Article Text

Abstract
Introduction Janus kinases (JAKs) regulate inflammatory gene expression through phosphorylation of signal transducer and activator of transcription (STAT) proteins. Expression of STAT proteins is increased in chronic obstructive pulmonary disease (COPD), and may be involved in driving chronic inflammation. Oral JAK inhibitors are effective as anti-inflammatory therapy but exhibit dose-limiting adverse effects. Development of inhaled compounds would be enhanced by robust biomarkers that directly reflect the anti-inflammatory and pharmacological activity in the lung.
Methods A novel flow cytometry assay was developed to measure STAT1 phosphorylation in sputum inflammatory cells. The standard sputum processing method was refined to improve sputum cell viability. The flow cytometric assay was used to assess the reproducibility of the measurement of STAT1 phosphorylation and the in vitro activity of a pan JAK-inhibitor on three separate visits in patients with COPD.
Results Upregulation of STAT1 phosphorylation was measured following in vitro IFNγ stimulation of sputum macrophages (stimulated/unstimulated ratio 1.57; p<0.00001). Upregulation was inhibited following in vitro preincubation with a pan JAK-inhibitor (inhibited+stimulated/unstimulated ratio 0.97). STAT1 phosphorylation activity could only be measured in macrophages.
Conclusions Sputum from patients with COPD can be used to reproducibly measure phospho-STAT expression in sputum macrophages. The flow cytometry-based method can be used to evaluate kinase inhibitors in vitro and subsequently in ex vivo studies. The assay is particularly useful for the assessment of inhaled compounds where whole blood assays may not be relevant.
- COPD Pharmacology
- Cytokine Biology
- Macrophage Biology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
A novel flow cytometric based method has been developed to measure kinase inhibition in induced sputum by measuring intracellular phosphorylation of components of the JAK/STAT pathway.
This work highlights that macrophages play an important part in the JAK/STAT pathway of inflammation.
This novel biomarker method details a unique application for the evaluation of inhaled kinase inhibitors as therapeutic agents in the treatment of lung disease and could prove a valuable tool in drug development.
Introduction
The regulation of protein function in mammalian cells is controlled via reversible protein phosphorylation mediated by protein kinases. Kinases, of which there are over 500 types, are the enzymes responsible for critical signalling pathways in all cell types. There has been recent interest in the use of kinase inhibitors for the treatment of chronic obstructive pulmonary disease (COPD) and asthma-COPD overlap syndromes via targeting neutrophilic inflammation and reversing steroid resistance.1 ,2 Kinase inhibitors are not specific for a single kinase, but usually inhibit several kinases which may result in off-target adverse effects.3
Janus kinases (JAKs) are non-receptor tyrosine kinases activated by various cytokine receptors, and regulate the expression of multiple inflammatory genes through phosphorylation of STAT proteins.4 JAK1/3 heterodimers regulate T-cell survival, whereas JAK2 mediates granulocyte-macrophage colony-stimulating factor-mediated neutrophil survival in addition to interferon-γ (IFNγ) and interleukin (IL)-12/IL-23 signalling. STAT4 is activated by IL-12 and IL-23, STAT5 by IL-2, whereas STAT6 is activated by IL-4 and IL-13. JAK-STAT signalling is activated in several inflammatory and immune diseases, leading to the development of inhibitors of this pathway, such as selective JAK inhibitors. Inflammation is increased in the respiratory tract in patients with COPD and, by analogy, with rheumatoid arthritis and inflammatory bowel disease it would be expected that JAK-STAT signalling is also involved in the chronic inflammation of patients with COPD. STAT4 is activated in lung parenchyma of patients with COPD.5
STAT phosphorylation can be detected easily by western blotting, but this cannot identify activation in specific cell types in a mixed population. Flow cytometry has been used to detect intracellular STAT1 phosphorylation in whole blood assays and peripheral blood mononuclear cells (PBMC),6 ,7 but not in sputum.
The selective JAK inhibitor, tofacitinib, inhibits JAK1, JAK3 and, to a lesser extent, JAK2 and tyrosine kinase 2 (TYK2), resulting in inhibition of STAT phosphorylation. This orally administered drug has been approved for clinical use for the treatment of rheumatoid arthritis, and has also shown clinical benefit in a wide range of other inflammatory diseases. Tofacitinib, in common with other oral JAK inhibitors, is associated with significant adverse effects, especially when used in higher doses.8 These complications limit the dose of drug that can be delivered systemically. In early studies with tofacitinib, whole blood assays were used to establish the mechanism of action of these drugs to inhibit the STAT phosphorylation pathway in leucocytes, whole blood or PBMC.
Other more recent compounds in development include pan-JAK inhibitors which have been shown to suppress STAT1 phosphorylation and inhibit the release of proinflammatory cytokines.9 These have a rapid systemic clearance and so, when given by the inhaled route, may maximise local anti-inflammatory activity while minimising systemic adverse events.10 Inhaled drugs may be the preferred route of administration for the treatment of inflammatory lung diseases, such as COPD. However, blood assays cannot be used to measure the effect of inhaled JAK inhibitors, as drug concentrations in the systemic circulation are designed to be low. This means that it is necessary to measure JAK-STAT inhibition in cells from the respiratory tract.
We have developed an assay system to measure STAT phosphorylation in sputum samples using flow cytometry. The measurement of STAT phosphorylation enables direct assessment of the efficacy and sensitivity of kinase inhibitor compounds, particularly those delivered via the inhaled route of administration to the lungs. The intracellular flow cytometry method identifies the specific cell populations that express phosphorylated STAT in sputum. The flow cytometry-based method is complemented by the additional measurements of cell types and cytokine levels. This biomarker method can be used to evaluate the efficacy and/or sensitivity, as well as the choice of a suitable dose range and/or dosage regimen for an inhaled kinase inhibitor.
Methods
Study design
The study was carried out according to The Code of Ethics of the World Medical Association (Declaration of Helsinki), and was approved by the National Research Ethics Service Committee London, Hampstead, Northwick Park Hospital REC Centre (REC reference 12/LO/0579). All individuals provided written informed consent.
A pilot study11 was undertaken to determine assay conditions which were subsequently used in the main study. Induced sputum samples were obtained from patients with COPD (n=6) and healthy smokers (n=3).
In the main study, sputum samples were obtained from 15 patients with established COPD (see below). Repeat samples were obtained on at least two occasions 1 week apart during three separate visits. The aim of the study was to establish an ex vivo method for the measurement of JAK activity by measuring STAT phosphorylation using flow cytometry in cells obtained from induced sputum. Separate cell fractions were measured unstimulated, after cytokine stimulation and after preincubation with a pan-JAK inhibitor plus cytokine stimulation. In addition, each sputum sample was analysed for differential cell count, and after sputum processing using a modification of standard methods, a multiplex analysis system was used to measure chemokines and cytokines.
Patients
The study included 15 evaluable patients with COPD who were current or ex-smokers. The demographic characteristics of the patients are presented in table 1. Patients with COPD were to have had a diagnosis, for at least 6 months, of moderate to severe COPD and met the criteria for GOLD category II–III disease12 (table 1). Patients had not taken oral corticosteroids within 3 months of visit 1, inhaled corticosteroids within 4 weeks of visit 1, or leucotriene modulators within 2 weeks of visit 1.
Demographic characteristics of patients with COPD included in the study
Primary and secondary evaluations
The primary end point for the study was STAT1 phosphorylation in sputum macrophages (non-stimulated and/or stimulated cells±JAK inhibitor). The secondary end points for the study were the sputum cell count data (total cell count; total neutrophil count and differential cell count (%); total macrophage count and differential cell count (%)), and selected biomarker end points: CXCL8, CXCL9, CXCL10, CXCL11, CCL2, CCL4, CCL5, IL-1β, IL-6, eosinophil cationic protein (ECP), neutrophil elastase (NE) and α2 macroglobulin.
Sputum induction
The study comprised three visits with each visit separated by at least 7 days. At visit 1, provided all other inclusion/exclusion criteria were satisfied (except laboratory test values which were reviewed as soon as they were available), the patient underwent sputum induction as previously described using nebulised 3–5% saline.13 ,14 If all entry criteria were met, the patient progressed to visits 2 and 3. At visits 2 and 3, an induced sputum sample was obtained. If a patient was unable to produce an evaluable sample at any visit, they could undergo a single additional visit (at least 4 days following the previous induction). An evaluable patient was defined as a patient who met all the inclusion and exclusion criteria, and produced at least two sufficient sputum samples which were evaluable for flow cytometry, cell count and cytokine analyses.
An evaluable sample was defined as >80% viability, <20% squamous cells, a minimum of 0.1 g in sputum weight and >2×106 total cells.
Sputum samples were processed using a technique adapted for intracellular STAT phosphorylation analysis. Established techniques using dithiothreitol (DTT, Sigma-Aldrich, UK),15 were adapted to decrease DTT concentration while retaining sufficient mucus liquefaction. Sputum plugs were selected for processing, the volume of the selected sputum sample measured and an equal volume of Dulbecco's phosphate buffered saline (DPBS, Sigma-Aldrich, UK) added. A reducing agent was added in order to liquefy the sample. DTT at a final concentration of 0.05% (w/v) was used to break the disulphide bonds in the mucus; this is a significantly lower concentration than is standard for sputum samples.
The tube was placed on a plate shaker at 300 rpm for 45 min; a longer incubation time than standard sputum processing techniques. The sample was centrifuged at 258 g for 10 min. The sputum supernatant was separated and retained for cytokine/chemokine analysis, while the cellular components of the sample were used to assess total cell counts, cell differential counts and STAT phosphorylation.
JAK inhibitor
PF-956980 is a pan-JAK inhibitor which inhibits STAT phosphorylation. Previous in vitro and ex vivo work on this compound has shown it to have a significant inhibitory effect with IC50 values of 4–121 nM.16 ,17
Cell preparation for STAT phosphorylation analysis
Isolated sputum cells were allowed to rest at 37°C for 1 hour. Cells were added to tubes containing PF-956980 (or DPBS) at a final concentration of 10−5 M before the addition of IFNγ (R&D Systems, Abingdon, UK) (or DPBS) at a final concentration of 10 ng/mL and incubated at 37°C for 20 min. Samples were then centrifuged at 258 g for 5 min at room temperature and the cells resuspended in 4% (w/v) paraformaldehyde (Sigma-Aldrich, Poole, UK) in DPBS at 37°C for 15 min in order to fix the cells. A further centrifugation at 258 g for 5 min at room temperature was followed by resuspension in 100% ice-cold methanol (Sigma-Aldrich, UK), and incubation on ice for 20 min in order to permeabilise the cells. The samples were centrifuged at 258 g for 5 min at room temperature, and Alexa Fluor 647-conjugated anti-pSTAT1 antibody (or isotype control) (BD Biosciences, Oxford, UK) was added for 30 min at room temperature in the dark. The samples were centrifuged at 258 g for 5 min at room temperature and suspended in DPBS containing 2% (v/v) human serum (Sigma-Aldrich, UK) and analysed using a FACSCanto II Flow Cytometer (BD Biosciences, UK).
Analysis of selected biomarker end points
Selected biomarkers in induced sputum supernatant were analysed using Luminex technology or ELISA. The following analytes were measured using Luminex technology kits (R&D Systems, Abingdon, UK) as per manufacturer's instructions, the lower limit of detection for each analyte shown in brackets: CXCL8 (0.11 pg/mL), CXCL10 (0.04 pg/mL), CXCL11 (0.14 pg/mL), CCL2 (0.08 pg/mL), CCL4 (0.23 pg/mL), CCL5 (0.59 pg/mL), IL-1β (0.11 pg/mL) and IL-6 (0.10 pg/mL). The remaining analytes were measured using ELISA as per manufacturer's instructions: CXCL9 (1.37 pg/mL, R&D Systems, UK), ECP (0.05 ng/mL, Aviscera Bioscience, Santa Clara, USA), NE (1.98 pg/mL, eBioscience, Hatfield, UK) and α2 macroglobulin (2 ng/mL, Abcam, Cambridge, UK).
Statistical methods
The analyses were performed on the evaluable population. The analysis explored the distributions of the Mean Fluorescence Intensity (MFI) ratios (stimulated/unstimulated and stimulated/inhibited+stimulated cell populations) at each visit. The increase in the MFI ratios was observed for each patient and each visit, and it was noted that the signal to noise ratio was so large that the probability of observing this effect by chance was negligible. The formal evaluation of the statistical significance for the observed deviation of the visit and outcome-dependent mean of MFI ratio from 1 was evaluated by the two-sided t-test.
For all the other analyses, we used a descriptive statistics that characterised demographic characteristics of the study population, variability of the outcome at each of the visits and variability of the pair-wise differences in the outcomes across the visits (ie, within/between patients’ variability). In the analysis of variability the log-transformed (base 10) values were used for MFI, sputum counts and cytokine concentrations while the untransformed outcomes were used for the differential counts (percentages) of neutrophils and macrophages.
A strength of association between repeated measures was characterised by the estimates of the correlation. The visit-depended between patients’ variability was characterised by the estimated SD of the values of (log-transformed in case of MFI, sputum counts and cytokine concentrations) outcomes collected at this visit. The within-patient variability for a pair of visits (eg, visit 1 and visit 2) was characterised by the estimate of the SD of the difference between the values observed at these visits. The numbers of observations at different visits and numbers of matched observations in a pair of visits were slightly different across visits and pairs of visits because of the missing values. Each of the descriptions (ie, correlation, SD (within), SD (between)) produced three values of descriptive statistics. These numbers were summarised by reporting minimum, median and maximum value for each of the outcomes. The values of MFI were summarised similarly.
The tabulations of within and between-patients’ variability are expected to be used in the design of future clinical trials where the effect of treatment will be evaluated by the comparisons of the observations of the outcomes of interest within or across patients.
Results
Pilot study
Flow cytometry was used to measure phosphorylation of STAT1, 3 and 4 proteins in sputum cells following exposure to IFNγ or inhibition of these cell samples with PF-956980. Viable cell populations for flow cytometry could only be obtained using a modified sputum processing technique where a lower concentration of DTT was used as described in the methods section. A comparison of the standard processing technique using 0.1% DTT and the modified approach using 0.05% DTT can be found in the online supplementary figure S1. These early results showed the absence of an assay window between stimulated and non-stimulated neutrophils, whereas phosphorylation of STAT proteins could be measured in the macrophage cell population. The pilot study data failed to demonstrate reliable measurement of phosphorylated STAT 3 or 4 following stimulation, and therefore, only phosphorylated STAT1 was measured in the main study. Finally, the pilot data showed that there was increased variability (data not shown) between replicate samples where the sample contained a low percentge of macrophage cell counts (below 5%). Therefore, sputum selection criteria were introduced for the main study which stipulated that patient samples were excluded from the analysis from those visits where the mean macrophage (%) was <5% of the total leucocyte population.
Supplemental material
Main study
Fifteen patients with COPD were enrolled, and each was asked to complete three visits where they would provide an induced sputum sample. Up to one repeat visit was allowed if the patient was unable to provide an evaluable sample at any of the visits, meaning patients may have a maximum of four attempts to produce an evaluable sample. A patient was included in the study provided that at least two samples met the criteria including adequate flow cytometry measurements. The mean per cent cell viability for evaluable samples used in this study was 88.49%, of squamous cells it was 5.00%, and the mean sputum weight was 1.88 g.
Mean cell counts and SDs for sputum cell counts were largely consistent over the three visits (table 2). Observed variability was lower than previously published literature values.
Repeatability and variability of sputum parameters
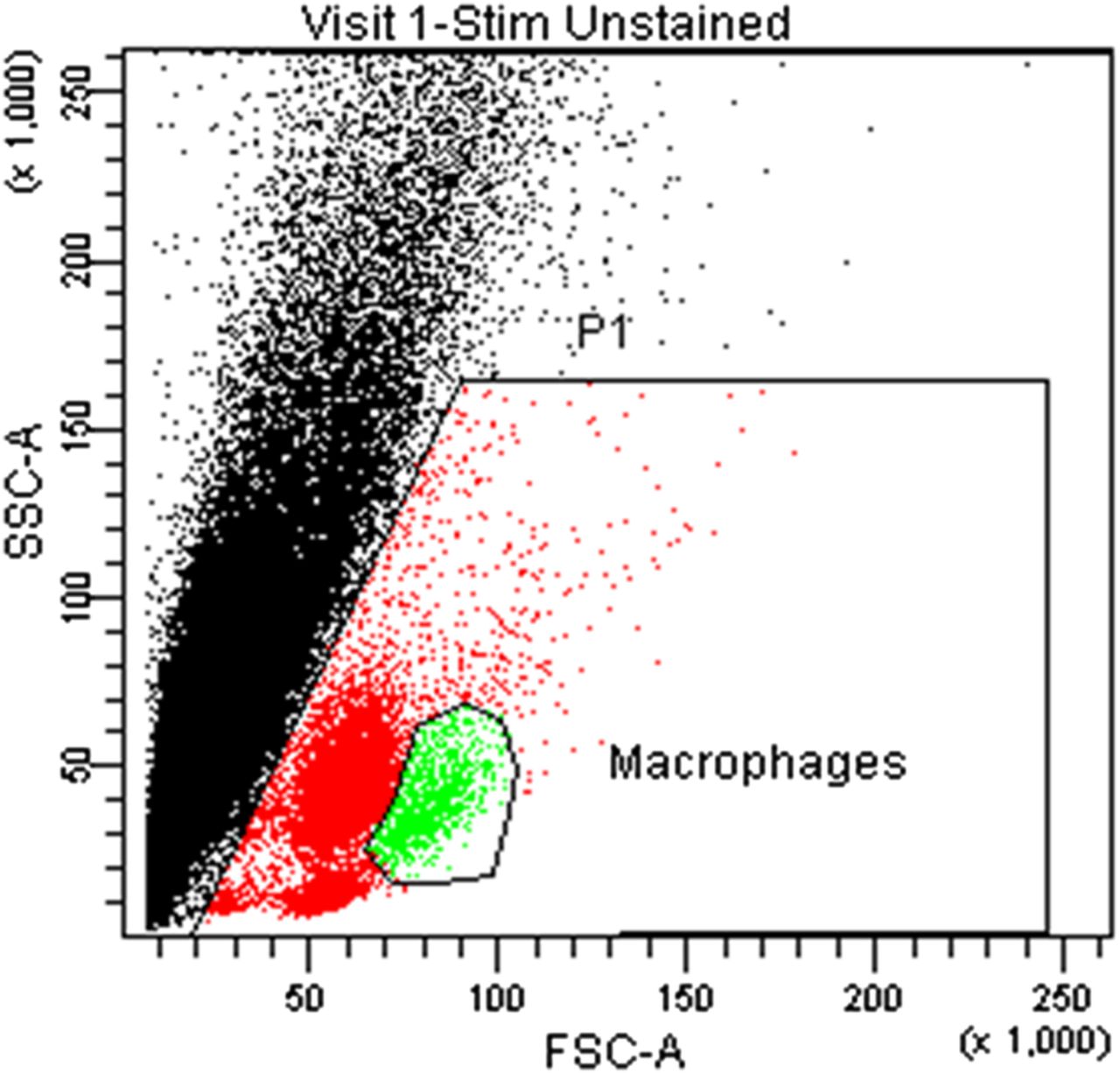
Flow cytometric gating of the macrophage population was achieved via sequential gating to first eliminate debris from the collective leucocyte populations based on size and granularity characteristics (FSC vs SSC) (figure 1). Macrophages were identifiable from the adjacent neutrophil population via their physical characteristics, confirmation of the population orientations being confirmed during prestudy work (data not shown). Debris was gated out (shown as the black population streak at the left-hand side of the profile), and the three distinct populations within P1 gated on with specific interest in the population to the right which contained macrophages. The population to the immediate left of the macrophages represents neutrophils, and the small population at the bottom of the profile is unidentified.

Gating strategy to identify sputum macrophage population. Gate P1 identifies the leucocyte populations in red, macrophages within this gate highlighted in green.
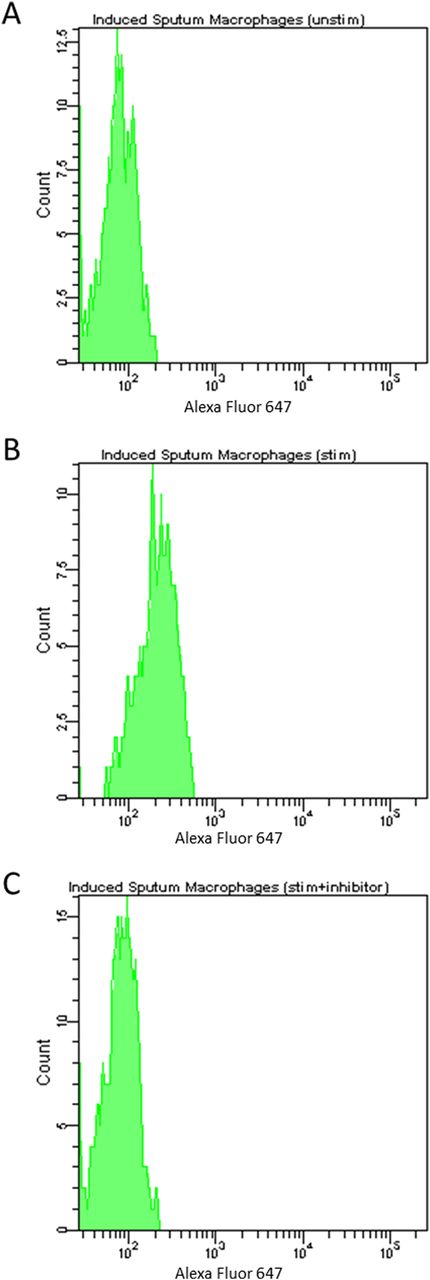
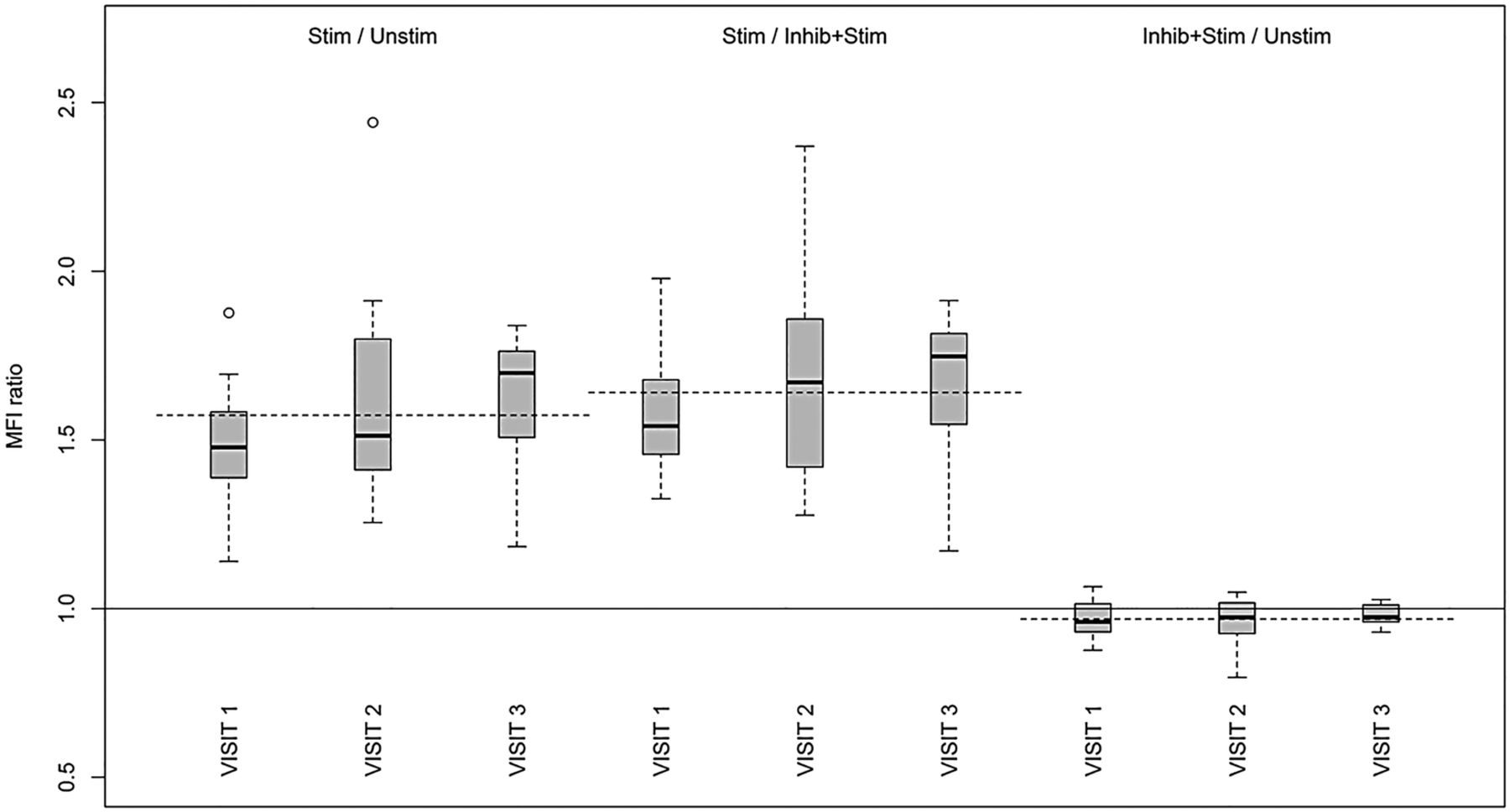
STAT1 phosphorylation as measured by flow cytometric analysis revealed a significant increase following stimulation with IFNγ (p<0.00001) and preincubation with JAK-inhibitor PF-956980 inhibited STAT1 phosphorylation completely with levels detected remaining comparable with non-stimulated samples (MFI ratio stimulated/unstimulated, 1.55; MFI ratio stimulated/inhibited+stimulated, 1.64; MFI ratio inhibited+stimulated/unstimulated, 0.97) (table 3, figures 2 and 3). Levels of STAT1 phosphorylation after stimulation with IFNγ and following preincubation with JAK-inhibitor PF-956980 showed good reproducibility over consecutive visits (table 3), there was little variation across visits in any of the three stimulation conditions, and the stimulated population was different from the non-stimulated and stimulated+inhibitor populations.
Repeatability and variability of mean fluorescence intensity (MFI)

STAT1 phosphorylation in sputum macrophages expressed as flow cytometric histogram data. Mean fluorescence intensity of macrophage population unstimulated (A), stimulated (B) and stimulated after preincubation with JAK-inhibitor PF-956980 (C).
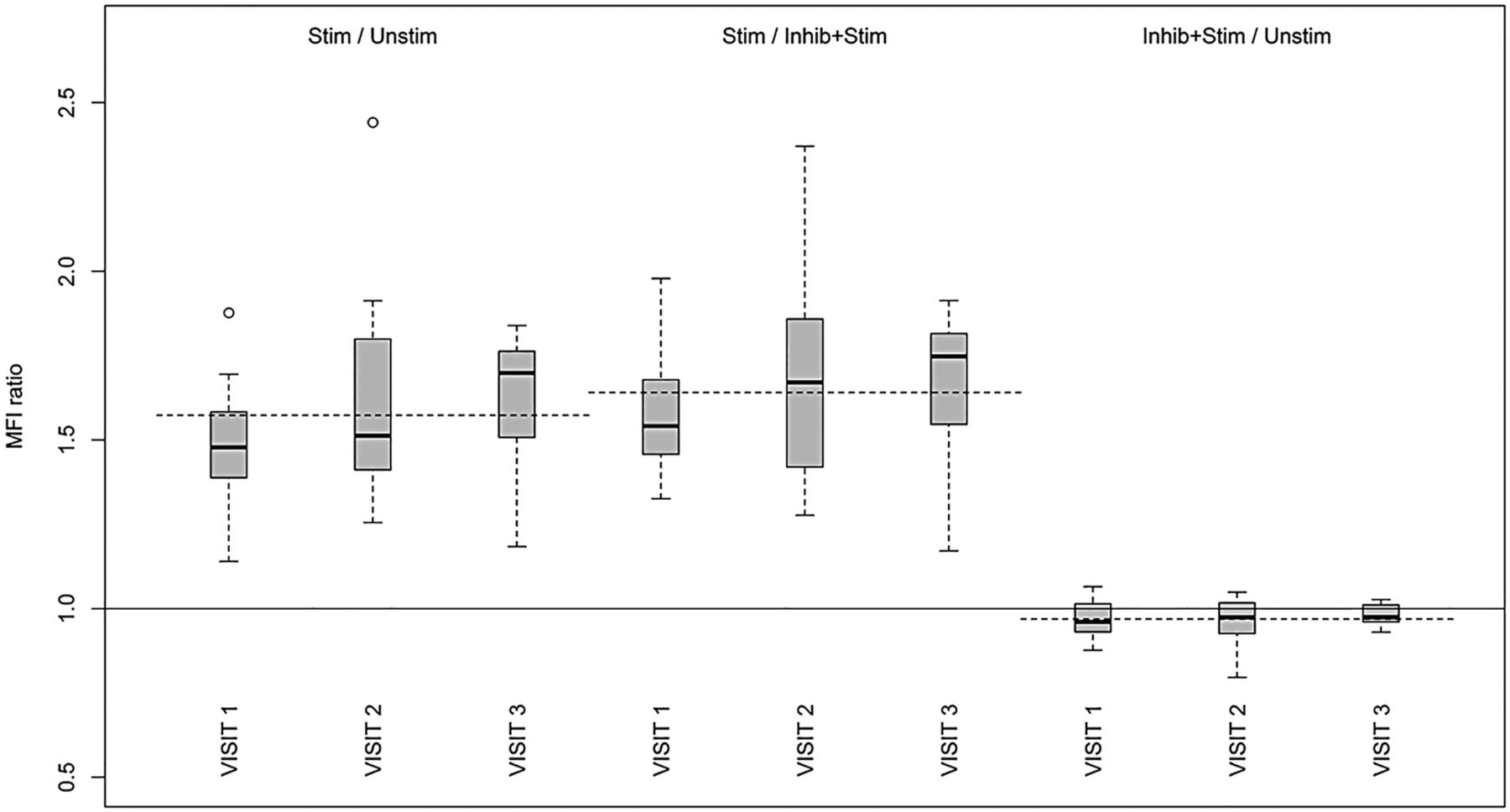
Distributions of ratios of MFI by visit for the stimulated/unstimulated, stimulated/inhibited+stimulated and inhibited+stimulated/unstimulated samples. A median is shown by the black horizontal bar, 25–75% range is contained within a grey-shaded zone. The ends of whiskers show the lowest and highest datum still within 1.5 IQR from the lower and upper quartiles. The unshaded symbols show the values with higher deviations from the quartiles. The dotted lines show the medians of ratios calculated for the data pooled over three visits: (1.57, 1.64, 0.97).
Figure 3 and table 3 demonstrate the sensitivity of the changes in the MFI value to the stimulation and inhibition. The median values and ranges of the ratios of MFI were 1.57 (1.14–2.44) for stimulated/unstimulated ratio, 1.64 (1.17–2.37) for stimulated/inhibited+stimulated ratio and 0.97 (0.80–1.07) for inhibited+stimulated/unstimulated ratio. The visit and outcome dependent tests confirmed the statistical significance of increase in MFI ratios with the p values all below 0.00001.
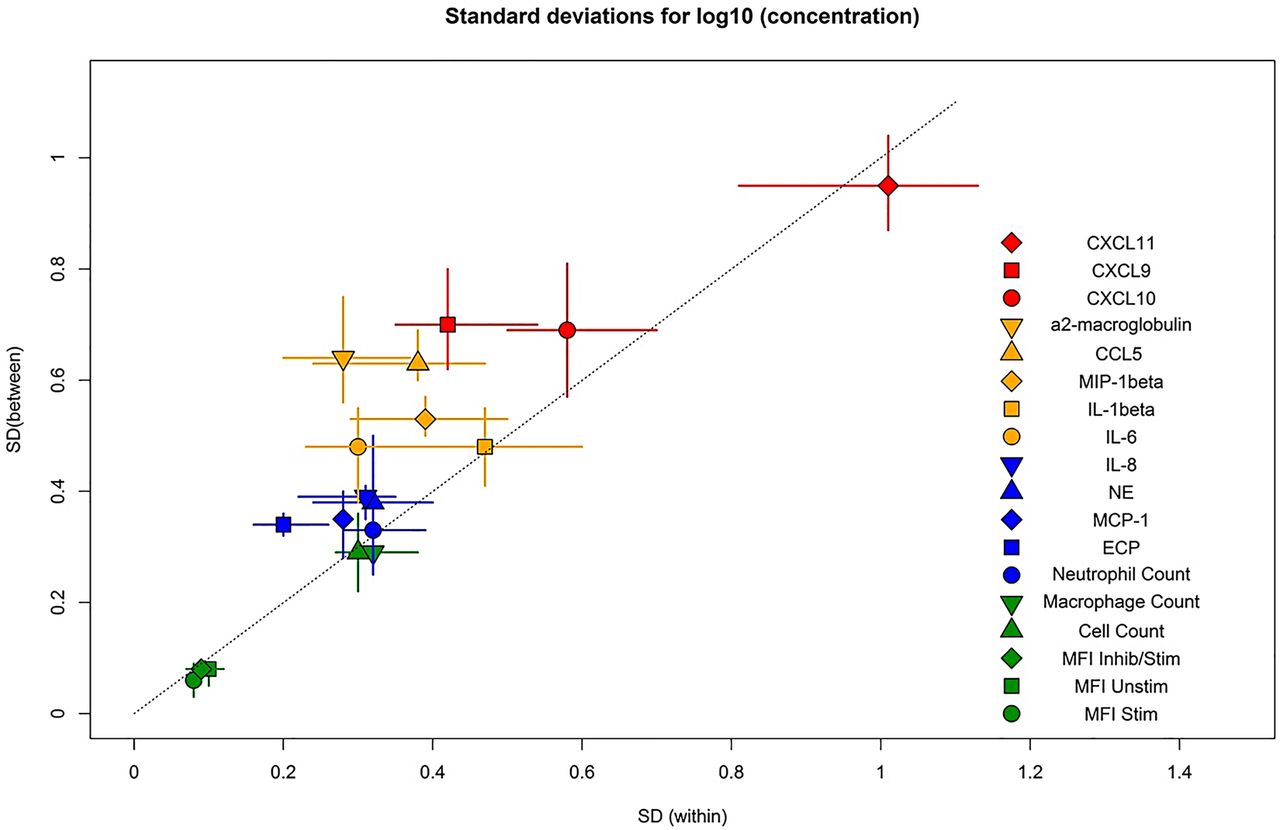
Inflammatory biomarkers were measured and the medians and SDs across the three visits, as well as the within-patient variability estimates exhibited good reproducibility, the within-patient variability was usually somewhat smaller than the between-patients’ variability (table 4).
Repeatability and variability of cytokine measurement in induced sputum supernatant
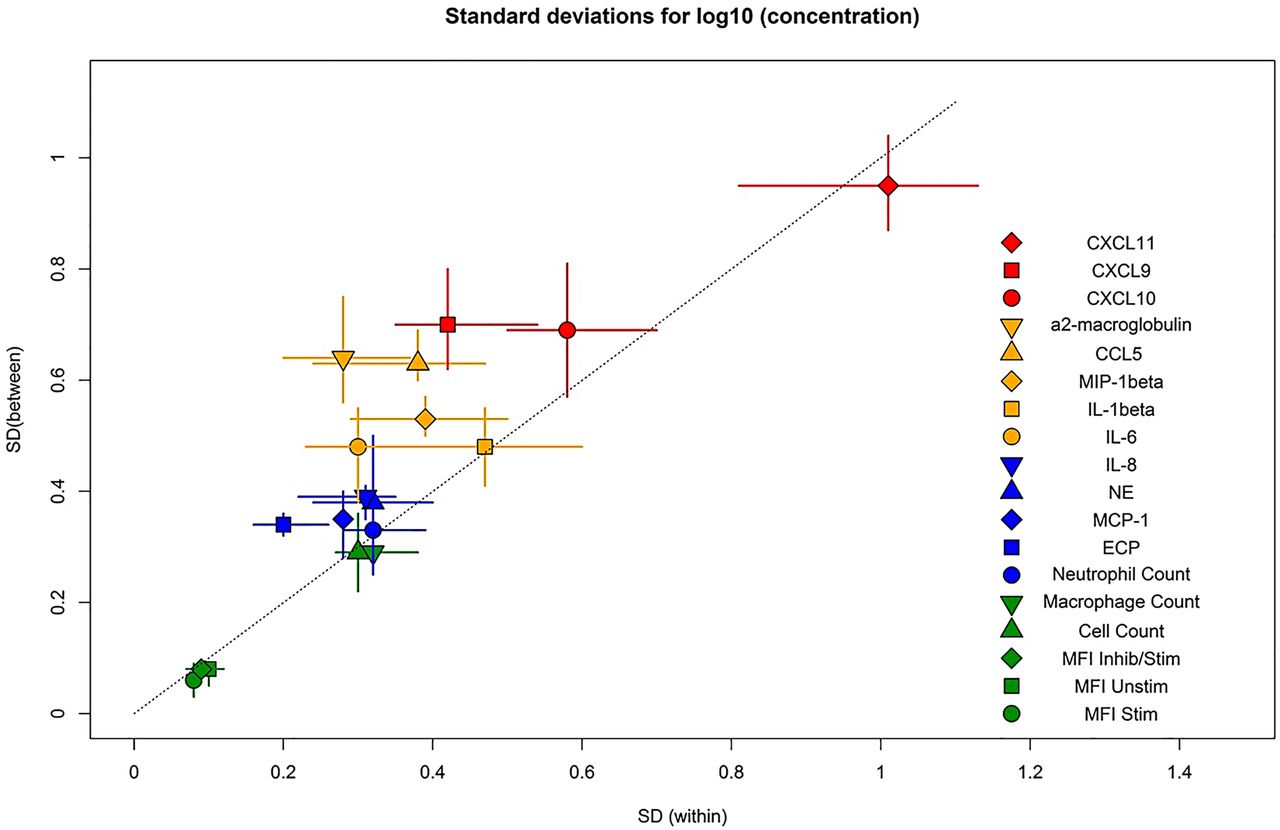
The characteristics of within and between-patients’ variability for all measurements are summarised in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Characteristics of within and between-patients’ variability. Shaded symbols show the median of the three measurements, and the horizontal and vertical lines show the range of the outcome values observed at three visits. A 1:1 line is added to facilitate the comparison of within and between-patients’ variability.
Discussion
COPD is an inflammatory disease of the airways characterised by increased levels of proinflammatory markers in lung tissue, and associated bronchial alveolar lavage (BAL) fluid and sputum. Increased sputum neutrophil levels have been correlated with disease progression and established as a primary biomarker of disease activity. Other biomarkers identified in sputum, such as CXCL8 (IL-8), club cell secretory protein (CC-16) and others, have been associated with disease activity, and in some studies correlate with disease progression.18 ,19
Previous studies have shown that both neutrophil and macrophage cell populations are increased in sputum and BAL samples taken from patients with COPD compared with those from disease-free patients,20 and that this increase is correlated with disease severity.21 ,22 Macrophages, in particular alveolar macrophages, are the most abundant type of immune cell found in the small airways, and they seem to accumulate in areas of tissue damage in the lungs.23 ,24 This increase in the number of macrophages may be due to active recruitment of circulating monocytes as a result of the chemoattractant actions of CCL2 and CXCL1, both of which are found to be raised in sputum and BAL samples from patients with COPD.25
Sputum neutrophil counts have commonly been described as the major biomarker in COPD,26 and neutrophils were previously believed to be an important cell type in kinase pathways. However, the data presented here suggests that macrophages may emerge as the more relevant and important effector cell in lung inflammation in COPD. Macrophages may actually be the key cell of interest in the STAT1 phosphorylation pathway. Indeed where sputum samples comprised of 100% neutrophils were studied no signal change was detected, and it has been previously noted that the correlation of sputum neutrophil counts and lung disease is often weak.26 Measurement of STAT phosphorylation in macrophages using this novel methodology could lead to a greater understanding of the mechanisms driving the chronic inflammation seen in COPD.
As a methodology for the analysis of STAT phosphorylation in COPD, flow cytometric analysis of induced sputum cells has a number of advantages. The use of induced sputum samples rather than whole blood or PBMCs allows the researcher to analyse changes occurring at the site of inflammation, in this case the lung, and therefore, assess the effects of inhaled drugs. Previous work has concentrated on whole blood techniques which provide valuable information relating to systemic effects but lack the specificity of more localised measurements.6 ,7 ,27 Table 3 and figure 3 show that the flow cytometric method produces reproducible STAT1 phosphorylation data over numerous visits enabling assessment of drug effects over time.
Flow cytometric analysis of induced sputum cells samples presents a number of challenges. Some of these are practical, for instance, high levels of epithelial cells and/or debris can affect sample analysis.28 Cell numbers are often limited due to size and quality of sample, meaning a minimum weight and viability count must be established in advance to ensure a sufficient cell count for flow cytometric analysis.24 The use of DTT can alter the detection of cellular surface markers.29 Sputum macrophages tend to express reduced levels of cell surface markers, possibly as a result of higher levels of proteases in the lung environment.30–32 Also, sputum macrophages tend to exhibit increased auto-fluorescence due to endocytosed particles in cigarette smoke leading to possible increases in background signal.33 These issues would seem to suggest that induced sputum is not an ideal sample type to study. However, induced sputum tends to have reasonably high viability compared with spontaneously produced sputum samples,34–36 and the induction procedure is well tolerated by patients with FEV1 >30%, meaning it can be used to study all but the most severe patients with COPD.37 Added to this is the fact that induced sputum appears to give reproducible cell and mediator data making it a good candidate for long term or repeatability studies.38
JAKs are a family of enzymes which catalyse the phosphorylation of STAT proteins, which regulate inflammatory gene expression. Gene association studies have found an association between STAT1 and COPD. On phosphorylation, STAT1 increases transcription and expression of several inflammatory biomarkers, including IFNγ, IL-2 and TNFα.20 ,39 The JAK/STAT pathway can be activated by IFNγ, which is increased in COPD,37 with an increase in STAT1 phosphorylation and upregulation of proinflammatory cytokines, such as CXCL9, CXCL10 and CXCL11 from airway epithelial cells.20 Inhaled JAK inhibitors are being developed with a view to inhibiting this pathway, and thereby reducing inflammation in COPD.
Kinase inhibitors administered via the inhaled route are designed to be delivered direct to the lung in order to avoid systemic effects and adverse effects. For this reason, established whole-blood assays for measuring STAT phosphorylation would not be relevant in these circumstances. Rather, the whole-blood technique is relevant in the evaluation of oral drugs, which have a systemic drug distribution that results in measurable blood levels. An inhaled drug, for lung diseases in particular, has advantages including local delivery to the site of action, and often a reduction in side effects commensurate with reduced systemic exposure.
A methodology such as the one described here would be of great benefit during the development of inhaled compounds. The study design included measuring the levels of one or more cytokines or chemokines in the same sputum sample obtained from the individual. The simultaneous measurement of intracellular STAT phosphorylation and cytokines from the same sample would give a complete pharmacodynamics picture of the compound under analysis, both its effect on STAT activation and the resulting protein translation. Furthermore, the intracellular flow cytometry method allows for identification of specific cell populations expressing phosphorylated STAT. This has not been possible using western blot-based methods.
The clinical development of kinase inhibitors, and particularly kinase inhibitors delivered via the inhaled route, would be enhanced by the development of novel biomarkers that reflect active pharmacologic activity in the lung. These biomarkers can be used to provide the scientific rationale for understanding optimal selection of similar compounds for clinical development, optimal selection of dose, dose range and prediction of likely pharmacodynamic activity. Early selection of the correct dose and dose range in clinical studies allows proof of pharmacology and/or proof of mechanism studies to further define the therapeutic ratio and support the correct dose selection prior to entering into larger patient studies.
The estimates of variability presented in tables 2⇑–4 may be used for power calculations for exploratory studies focused on the effect of the new treatments on the biomarkers of the patients with COPD. These estimates suggest that a small (∼10 patients with COPD with complete responses) proof of pharmacology study using a crossover design will be sufficient for detecting (with the two-sided significance level=0.05 and power=90%), a 30% increase in the MFI caused by STAT1 phosphorylation.
Conclusion
STAT1 phosphorylation and accompanying inflammatory cytokine levels can be reproducibly measured in sputum samples via the novel processing and analysis methods described. The inhibition of STAT1 phosphorylation after IFNγ stimulation by a JAK inhibitor was also demonstrated.
The results of this study indicate that macrophages play an important part in the JAK/STAT pathway of inflammation. Much previous work has focused on neutrophilic inflammation, but these data indicate that, not only are macrophages important, but they play a key role in the regulation of chronic airway inflammation. It is of interest that clinical trials using antineutrophil therapies such as CXCR2 antagonists have shown dramatic reduction in circulating and pulmonary neutrophil counts,40 however, these effects have not translated into meaningful clinical benefits in patients with COPD.41 These techniques can be used to develop a greater understanding of the role of macrophages in chronic airway disease. This information may indicate possible future therapeutic targets while enabling assessment of the efficacy and sensitivity of new and novel therapeutic compounds.
References
Footnotes
GCN and RAH contributed equally.
Contributors GCN, RAH, PJB, IK, LT, BRL, LED were involved in the conception and design of the work. GCN, MS and BRL were involved in the analysis and interpretation of data. GCN, PJB, IK, BRL, and LED were involved in drafting or revising the manuscript. Final approval of the manuscript was by GCN, RAH, PJB, IK, LED, BRL.
Funding Pfizer funded this work.
Competing interests GCN and BRL had support from Pfizer Inc for the submitted work.
Patient consent Obtained.
Ethics approval National Research Ethics Service Committee London, Hampstead, Northwick Park Hospital REC Centre (REC reference 12/LO/0579).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.