distance and 427±249 mm2 at two-third the distance from ASIS to patella, measured using a curvilinear probe. At neither the three-fifth distance (−9±230 mm2, 4.8%; p=0.67) nor at the two-third distance (−22.4±158 mm2, 0.6%; p=0.52) was there change in RFCSA between admission and follow-up at 4 weeks.
Baseline characteristics of COPD exacerbation cohort
Relationship between physical activity and RFCSA during AECOPD
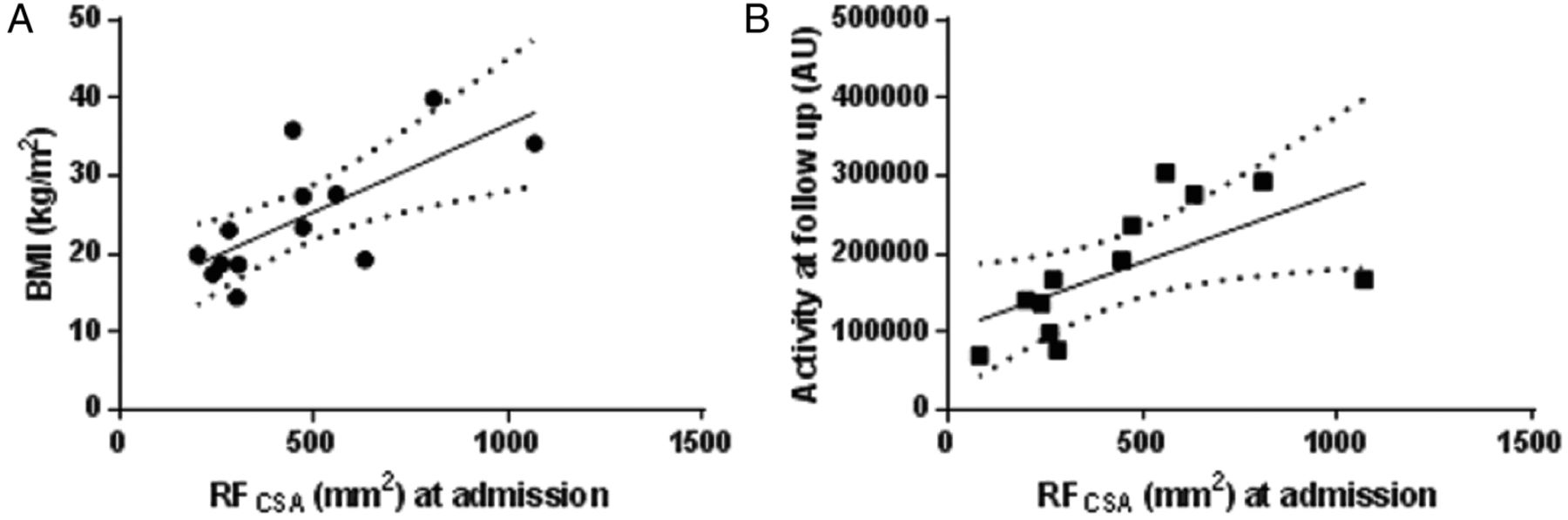
Sixteen of the participants underwent triaxial accelerometer activity monitoring during hospital admission and during the 4-week follow-up period after discharge. There was a direct correlation observed between admission RFCSA (532±319 mm2) and BMI (24.8±7.7 kg/m2; r=+0.65, p=0.018, figure 4A), and between RFCSA at admission (532±319 mm2) and activity levels at 4 weeks post-hospital discharge (activity count 150 610±91 006 AU; r=+0.75, p=0.006). Interestingly, there were no correlations observed between RFCSA at admission and age, length of stay or exacerbation frequency. At 4 weeks post-hospital discharge, 12 patients had continued to wear the accelerometer, with a direct relationship observed between: RFCSA (409±192 mm2) and activity count (180 735 ±78 702 AU; r=+0.76, p=0.006, figure 4B); and RFCSA and BMI (r=0.58, p=0.04). There were no correlations observed between forced expiratory volume at 1 s and age, or activity levels.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Correlation between rectus femoris cross-sectional area (RFCSA) at admission and body mass index. (B) Correlation between RFCSA at admission and activity at 4-week follow-up.
Discussion
The current study has demonstrated that, despite the technical limitations of using the lower frequency curvilinear ultrasound probe, particularly in terms of image resolution, the measurement of RFCSA using the curvilinear probe has satisfactory agreement with the measurement obtained using the standard higher frequency linear probe. The curvilinear probe demonstrated superiority over the linear probe, as it was able to acquire, on every occasion, the whole RFCSA image whereas this was not possible using the linear probe, especially in patients with substantial muscle bulk and excess subcutaneous fat. Furthermore, fewer whole RFCSA images were acquired by the linear probe at three-fifth distance from the ASIS to the superior border of the patella compared to two-third distance, and the clinician should consider using the lower frequency curvilinear probe when using the three-fifth landmark distance. In addition, the curvilinear probe was shown to have satisfactory inter-rater and intra-rater agreement, which has confirmed the clinical usefulness of the curvilinear probe. Moreover, the inter-rater and intra-rater RFCSA agreement of the curvilinear probe was greater at three-fifth distance, and this further supports the use of the lower frequency curvilinear probe at three-fifth distance from the ASIS to the superior border of the patella. There was no difference between the spliced and whole image measurement of RFCSA when using the linear probe, albeit it must be acknowledged that the difference between the whole and spliced images was less at three-fifth distance from ASIS to the superior border of the patella, and thus, if the clinician uses the spliced image, the three-fifth distance would be preferred. Finally, the curvilinear probe has clinical acceptability to monitor the trajectory of change of RFCSA in patients with COPD during the acute and recovery stage of an exacerbation.
Technical implications of the study
Image acquisition using the curvilinear probe showed satisfactory inter-rater, intra-rater and interoccasion reliability. This is consistent with a previous non-clinical study that investigated the differences between the curvilinear and linear ultrasound probe using fluid-filled vessels as the test objects. In the study by Warner et al, the intra-rater and inter-rater reliabilities were high, however, the differences in measurements between the two probes varied with the simulation and the model of ultrasound machine employed, albeit the difference was small at <50 mm2. Furthermore, in agreement with Hammond et al,8 we have shown high intertransducer, inter-rater, intra-rater and intraoccasion agreement. It must be highlighted, however, that the study by Hammond et al8 was performed on a small group of participants and, surprisingly, the measurements were performed at three-fourth the distance between the ASIS and superior border of the patella, a distance that has not been validated against quadriceps muscle strength, quadriceps muscle endurance, exercise capacity or other clinical variables, unlike the three-fifth and two-third distances.1–3
The current study has demonstrated that the splicing method could be the technique to use if an adequately sized linear probe or curvilinear probe is not available, and that this technique can be used in healthy, chronic and acute patient populations. In addition, the measurements of RFCSA by linear and curvilinear ultrasound probes are not significantly different, as demonstrated by the small differences between measurements, high ICC and low CV. The ICC using the curvilinear probe and splicing images using a linear probe was 97%, indicating that both techniques could be used to measure RFCSA in patients in whom a linear probe is unable to visualise the whole area of the muscle. This is wholly relevant to the RFCSA measurement at three-fifth distance from ASIS to the superior border of the patella, as fewer whole RFCSA images were acquired by the linear probe at this landmark.
Clinical implications
Similarity between measurements of the RFCSA using different techniques
These findings have demonstrated that RFCSA measurements obtained using three different methods (linear whole images, spliced linear images and images from a curvilinear probe) are equally effective in measuring RFCSA, with the understanding that using a linear or curvilinear probe is preferential to the splicing method, due to the greater variability in measurements with this method. Indeed, the present data support the use of the lower frequency curvilinear probe at three-fifth distance from ASIS to superior border of the patella. This is clinically important since respiratory and critical care departments will have an ultrasound available for venous line insertion and pleural ultrasound with at least one of the probes available. Furthermore, in clinical cases where sequential or follow-up scans are required, these should, based on the current data, be performed with the same probe. This has particular clinical utility in the measurement of RFCSA in patients with high muscle mass, such as young critically ill trauma patients, and patients with an increased subcutaneous layer such as caused by fluid overload and obesity, where depth penetration as well as an extended window width are required.
Application in the acute setting
Ultrasound has previously been used to monitor changes in RFCSA in the critically ill,3 to measure response to resistance training in COPD and healthy subjects,22 and to correlate RFCSA with muscle strength.1 These studies have all used a linear probe. To the best of our knowledge, this is the first study to use a curvilinear probe to track changes in RFCSA. Although the study numbers were small in the acute exacerbation cohort, these preliminary data are novel and hypothesis generating. In addition to demonstrating that the curvilinear ultrasound probe can be used to track changes in acutely unwell patients with COPD, we have shown correlations between RFCSA at admission and body composition as well as the level of physical activity at 4 weeks. Indeed, in a subgroup of these patients, we observed a direct positive relationship between RFCSA and physical activity at 4 weeks following hospital discharge. This approach could have clinical importance in patient selection, to identify those acute patients most likely to benefit from rehabilitation, which may, in part, explain the lack of improvement with rehabilitation in a recently published trial on these patients.23 ,24 Additionally, Greening et al25 showed that RFCSA was associated with readmission and mortality following admission with an exacerbation of COPD, which highlights the requirement to have robust measures to track the change in RFCSA during an exacerbation. The data we have presented from four studies performed in this paper were detailed physiological studies, and it is interesting that there were no correlations between RFCSA and frequency of exacerbations; this may have been due to small sample size—larger studies will be required to confirm or disprove these findings.
Limitations of the study
In contrast to CT and MRI, which are relatively operator independent, ultrasound is an operator-dependent mode of imaging and errors in measurements can occur. However, we have shown in the current study that the ultrasound images obtained, using both, the linear and curvilinear probes were similar, with high intra-rater and inter-rater agreement with both probes. This was achieved, in part, by the scans being performed by two experienced operators and, in particular, attention was focused on ensuring an optimal standardised operating protocol for measurement acquisition including avoidance of muscle compression, and accurate probe position perpendicular to the long axis of the femur. A major limitation of the spliced image method acquired using the linear ultrasound probe was that it required increased time for image acquisition compared to the whole image acquisition technique. This extended time requirement is also likely to apply to image analysis time, however, this calculation was not possible retrospectively. There was no difference in the time taken to obtain images using a curvilinear probe compared to a linear probe, but there was, as expected, a difference between using the curvilinear probe and linear splicing method. Although the difference in RFCSA measurements using the spliced method at two-third distance was not significant, the difference was larger than those obtained using the other methods. While the authors acknowledge that there was a difference in the spliced measurements at two-third distance from ASIS to the superior border of the patella, this difference was not present at the three-fifth distance, and as there is no currently established minimal clinically important difference (MCID) for change in RFCSA, further research is required to determine the MCID in various patient groups. Finally, we acknowledge that there was a difference in the width of the probes, which resulted in fewer whole images being captured by the linear probe, albeit that this probe has been commonly used in previous studies.1 ,3 ,12 ,26 The authors acknowledge that the shape of the probe will influence the ability to image the underlying muscle in detail, however, the linear probe is currently the most common probe used in practice. These current data support the use of the splicing technique employing the linear probe, if a curvilinear probe is not available, and that the measurement should be taken at three-fifth distance. The authors acknowledge that the sample sizes were small and future work is required to confirm these data in large populations, particularly, looking at the correlations in the COPD population, sample size calculations will need to be calculated in order to detect differences.
Conclusion
In healthy subjects and patients with chronic respiratory disease, the data from these detailed physiological studies have demonstrated that the use of the lower frequency curvilinear probe is not inferior to that of the higher frequency linear probe in measuring RFCSA. Furthermore, there was strong intra-rater and inter-rater agreement in the use of the curvilinear probe to measure RFCSA. The RFCSA spliced image method has limitations and it should only be used when a curvilinear probe is not available, and the clinician should use the same method to measure RFCSA when acquiring sequential follow-up data. The use of the curvilinear ultrasound probe has been validated in both, stable and acute patients with chronic respiratory disease, which will permit extension of the use of the curvilinear probe to patients where the image depth pentration and width capture requirements are greater, such as young trauma patients with high muscle bulk, morbidly obese patients with significant subcutaneous fat and patients with fluid overload.
References
Footnotes
Contributors SM and NH designed the study. SM, ES, AT and RH were involved in data collection. SM was responsible for data analysis. SM, ES, AT, RH, MR, BC, ZP, JM and NH were involved with drafting and in review of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Westminster National Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.