Article Text

Abstract
Introduction There is a lack of data evaluating the clinical effect on symptoms of pleural intervention procedures. This has led to the development of patient-reported outcome measures (PROMs) to define what constitutes patient benefit. The primary aim of this paper was to prospectively assess the effect of pleural procedures on PROMs and investigate the relationship between symptom change and clinical factors.
Methods We prospectively collected data as part of routine clinical care from 158 patients with pleural effusion requiring interventions. Specific questionnaires included two patient-reported scores (a seven-point Likert scale and a 100 mm visual analogue scale (VAS) to assess symptoms).
Results Excluding diagnostic aspiration, the majority of patients (108/126, 85.7%) experienced symptomatic benefit from fluid drainage (mean VAS improvement 42.6 mm, SD 24.7, 95% CI 37.9 to 47.3). There was a correlation between symptomatic benefit and volume of fluid removed post aspiration. A negative association was identified between the number of septations seen on ultrasound and improvement in dyspnoea VAS score in patients treated with intercostal chest drain.
Conclusion The results of our study highlight the effect of pleural interventions from a patient’s perspective. The outcomes defined have the potential to form the basis of a clinical useful tool to appraise the effect, compare the efficiency and identify the importance of pleural interventions to the patients.
- Pleural Disease
- mesothelioma
- empyema
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
key messages
This is the first study assessing the effect of pleural procedures on patient-reported outcome measures.
Septation score is a potential novel predictor of symptomatic response from fluid drainage.
Patient reported outcome measures have a potential to be employed in everyday clinical practice and may form a basis of a clinical useful tool in the future.
Introduction
Pleural diseases are frequent health problems in the general population, and under this term, a broad variety of different conditions are included that require specific management.1 2 Pleural effusion and pneumothorax are the most common presentations of pleural disease and are increasing in incidence.3–6 Standardisation of management of pleural diseases is difficult, and the number of pleural interventions available to physicians is rapidly expanding.7 Pleural aspiration, chest drain and indwelling pleural catheter (IPC) insertion, medical thoracoscopy and ultrasound (US)-guided pleural biopsies are included within the armamentarium of available procedures.7 Clinicians providing these interventions must be able to select the optimal intervention rationally, based on patient benefit.
Dyspnoea is one of the most common symptoms of pleural diseases and the main reason patients present to medical services. Relief of dyspnoea is the most important outcome from a patient’s perspective and is the treatment intent in the majority of cases. Symptomatic benefit has not been traditionally used until recently as a primary endpoint in clinical studies of pleural interventions, with radiological or biological measurements preferred potentially due to lack of data on the valid measurement and meaning of symptom change.8
Patient-reported outcome measures (PROMs) indicate a patient’s health status or health-related quality of life at a single point in time and are gathered through short, self-completed questionnaires. They offer the opportunity to improve the quality and outcomes of health services, reflecting patients’ experiences and views.9 10 Recently, clinical trials have started to develop and employ PROMs for the appraisal of novel treatments in malignant pleural effusion (MPE).11 A visual analogue score (VAS) for assessing dyspnoea has been used for patients with MPE and the percentage of patients that experienced symptomatic benefit after each intervention has been evaluated.12 A number of different symptom-based outcome measures have been used in patients with MPE in the literature13–16 but none has specifically addressed pain and breathlessness in a clinically pragmatic population undergoing pleural procedures.
The impact of different pleural interventions on patient symptoms has never been measured in real-life practice. The primary aim of this paper was to prospectively assess the effect of various pleural procedures on PROMs and investigate the relationship between symptom change and clinical factors.
Methods
Participants
Patients were prospectively recruited as part of routine clinical care, with consecutive patients seen in our service between 1 November 2013 and 1 June 2015. Patients who had pleural effusion requiring intervention such as diagnostic or therapeutic aspiration, intercostal chest drain (ICD) insertion, IPC insertion and medical thoracoscopy were included.
PROMs based on VAS and a seven-point Likert score
We assessed each patient-reported dyspnoea using two separate scores. A 100 mm VAS, anchored at 0 mm (‘not breathless at all’) and 100 mm (‘worst possible breathlessness’). The VAS for dyspnoea was taken pre and post each procedure. VAS scores for pain, willingness to repeat the procedure if clinically indicated and patients’ expectations of the procedure were taken in parallel.
Patients completed a seven-point Likert scale for dyspnoea post procedure that enables the identification of the significance of improvement. Patients scaled the effect of the procedure on their breathing on six different points. Patients who reported improvement on the Likert scale post procedure (‘slightly or large’) were defined as having experienced clinical benefit from the procedure.
Questionnaire/data acquisition
Data were acquired using a paper survey in a single centre (Oxford University Hospitals NHS Foundation Trust). Alongside with information for dyspnoea, VAS scores for pain, willingness to repeat the procedure if clinically indicated and patients’ expectations of the procedure were taken in parallel (see online supplementary material). Clinical, radiological and diagnostic data were recorded as part of routine clinical care and patients categorised according to underlying diagnosis. Patients completed the questionnaire within 1 hour post aspiration or IPC insertion and within 24 hours post thoracoscopy and ICD insertion (as the drainage time was intended clinically to be different). Information on PROMs, baseline data, thoracic US parameters and the volume of fluid drained in 24 hours were also recorded.
Pleural procedures
Interventions for pleural effusion occurred with US guidance in all cases. During US, size of effusion, fluid echogenicity, maximum depth of fluid and the number of fluid septations were assessed (scored as no septations, 1–2, 3–4 and >5 septations visible in a single US field at area of maximum septations). Local anaesthetic (1% lidocaine—up to 30 mL) was used for all procedures. Lidocaine plus epinephrine and slight sedation was used in addition for IPC insertion and medical thoracoscopy. Patients with trapped lung (defined as inability of the visceral and parietal pleura to oppose) post-therapeutic aspiration or ICD or IPC insertion were also recorded.
Statistics
All analyses were preplanned prior to review of any data. GraphPad Prism software V.6.0 (GraphPad Software, California, USA) and SPSS V.22.0 were used. Patients were categorised based on disease, type of pleural intervention and response to the Likert scale. Data were assessed for distribution and are presented as mean, SD, 95% CI. The mean decrease in VAS following each procedure was calculated for each group, with 95% CIs. Normally distributed data were compared with t-test for two groups (unpaired to compare ΔVAS means and paired for comparison pre and post procedure) and analysis of variances for multiple groups (Holm-Sidak’s multiple comparisons for ΔVAS dyspnoea post procedure—figure 1) were used for analysis of the data. For non-parametric data (VAS for pain—figure 2; and ΔVAS based on number of septations—figure 4) Kruskal-Wallis with Dunn’s multiple comparisons were used and data are presented as median with IQR. A linear regression model was used to assess correlation between volume of fluid and ΔVAS. Multivariate analysis was performed to assess the effect of improvement in dyspnoea according to therapeutic aspiration group.
Study approval
Through discussion with the institutional research governance team, this study was deemed to be an audit of current practice not requiring specific ethical approval.
Results
Demographics
A total of 158 patients were included between 1 November 2013 and 1 June 2015; 84 were not included in the study due to refusal to complete the questionnaire, cognitive issues and loss of vision or missing data. There were no missing data on the collected forms of included patients. Mean age was 69 years, with 94 (57.0%) male patients. Baseline information and diagnoses are presented in table 1. Final diagnosis in all cases was based on positive histology, cytology or microbiology, or clinical follow-up for at least 3 months in the case of benign disease.
Details of diagnoses made in patients undergoing each procedure
Effect on breathlessness from pleural procedures
The patient-reported difference (ΔVAS) in dyspnoea varied between procedures. Excluding those who had diagnostic aspiration (32/158), the majority of patients (108/126, 85.7%) experienced symptomatic benefit from fluid drainage (mean VAS improvement 42.6 mm, SD 24.7, 95% CI 37.9 to 47.3). There were no statistical differences in ΔVAS for dyspnoea between major drainage procedures (figure 1) but all these procedures had a statistically larger effect on dyspnoea compared with diagnostic aspiration (diagnostic aspiration mean difference 7.4 mm, 95% CI 2.5 to 12.3 mm, p<0.05).
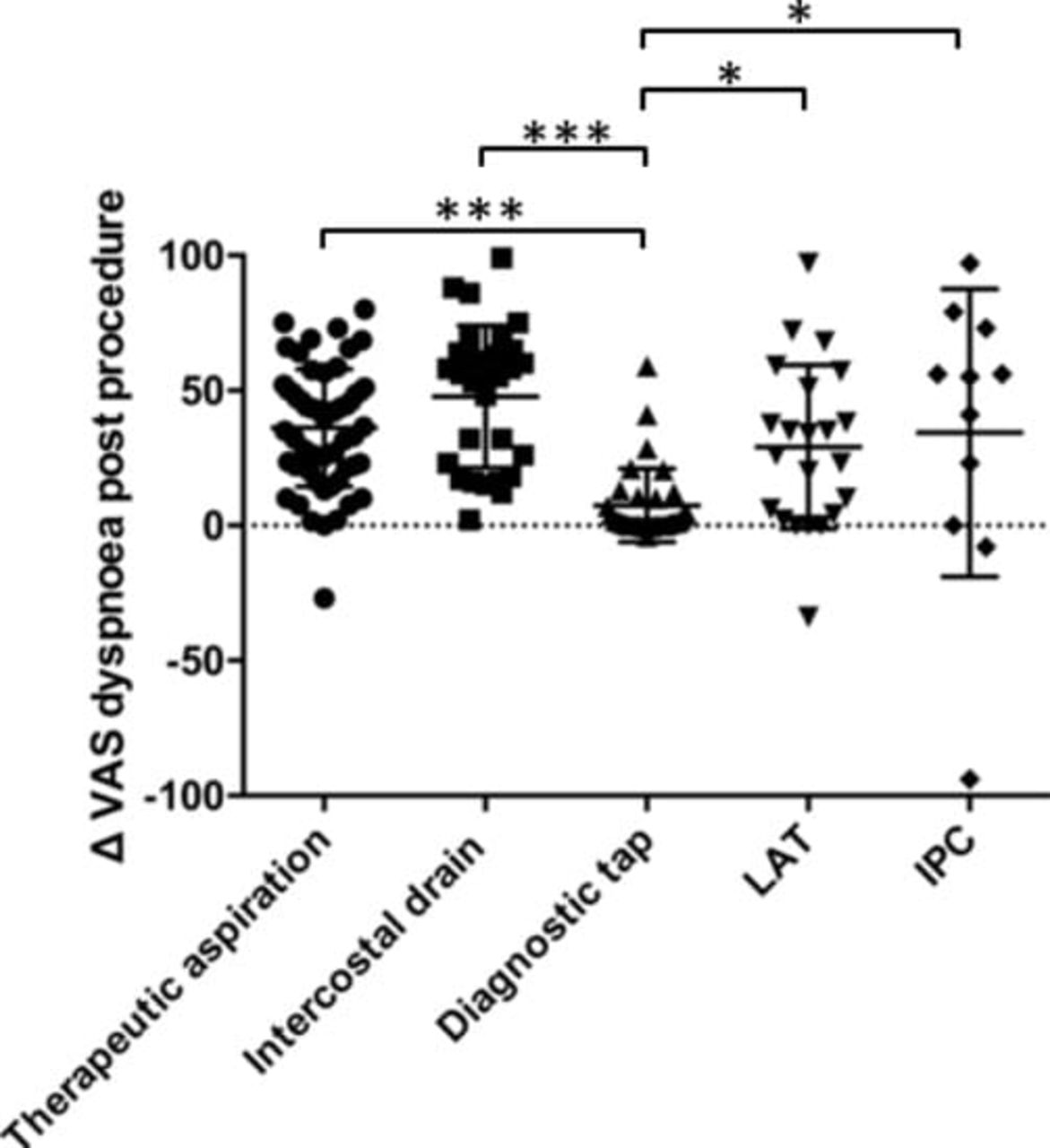
Change in visual analogue score (VAS) for dyspnoea post procedure for patients with pleural effusion. Data are presented as mean, SD. *p<0.05 and ***p<0.0001 demonstrate significant differences between groups. IPC, indwelling pleural catheter; LAT, local anaesthetic thoracoscopy.
Correlation of Likert score with ΔVAS
A total of 49/58 (84.4%) patients undergoing therapeutic aspiration (average volume of fluid aspirated was 955 mL) experienced clinical benefit post intervention (see online supplementary figure 1). Specifically 10/49 patients had trapped lung and were equally distributed between the three groups of individuals who had symptomatic improvement post-therapeutic aspiration (large or moderately better, slightly better but worthwhile, slightly better but not worthwhile). Of the nine patients who did not notice a change in breathlessness, four (44%) had evidence of trapped lung post aspiration on chest radiography and two (23%) had <550 mL of fluid aspirated due to symptoms (cough, chest tightness) during the procedure. In the remaining three (33%) patients, an underlying factor for lack of response could not be identified. There were no statistical differences between patients with trapped lung between improved and non-improved groups.
The majority of patients postdiagnostic aspiration (96%, 31/32) did not notice any change in breathlessness and 87.8% (29/33) of patients with ICD insertion experienced a significant change in breathlessness after the procedure. In total, 22 patients underwent medical thoracoscopy, 18 (81.8%) of whom noticed a slight but worthwhile improvement in breathing. Thirteen patients with MPE had an IPC insertion for fluid control, of whom 31% (four) indicated that the improvement in dyspnoea was ‘slightly better but worthwhile’ after the procedure and seven (69%) experienced a large or moderate improvement on their breathing.
VAS for pain
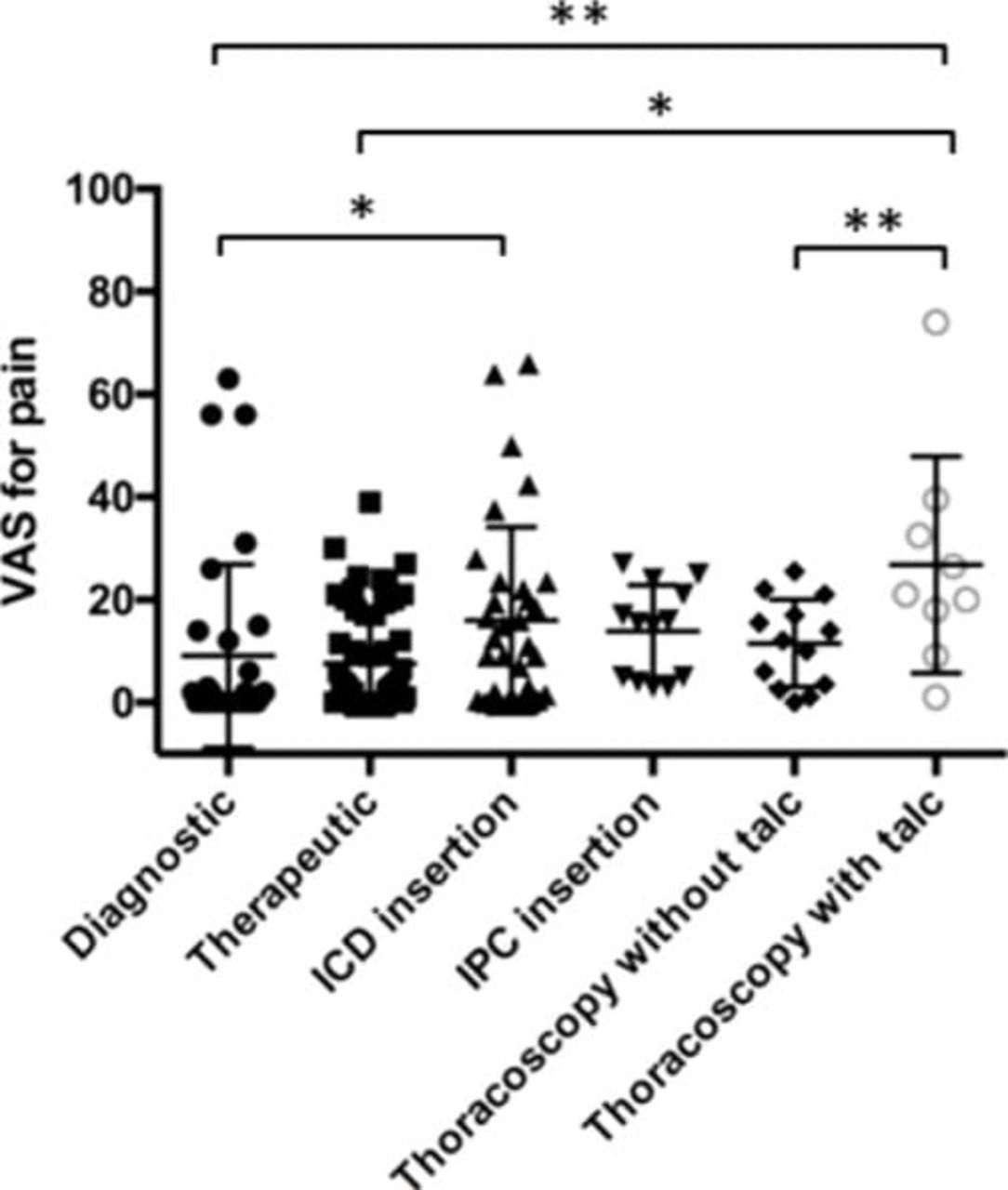
Average pain experienced across all pleural procedures was 12.2 mm (SD 25.7 mm, 95% CI 9.7 to 14.8 mm, figure 2). Diagnostic aspiration was not significantly different in pain experienced to therapeutic aspiration (difference −1.5 mm, 95% CI −7.4 to 4.3 mm, p=0.60). Both groups received the same volume of local anaesthetic. ICD insertion was significantly more painful than therapeutic aspiration (difference 8.4 mm, 95% CI 2.5 to 14.3 mm, p=0.0054). Pain was similar in ICD and IPC insertion groups (difference −2.1 mm, 95% CI −12.8 to 8.6 mm, p=0.69).
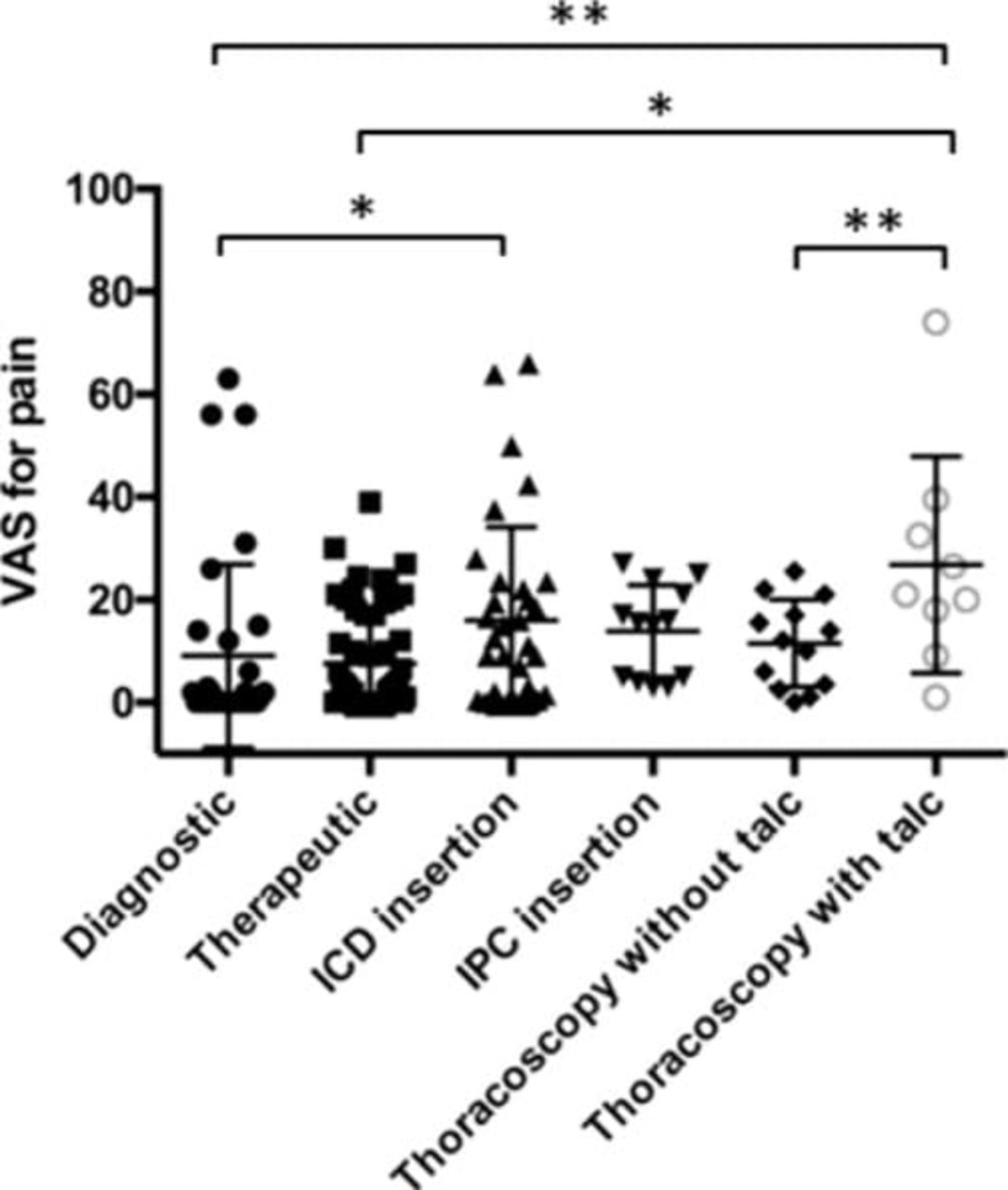
Visual analogue scale (VAS) for pain on different procedures. Patients with ICD experience significantly more pain compared with those who had a therapeutic aspiration. Patients who had talc poudrage felt significantly more pain compared with those who had diagnostic thoracoscopy. Data are presented as mean, SD. *p<0.05 and **p<0.001 demonstrate significant differences between groups. IPC, indwelling pleural catheter.
Patients undergoing thoracoscopy experienced more pain with talc poudrage compared with those undergoing diagnostic thoracoscopy only (difference 15.3 mm, 95% CI 1.8 to 28.7 mm, p=0.02). The doses of local anaesthetic and sedation (fentanyl and midazolam) used were not different between these two groups.
Exploratory analyses: VAS for dyspnoea associates with fluid removal
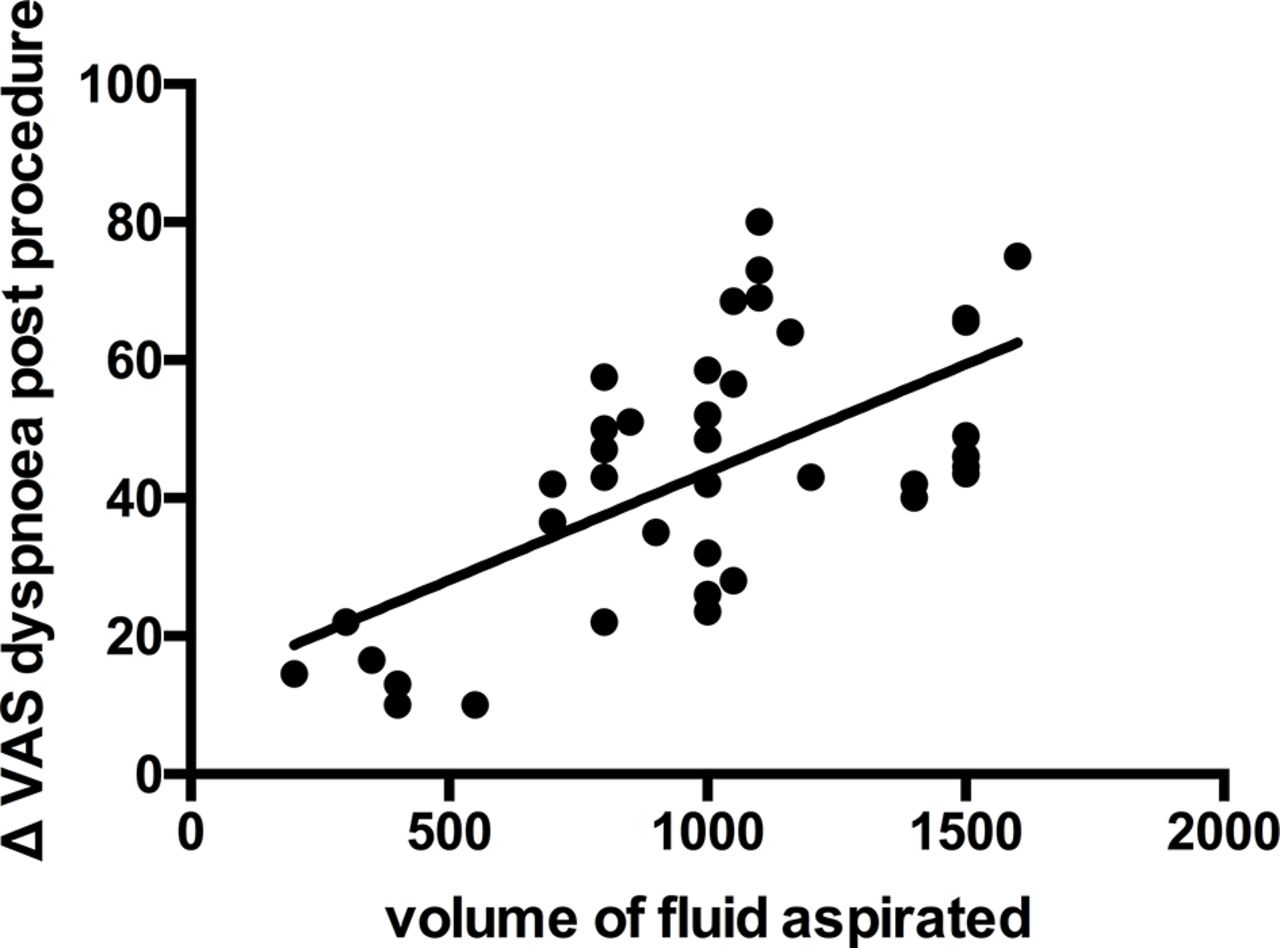
Improvement in patients’ dyspnoea was correlated with the volume of fluid drained after therapeutic aspiration. VAS improvement correlated with the volume of fluid drained (figure 3, r2=0.54). The volume of fluid aspirated ranged from 200 to 1500 mL (stopped at 1500 mL due to local department drainage policy).
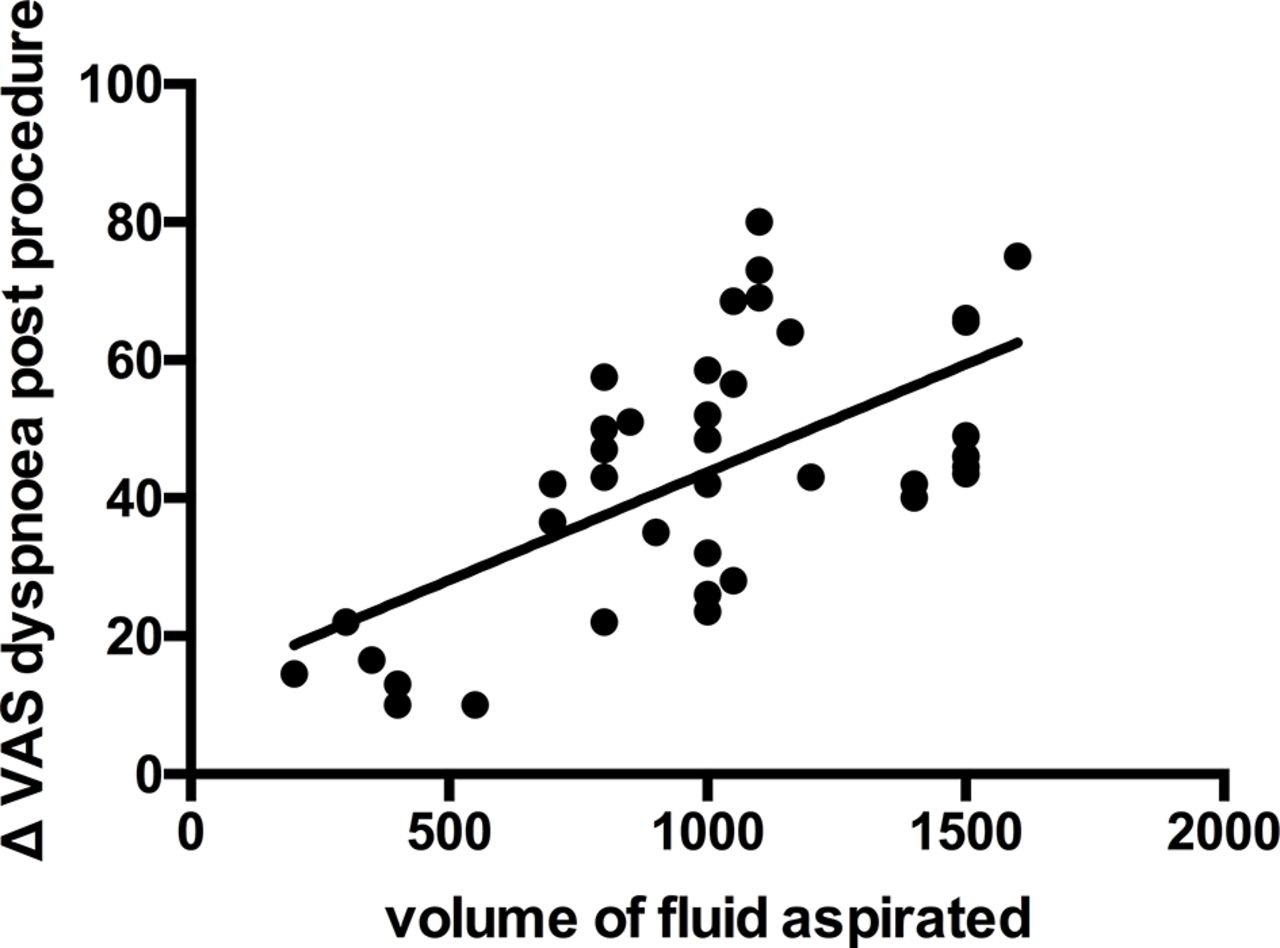
Correlation of volume output with difference in visual analogue scale (VAS) for dyspnoea for patients with therapeutic aspiration. Circles represent individual data points and solid line the best line that fits. (r2=0.54, p<0.0001).
Dyspnoea improvement correlates with the number of septations
In the ICD group, the number of septations on US was negatively correlated with dyspnoea improvement (figure 4). Those with an average of >5 septations per US image had less improvement in dyspnoea compared with those with <5, and this appeared to be unrelated to the volume of fluid removed (p=0.08, non-parametric comparisons due to small group size). In the former group (>5 septations), 66.6% (2/3) of the patients had trapped lung.

{kind=link}
![[Supplementary_Figure1.jpg]](https://bmjopenrespres.bmj.com/content/bmjresp/4/1/e000171/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
The number of septations on ultrasound (US) is correlated with the improvement in dyspnoea after ICD insertion. Data are presented as median with IQR (p=0.08, non-parametric comparisons). VAS, visual analogue scale.
To explore the relationship between volume of fluid, improvement in VAS and number of septations, post hoc analyses were performed. Both volume of fluid (p=0.02) and number of septations (p=0.01) correlated with improvement in VAS. Multivariate analysis using volume of fluid drained and number of septations as the dependant variables and VAS change as the outcome demonstrated that only number of septations remained significant within the model, suggesting it is the only independent predictor of VAS change (p=0.02).
Patients’ perception of the pleural service
A total of 135/158 (87%) of patients were satisfied with the service and did not provide specific comments. The most common comments from patients were the waiting time and pain of the procedure. In total, 156/158 (99%) patients were willing to repeat the same procedure if clinically required. The two patients who were not willing to repeat the procedure had undergone a diagnostic aspiration (20 mL of local anaesthetic used and found the procedure painful) and an IPC insertion (MPE with evidence of trapped lung on chest X-ray, 1500 mL of fluid drained and no improvement in dyspnoea 1 hour postinitial drainage).
Discussion
This is the first study to our knowledge that specifically explores the effect of different pleural procedures on PROMs, including outcomes of importance to patients. As the treatment intent in many such procedures is symptom amelioration, provision of validated data on the symptom effect of such interventions is required to provide rational care for patients. Our findings identified a correlation between fluid removal and improvement in patients’ dyspnoea and a novel predictor of symptomatic response (septation score).
The results demonstrate a number of key findings that should be useful in the future management of patients with pleural effusion due to undergo intervention. The majority of patients (108/126, 85.7%) experience symptom benefit from drainage and reported improvement in terms of breathlessness (on the Likert scale). However, even where specialist clinicians have selected patients for procedures thought to be of potential benefit, 14.3% of patients undergoing therapeutic aspiration did not experience a worthwhile change in breathlessness. These are important data when consenting patients for such procedures and may justify conducting a therapeutic aspiration in all patients prior to offering definitive treatment. Pleural procedures are associated with potential significant harm, and being able to predict which patients will not gain symptom relief would be of great value.17
Of those with a poor symptomatic response, 71% had either trapped lung or <550 mL of fluid drained due to cough or chest tightness as a result of fluid removal. For the remaining 29%, we assume these patients had other, parallel reasons for breathlessness, with fluid being a minor contributor to symptoms. However, the average fluid drained in patients with a lack of meaningful symptomatic response was 836 mL, enforcing the idea that volume of drainage alone and therefore size of effusion may not always be related to symptom benefit.
Our results provide potentially important information on a novel predictor of symptomatic response that is available prior to drainage. The septation score at preprocedure US was inversely associated with symptomatic benefit from drainage. Although this effect may be assumed to be related to the amount of fluid drained (as more septated effusions may lead to less drainage of fluid), multivariate analysis suggests that the septation score is independently predictive of symptom change when accounting for volume of fluid. The mechanism of this effect is not completely clear, and we speculate that the septations correlate with reduced fluid drainage, but may also act as a marker for another intrathoracic process (such as visceral pleural thickening or more advanced disease), which may be the reason behind poorer symptomatic response. If replicated in future studies, this may be an important factor available prior to any drainage procedure that allows prediction of poor symptomatic response.
Most clinicians would consent patients undergoing pleural procedures for the procedure being painful, but precise data on the pain associated with such procedures have not until now been available. The pain data in this study are highly informative in this regard, but also demonstrate some surprising results. Medical thoracoscopy without poudrage, for example, was not significantly different in terms of pain to standard ICD insertion. This lack of difference may reflect the use of increased doses of anaesthetic and sedation in thoracoscopy patients, but does provide reassurance for patients. Talc poudrage has here been associated with a doubling in pain levels (11.5 vs 26.8 mm) and this again provides important information in obtaining patient consent and the provision of adequate analgesia post procedure. In our centre, intravenous opiates were not given to the patients prior to thoracoscopy and baseline pain levels prior to the procedure were not assessed in our study.
One particularly interesting finding which should influence current practice is the relative pain experienced in those undergoing diagnostic aspiration. Pain experienced was no different comparing diagnostic aspiration using a 21G needle (outer diameter 0.82 mm) and therapeutic aspiration using 6F catheters (outer diameter 3 mm) despite the use of similar doses of local anaesthetic in our practice. This suggests that local anaesthesia should be used even in diagnostic procedures in all cases.
There are limitations to this work. Patients were assessed from one hospital which is a tertiary referral centre for pleural disease. This study only assessed symptom change at 1 hour post procedure for day-case procedures, and 24 hours for inpatients, and potentially longer-term studies are required to follow-up this work. Potentially, an amnesic effect from slight sedation could affect patients’ responses but the exact extent of the effect is difficult to assess. Lastly, there is a potentially significant number of confounding factors that contribute to PROMs which are difficult to assess in our data set (eg, prior drainages, different diagnosis). A larger multicentre, multinational study is needed to confirm our results in the future.
This study is the first to prospectively address PROMs in pleural interventions in real-life practice. The outcomes defined in our data set have the potential to be employed in everyday clinical practice and may form the basis of a clinically useful tool in the future to appraise the effect, compare the efficiency and identify the importance of pleural interventions to the patients.
Acknowledgments
The authors thank the Respiratory Interventional Nurses, Oxford Centre for Respiratory Medicine, for their assistance on questionnaire collection, Maria Bantouna for her assistance on graph design and Kanellakis for the help in statistical analysis.
References
Footnotes
Contributors IP and NMR conceived the article, collected and analysed the data and wrote the manuscript; had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. EKM and NA designed the questionnaire for PROMs, critically revised and approved the final manuscript. AY, AT, RJH and JPC provided data on cases, critically revised and approved the final manuscript.
Funding Psallidas I is the recipient of a REPSIRE2 European Respiratory Society Fellowship RESPIRE2 – 2015 – 7160. Rahman NM is funded by the National Institute Health Research (NIHR) Oxford Biomedical Research Centre. Hallifax RJ is funded by a Clinical Training Fellowship from the Medical Research Council (MR/L017091/1). The founding sources have no role in writing the manuscript or the decision to submit it for publication. Psallidas I and Rahman NM had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Disclaimer The founding sources have no role in writing the manuscript or the decision to submit it for publication.
Competing interests IP is the recipient of a REPSIRE2 European Respiratory Society Fellowship RESPIRE2-2015-7160. NMR is funded by the National Institute Health Research (NIHR) Oxford Biomedical Research Centre. RJH is funded by a Clinical Training Fellowship from the Medical Research Council (MR/L017091/1).
Patient consent The study has been discussed with the ethical committee in University of Oxford and is considered an audit of practice. Patient consent forms have not been obtained.
Ethics approval The study has been discussed with the ethical committee in University of Oxford and is considered an audit of practice.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests for access to data should be addressed to the corresponding author.