Article Text

Abstract
Introduction During critical illness, dental plaque may serve as a reservoir of respiratory pathogens. This study compared the effectiveness of toothbrushing with a small-headed toothbrush or a foam-headed swab in mechanically ventilated patients.
Methods This was a randomised, assessor-blinded, split-mouth trial, performed at a single critical care unit. Adult, orally intubated patients with >20 teeth, where >24 hours of mechanical ventilation was expected were included. Teeth were cleaned 12-hourly using a foam swab or toothbrush (each randomly assigned to one side of the mouth). Cleaning efficacy was based on plaque scores, gingival index and microbial plaque counts.
Results High initial plaque (mean=2.1 (SD 0.45)) and gingival (mean=2.0 (SD 0.54)) scores were recorded for 21 patients. A significant reduction compared with initial plaque index occurred using both toothbrushes (mean change=−1.26, 95% CI −1.57 to −0.95; p<0.001) and foam swabs (mean change=−1.28, 95% CI −1.54 to −1.01; p<0.001). There was significant reduction in gingival index over time using toothbrushes (mean change=−0.92; 95% CI −1.19 to −0.64; p<0.001) and foam swabs (mean change=−0.85; 95% CI −1.10 to −0.61; p<0.001). Differences between cleaning methods were not statistically significant (p=0.12 for change in gingival index; p=0.24 for change in plaque index). There was no significant change in bacterial dental plaque counts between toothbrushing (mean change 3.7×104 colony-forming units (CFUs); minimum to maximum (−2.5×1010 CFUs, 8.7×107 CFUs)) and foam swabs (mean change 9×104 CFUs; minimum to maximum (−3.1×1010 CFUs, 3.0×107 CFUs)).
Conclusions Patients admitted to adult intensive care had poor oral health, which improved after brushing with a toothbrush or foam swab. Both interventions were equally effective at removing plaque and reducing gingival inflammation.
Trial registration number NCT01154257; Pre-results.
- Assisted Ventilation
- Bacterial Infection
- Pneumonia
- Respiratory Infection
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
In general, patients admitted to adult intensive care initially presented with poor oral hygiene.
Oral hygiene intervention during intubation using either a toothbrush or a foam swab significantly improved oral care based on plaque and gingival indices.
There was no significant difference between the oral hygiene interventions based on the measured parameters.
Introduction
There is increasing evidence that oral health impacts on the general well-being of an individual, with cardiovascular disease, diabetes and low birth weight all associated with poor oral hygiene.1–3 Furthermore, poor oral hygiene has been linked with higher incidence of respiratory infections, such as community-acquired pneumonia, healthcare-associated pneumonia, hospital-acquired pneumonia and ventilator-associated pneumonia (VAP).4–6
Dental plaque is an archetypal biofilm and during critical illness can rapidly become colonised by potential respiratory pathogens and in these cases, it serves as a reservoir for VAP pathogens.4 ,7–9 A number of interventions aimed at improving oral cleanliness have demonstrated a reduction in VAP or mortality in randomised clinical trials.10–13 However, these trials did not actually measure oral cleanliness and there has been a paucity of research conducted in mechanically ventilated patients on what represents the optimal methods for improving oral hygiene.14 Indeed the majority of observational studies in the general critical care population demonstrate an increase in plaque scores over time, despite receipt of ‘routine’ oral care.4 ,7–9
It has long been established that the best approach for removal of dental plaque is by mechanical disruption using a toothbrush15 and previously, this approach has been found to be superior than using foam swabs.16 Considerable variability exists in oral hygiene practices among critical care nurses,17 ,18 with use of foam brushes or toothbrushes often employed.18 ,19 The aim of the current study was to compare the efficacy of foam swabs and toothbrushes at removing dental plaque in mechanically ventilated patients. As dental plaque not only acts as a reservoir for respiratory pathogens, but also drives gingival inflammation, the effects of the two interventions on gingival inflammation scores were also assessed.
Methods
Study design: This study employed a ‘split-mouth’ design in which two oral hygiene methods, that is, use of a foam swab or a ‘small-headed’ toothbrush (figure 1) were used to clean the teeth on different sides of a patient's mouth. The advantage of such a split-mouth design over randomising individual patients was the reduction in interparticipant variability.20 The side to which the cleaning method was allocated was assigned by computer-generated randomisation. Assessors, laboratory staff and statistician were blinded to the hygiene method assigned. Trial registration: Clinical Trials.Gov NCT01154257 14 June 2010.

Toothbrush (A) and foam swab (B) used in this study (SAGE products).
Patient recruitment: Ethical approval was obtained from the Research Ethics Committee for Wales (09/MRE09/44). Written informed consent was obtained in accordance with ethical approval. Mechanically ventilated patients admitted to the adult intensive care unit (ICU) at the University Hospital of Wales, Cardiff, UK were eligible for the study. Patients were eligible for inclusion if they were aged >18 years, were mechanically ventilated with an endotracheal tube placed via the oral route, and had >20 teeth of broadly symmetrical (left and right) distribution. Patients that did not meet the inclusion criteria, or had thrombocytopaenia (platelet count <30), uncontrolled coagulopathy, facial or oral trauma, or were expected to be ventilated <24 hours, were excluded from the study.
Oral hygiene intervention: Prior to oral hygiene intervention, Silness-Löe plaque (table 1) and gingival indices (table 2) were documented, where scores ranged between 0 and 3, with 0 being equal to health and a score of 3 meaning gross plaque deposits or marked gingival inflammation.21 These were recorded on the upper and lower first molars, first bicuspid and central incisors on each side of the mouth from the buccal surface. Plaque and gingival index scores were an average of the six teeth on each side. For patients with missing index teeth, the remaining teeth in closest proximity were scored. A decayed, missing and filled teeth (DMFT) index22 was used as an indicator of the patient's oral health on admission to critical care.
Plaque index scoring used in this study and as defined by Silness and Löe21
Gingival index assessment (severity of gingivitis) used in this study based on gingival colour, presence of oedema and bleeding21
Following receipt of training by a dental professional, research and nursing staff provided oral hygiene intervention. Cleaning was performed every 12 hours until extubation (if <7 days) or up to 7 days after recruitment. The modified Bass technique23 for brushing was used with toothbrushes and foam swabs that had been premoistened with sterile water. Chlorhexidine was not used in the study, as it would reduce bacterial numbers, prevent plaque reaccumulation on clean oral surfaces24 ,25 and was not part of the routine oral care in the critical care unit. Each side of the mouth was cleaned for 1 min (30 s per quadrant) and compliance with the intervention recorded. Silness-Löe plaque and gingival indices were recorded daily and on each side of the mouth by a single, dentally trained operator blinded to treatment allocation. These scores were recorded at the start of the study (ie, baseline), before randomisation and then each morning.
Dental plaque was collected using sterile endodontic paper points (size ISO45; QEP, Peterborough, UK), with one paper point used per tooth from each side of the mouth to determine bacterial load. Plaque samples were obtained at the same time of day, and by the same individual who measured the plaque and gingival indices prior to cleaning. Sampling started at the distal part of the buccal aspect of the tooth with 1 mm of the paper point placed into the gingival sulcus. Using a slow and continuous motion, the paper point was drawn towards the operator to recover the plaque. Paper points were immediately immersed in 1 mL of reduced transport fluid for microbial culture.26 Paper points were vortex mixed for 20 s and the resulting solution serial decimally diluted in phosphate buffered saline. Fifty-microlitre volumes of the dilutions were then inoculated on selective agar media (Lab M, Heywood, UK) using a spiral plating system (Don Whitley Scientific, Shipley, UK). The following agars were used to culture microorganisms: blood agar for total bacterial enumeration, fastidious anaerobe agar (FAA) for anaerobic/facultative anaerobic bacteria, Sabouraud dextrose agar and CHROMagar Candida (CHROMagar; Paris, France) for Candida and yeast species, mannitol salt agar (MSA) for Staphylococcus species, and a selective agar for Pseudomonas aeruginosa (Lab M). Inoculated media were incubated under appropriate gaseous environments at 37°C for 48 hours, with the exception of MSA (5 days) and FAA (7 days). After incubation, colony-forming units (CFUs) were enumerated and suspected target species presumptively identified based on colony appearance. Definitive identification was through PCR-mediated 16S ribosomal DNA (rDNA) sequencing. Bacterial DNA was extracted using the Gentra Puregene Yeast/Bacteria kit (Qiagen, Manchester, UK). rDNA was amplified by PCR using the universal bacterial primer pair of D88: GAGAGTTTGATYMTGGCTCAG, and E94: GAAGGAGGTGWTCCARCCGCA.27 Final reaction volumes were 50 μL and included 1 μL of each forward and reverse primer at 50 mM, 25 μL of PCR MasterMix (Promega, Southampton, UK) and DNA template (5 μL). PCR cycling consisted of initial heating at 95°C for 5 min, followed by 30 cycles of 95°C for 45 s denaturation, primer annealing at 60°C for 60 s and product extension at 72°C for 1 min. The extension step was extended by 5 s per cycle and a final extension step of 72°C for 5 min was performed. Negative controls of sterile DNA-free water in place of template DNA were included for each PCR. Amplicons (1500 bp) were resolved by standard electrophoresis in 1.5% (w/v) agarose gels stained with Safeview (NBS biologicals, Huntingdon, UK) and visualised under ultraviolet light using a GelDoc system (Bio-Rad). Five μL of each PCR product was cleaned by addition of 2 µL of ExoSAP-IT (USB/Affimatrix, High Wycombe, UK) and heating for 15 min at 37°C, followed by a further 15 min at 80°C. Cleaned products were diluted to 20 μg/μL in DNAse-free water and sequenced using the d88 forward primer in an automated sequencer (ABI 3130xl genetic analyser; Applied Bioscience, Warrington, UK). Species were identified from sequences using the Basic Alignment Search Tool (BLAST) from the National Centre for Biotechnology Information (NCBI) for microbes, and≥95% identity was considered confirmatory of species identification.
Statistical analysis
No previous studies had been conducted in mechanically ventilated patients that could prior inform on sample size. It was estimated that 20 patients would be required to detect a 0.63 shift in plaque scores with a power of 80% at the conventional 0.05 α level. Initially it was intended to analyse plaque scores after 72 hours of cleaning and it was estimated that recruiting 50 patients would give at least 20 patients allowing for drop out of patients through endotracheal tube (ETT) extubation or death before 72 hours. However, as it was deemed that 24 hours of cleaning would be sufficient to reduce plaque scores, it was decided, prior to patient recruitment to analyse data after a minimum of 24 hours.
The distribution of numeric data was tested for normality and presented as mean (SD) for normally distributed data, and median (range) for non-normally distributed data. The overall changes (baseline to end of follow-up) in plaque index, gingival index and bacterial counts were calculated for each patient and cleaning method. The null hypothesis of no change in outcomes over time was tested using a paired samples t-test for normally distributed differences, or a Wilcoxon signed-rank test for skewed distributions. McNemar's test was used for paired proportions.
For normally distributed differences, repeated measures analysis of variance was used to test significant differences in outcomes between methods within patients after adjusting for baseline DMFT, number of days follow-up and side of the mouth. A 5% level of significance was used for all statistical tests. The statistical software package IBM SPSS for Windows V.21 was used for analysis.
Results
Informed consent was obtained for 28 patients by a patient consultee. After inspection by the dental professional, six consented patients were not eligible for the study as they had insufficient or asymmetric teeth and one further patient died within 24 hours, leaving 21 patients to complete investigations. Following a safety alert from the UK medicines and healthcare products regulatory agency28 (not arising from this study), foam swabs were withdrawn from clinical use in Wales (but not elsewhere in the UK) and no further recruitment was allowed. The 21 patients comprised of 10 males and 11 females, aged between 23 and 70 years (mean age 49 years). Recorded patient characteristics were diagnosis on admission, duration of hospitalisation, days of intubation prior to randomisation and recent antibiotic therapy (table 3). On average, days of hospitalisation prior to admission in intensive care were 3.4 (4.5 SD), and ventilator days prior to randomisation was an average 3.4 (3.2 SD) days. The majority of patients (16/21) were in receipt of antibiotic therapy at the start of the study. The median number of follow-up days was 4 days (range 2–7 days) and mean DMFT score was 10.7 (SD 5.2, range 3–23). Compliance with the oral interventions was 100% and there were no reports of harm or unintended effects for any of the participants.
Characteristics of the patients participating in this study
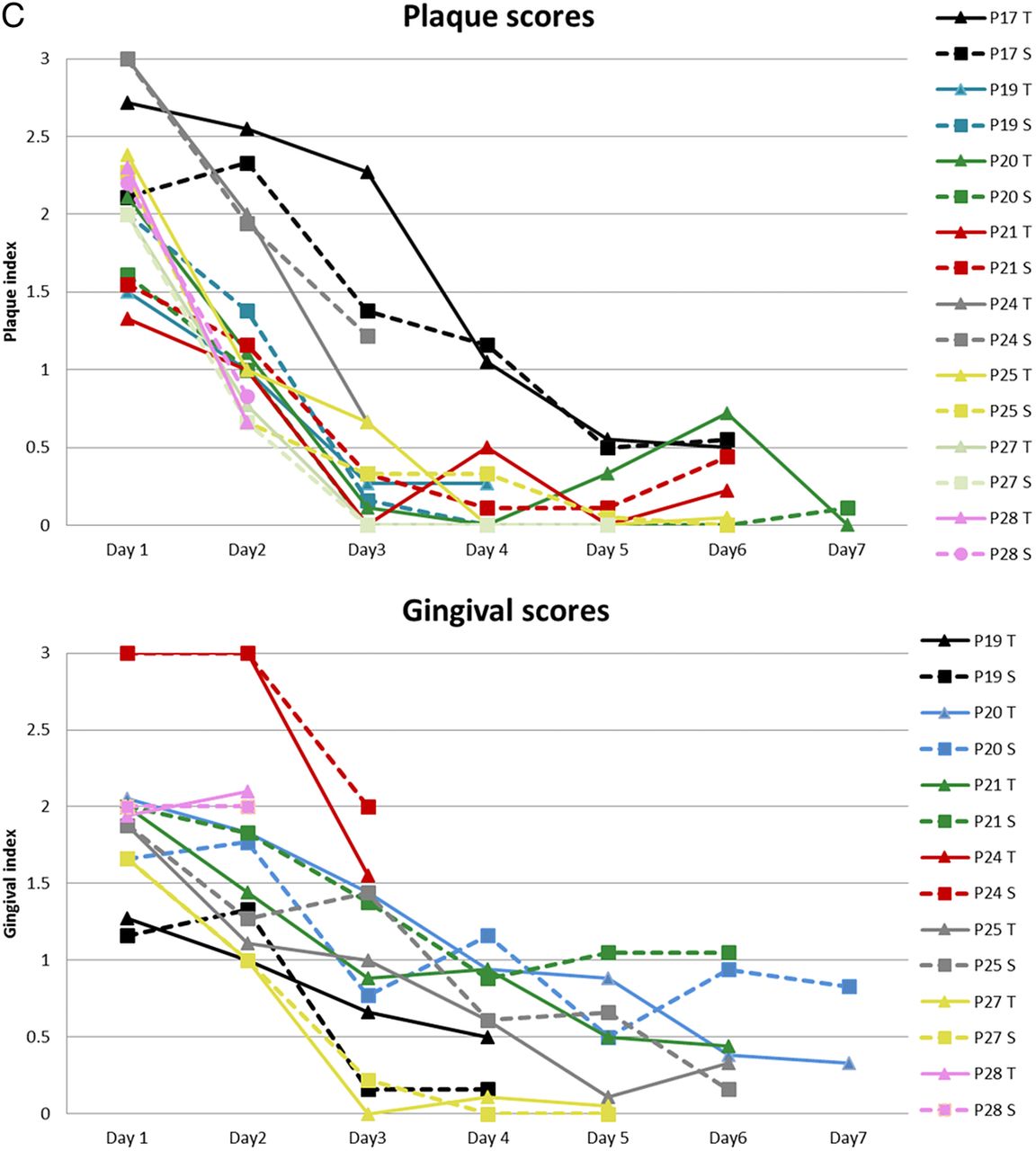
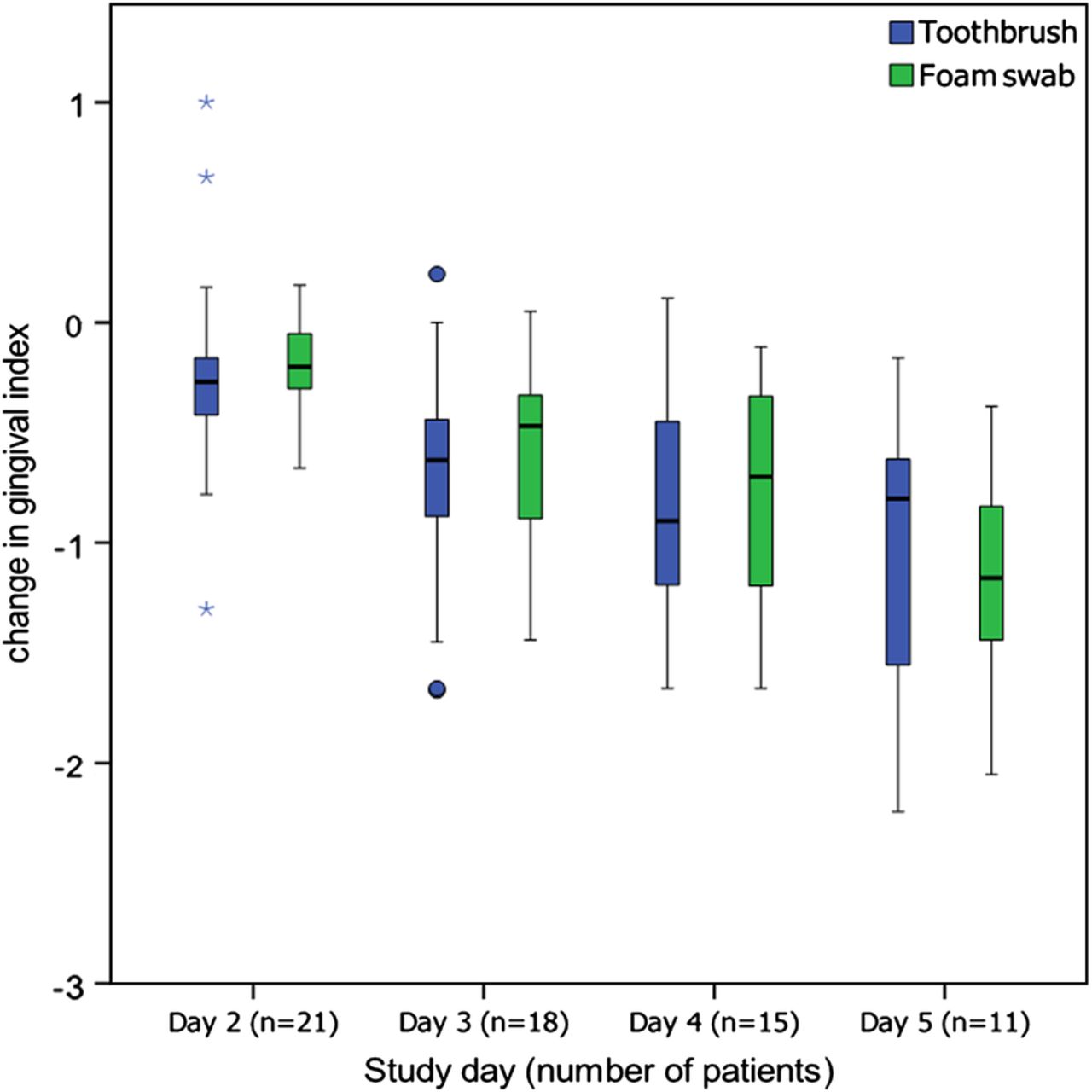
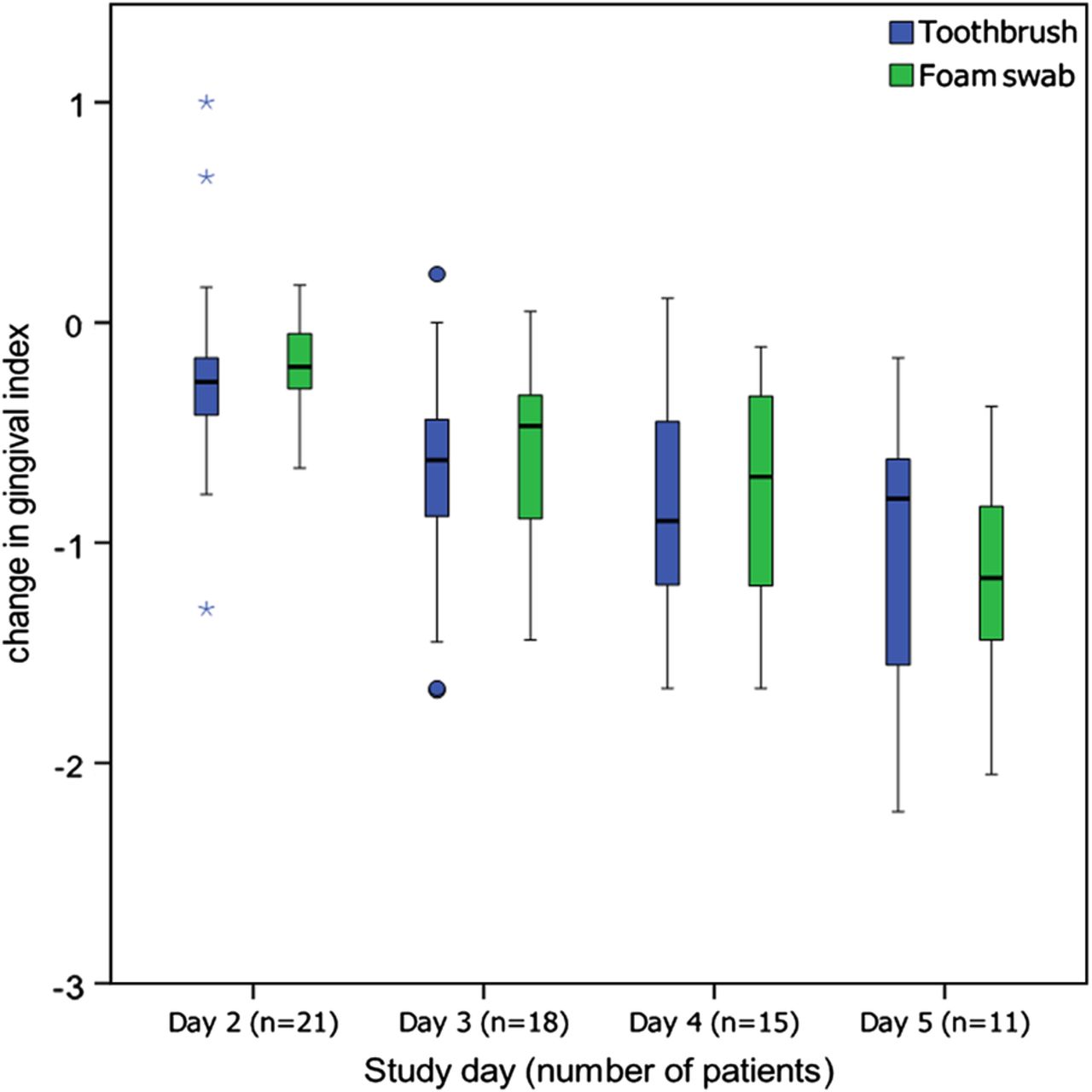
Baseline scores and the changes in each outcome over time for plaque index, gingival index and bacterial counts for each treatment are presented in table 4 and figure 2A–C. There was a significant reduction in plaque index over time for use of toothbrushes (mean change=−1.26; 95% CI −1.57 to −0.95; p<0.001) and foam swabs (mean change=−1.28; 95% CI −1.54 to −1.01; p<0.001). There was also a significant reduction in gingival index over time using toothbrushes (mean change=−0.92; 95% CI −1.19 to −0.64; p<0.001) and foam swabs (mean change=−0.85; 95% CI −1.10 to −0.61; p<0.001). There was no significant difference in reduction of plaque index between the two interventions (p=0.24). Greater reduction in gingival index was observed for toothbrushes compared with foam swabs (figure 3), although this was not statistically significant (p=0.12). The number of days of cleaning was a significant covariate in the analysis of change in gingival index (p=0.003) and plaque index (p=0.05). There was some evidence of an interaction between treatment and baseline DMFT score for both change in gingival index (p=0.07) and plaque index (p=0.06), suggesting that the impact of toothbrushes and foam swabs may be greatest in those with poorest oral health.
Baseline scores and change in outcomes (plaque index, gingival index and bacterial counts) by oral hygiene method (n=21 patients)

(A) Changes in plaque and gingival index (Silness and Löe)21 for patients 1–8 over a 7-day period using oral hygiene intervention either with a toothbrush (solid line) or foam swab (broken line). (B) Changes in plaque and gingival index (Silness and Löe)21 for patients 9–17, over a 7-day period using oral hygiene intervention either with a toothbrush (solid line) or foam swab (broken line). (C) Changes in plaque and gingival index (Silness and Löe)21 for patients 19–28, over a 7-day period using oral hygiene intervention either with a toothbrush (solid line) or foam swab (broken line).
Continued
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box plots of change in gingival index (from baseline) for each study day. Asterisks represent extreme outliers >3 IQR; circles represent outliers >1.5 IQR.
An overall analysis of patients’ oral health status was compared with results from the 2009 Adult Oral Health survey29 undertaken by the National Health Service (NHS) Information Centre for health and social care (table 4). From this comparison, it was apparent that the patient cohort examined in this study had a similar number of teeth present and less obvious caries than the general population. However, periodontal health was worse, impacting on overall oral health (table 5). The 2009 survey reported that 10% of the population had excellent oral health, but if similar parameters of excellence were applied to the participants in this current study, only one patient (4%) met these criteria. For patients that were not randomised on the same day of hospital admission, it was possible that their periodontal health had progressively deteriorated due to their illness impairing normal oral hygiene routine and reliance on healthcare workers to perform oral hygiene tasks.
Comparison of oral health parameters of this study's patients and the general population
No significant change in bacterial counts was observed over time using either toothbrushes or foam swabs (table 4). Ten of the 21 patients had high baseline total bacterial counts (≥106 CFUs/sample). Of these, 7 (70%) exhibited a reduction in bacterial counts using toothbrushes compared with 4 (40%) using foam swabs (p=0.48).
From microbial culture, respiratory pathogens were identified in the dental plaque of patients, with Staphylococcus aureus detected in 6 patients and P. aeruginosa in 2 patients, 5 patients had S. aureus or P. aeruginosa colonisation from day 1, while 13 patients did not have cultivable respiratory pathogens. Interestingly, for two patients, S. aureus was not recovered from dental plaque until day 3 of the study, and for 1 patient, P. aeruginosa was present only from day 4. The opportunistic fungal pathogen, Candida albicans was cultured from the plaque of 16 patients.
Discussion
In healthy adults, the predominant oral microorganisms are normally harmless bacteria, with the plaque community largely consisting of facultative anaerobic Gram-positive streptococci. However, in critically ill adults, a rapid shift to inclusion of potentially pathogenic organisms including S. aureus and Gram-negative bacilli such as P. aeruginosa can occur; both of these species can cause VAP.4 ,7–9 Molecular analyses of bacteria from the oral cavity and those isolated from the lungs of patients with VAP have demonstrated that genetically identical organisms were present at both sites, supporting the concept that bacteria colonising the oral cavity were also involved in pulmonary infection.30–33 In keeping with this aetiology, a number of interventions that improve oral cleanliness have been shown to reduce either VAP34–36 or mortality.13 These interventions have tended to focus on use of antiseptic or antibiotic strategies, often involving chlorhexidine, rather than methods routinely employed in dentistry. The reason for this may be the greater familiarity of critical care healthcare professionals with pharmacological interventions.
A rapid improvement in oral hygiene can be achieved by restarting toothbrushing and in this regard, twice daily brushing of teeth is recommended to remove plaque and prevent plaque-mediated diseases such as dental caries and gingivitis.37 ,38 However, there is considerable variability among critical care nurses on how oral care is delivered, with many choosing a foam swab in preference to a toothbrush, or neither method being used and relying on the application of antiseptic solutions or gels.18 ,39 ,40 Almost all studies in critically ill patients have demonstrated that plaque scores increase even when oral care programmes are in place4 ,7–9 and it is therefore important to determine the optimal approaches to reduce plaque scores in mechanically ventilated patients.14
In the current study, we determined the effects of foam swabs and toothbrushes on indices of oral cleanliness. A split-mouth design commonly used in oral care research was employed, as this reduces interindividual variability. Our results demonstrated that both plaque and gingival scores improved with the two tested interventions, and there was no significant difference between use of foam swabs and toothbrushes in their ability to improve oral cleanliness. This is in contrast to studies in volunteers where mechanical disruption of plaque was found to be far more effective using a toothbrush.16 ,41 ,42 It is unclear why no significant difference was observed, but the foam swab used in this study had a coarse ridging (figure 1), which may have assisted plaque removal. A limitation to this study was the relatively short follow-up period (2–7 days); however, it would be expected that the changes in the level of dental plaque accumulation would be most noticeable in the first 48 hours and it was possible that the improvement reached a plateau where no further significant benefit could be achieved. Nevertheless, low levels of dental plaque would be expected when a strict protocol was followed. A similar dynamic was expected with gingival inflammation scores, although the initial response could take longer, to allow tissues to respond to the new conditions. Only one other study has compared use of a toothbrush with foam swabs during critical illness and measured plaque scores.43 Needleman et al compared a powered toothbrush with a foam swab in 46 individually randomised patients, with cleaning undertaken four times a day for 2 min in combination with 20 mL of 0.2% chlorhexidine. The study found that a powered toothbrush was significantly better at reducing plaque.43 However, it was also observed that foam swabs reduced plaque scores significantly from baseline. Powered toothbrushes have the advantage of a much smaller head than a manual brush and direct visualisation is not necessary, as the rotating head has only to be held on the tooth surface. In mechanically ventilated patients, a powered toothbrush may have an advantage over a manual toothbrush for these reasons and should be evaluated in future studies.
No reduction in the number of bacteria isolated from plaque was evident by either method. This might reflect difficulties in plaque collection or could be due to the fact that plaque quantity was not simply a reflection of bacterial number, as most of the plaque substance consists of extracellular polymeric substances (EPS). For example, there could be cases where plaque indices differ not as a result of changes in bacterial number, but due to the relative quantity of EPS. This result is in contrast to the study of Needleman et al43 where chlorhexidine in combination with a toothbrush or foam swab led to significant reductions in the number of plaque bacteria recovered.
Candida colonisation of the respiratory tract has been previously reported for 25% of critically ill patients receiving mechanical ventilation,44 and in the present study, the yeast was present in the dental plaque of 76% of patients. Candida colonisation of the airways has been identified as an independent risk factor for P. aeruginosa VAP44–46 and may therefore represent a possible target for reducing VAP. While culture analysis showed that S. aureus and P. aeruginosa were present in the plaque of only 13 patients, it should be highlighted that this was a short duration study, and more sensitive molecular methods may have revealed a higher incidence of these bacteria in plaque specimens. Furthermore, this study was limited to two major VAP pathogens, but additional respiratory pathogens could have been identified using a wider range of selective culture media.
It is important to emphasise that this study has focused on the efficacy of two oral hygiene practices, rather than their effect on VAP incidence, ICU length of stay or mortality rates. Toothbrushing has been used in a number of critical care studies as a method to reduce VAP, with mixed findings.47–50 Two recent systematic reviews and meta-analysis concluded that there was no robust data supporting a reduction in VAP and that more research was necessary.51 ,52 Unfortunately, within these studies, compliance with the intervention was variable53 and none of the studies reported if there was a reduction in dental plaque, which serves as the reservoir for respiratory pathogens. Our results demonstrated that both foam swabs and toothbrushes were able to reduce plaque scores in mechanically ventilated patients and were not significantly different in this regard. However, considerably more research is required to define the optimal method for mechanically removing plaque; a powered toothbrush, a manual brush with a smaller head or increased frequency of cleaning may prove more effective and a larger sample size will make findings more robust.14 Moreover, a better understanding of how antiseptics or antibiotics interact with mechanical methods is required. In a recent meta-analysis, Klompas et al54 suggested that chlorhexidine could be ineffective or possibly harmful in general critical care units. Chlorhexidine is less effective in vitro than other antiseptics, but in vivo it binds to clean tooth surfaces and is released over time, a property called substantivity, and this reduces plaque accumulation.55 ,56 Mature biofilms are also less susceptible than those recently formed57 and it follows that chlorhexidine will be most effective when plaque has been physically disrupted.43 ,58
Conclusion
Oral health of patients admitted to this adult ICU was generally poor. Dental plaque and gingival inflammation indices were reduced when toothbrushes and foam swabs were used in a strict oral care programme. While more research is needed to demonstrate the effect of mechanical plaque removal in the prevention of colonisation by respiratory pathogens and VAP incidence, oral care in ICUs must not be neglected.
Acknowledgments
The authors would like to thank the patients and their families who took part in this study and the nursing and research staff in the adult critical care unit at the University Hospital of Wales.
References
Footnotes
MPW and DWW are joint last authors.
Contributors PJM, AH, SH, JMC, NP, CE, TK, MAOL, MPW, DWW provided substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data. PJM, AH, MPW, DWW were involved in drafting the work or revising it critically for important intellectual content. MPW, DWW were involved in final approval of the version published. MPW, DWW provided agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding MPW was funded by a NISCHR AHSC Clinical Research Fellowship. MPW consulted for Bard, Merck (MSD), KaloBios Pharmaceuticals (Advisory Boards); has previously been employed by NISCHR AHSC (research fellowship 0.4 WTE); has received royalties from Wiley Publishing (book chapters); has received a fee for lecturing at an educational meeting from Fisher & Paykel, Merck (MSD); has received support for travel from ISICEM, Eli Lilly, British Thoracic Society, and Intensive Care Society; has received a loan of EIT equipment for research from CareFusion.
Competing interests This research was funded by Cardiff University and PJM was supported by a Walport Clinical Fellowship and obtained a research grant for consumables from a GSK-Oral and Dental Research Trust award. SAGE products gifted the toothbrushes and foam brushes used in this study.
Ethics approval Research Ethics Committee for Wales.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.