Article Text

Abstract
Introduction The Beta Agonist Lung Injury Trial-Prevention (BALTI-P) translational substudy and Vitamin D to Prevent Acute Lung Injury Following Oesophagectomy (VINDALOO) trials recruited patients undergoing oesophagectomy, 4 years apart. The acute respiratory distress syndrome (ARDS) rates were lower in the VINDALOO trial. We sought to identify changes between these two trials and identify risk factors for ARDS in oesophagectomy.
Methods There were data available from 61 patients in the BALTI-P substudy and 68 from VINDALOO. Databases were available for both trials; additional data were collected. Multivariate logistic regression was used to analyse risk factors for ARDS and postoperative complications in the cohorts combined.
Results Logistic regression analysis showed active smoking was associated with an increase in ARDS (OR 3.91; 95% CI 1.33 to 11.5) and dihydropyridine use (OR 5.34;95% CI 1.56 to 18.3). Hospital length of stay was longer for those who took dihydropyridines (median 29 days (IQR 17–42) vs 13 days (IQR 10–18), P=0.0007) or were diabetic (median 25 days (IQR 14–39) vs 13 (IQR 10–19), P=0.023) but not for current smokers (median in never/ex-smokers 13 (IQR 10–23) vs current smokers 15 (IQR 11–20), P=0.73).
Conclusions Smoking cessation trials should be promoted. Dihydropyridine effects perioperatively require further clinical and mechanistic evaluation. Patients undergoing oesophagectomy are a useful model for studying perioperative ARDS.
- ards
- tobacco and the lung
- drug induced lung disease
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Key messages
ARDS following oesophagectomy is associated with adverse outcome.
Smoking and dihydropyridines are associated with postoperative acute respiratory distress syndrome (ARDS) in oesophagectomy. Although the cohort appears to be changing, oesophagectomy remains a useful clinical model of ARDS.
Introduction
Patients undergoing oesophagectomy have high rates of postoperative complications1 including the acute respiratory distress syndrome (ARDS).2 We have previously shown that ARDS following oesophagectomy is associated with more non-respiratory organ failure, longer critical care and hospital stays,3 and other groups have demonstrated worse short-term and long-term outcomes associated with ARDS2 and other pulmonary complications.4 Severe infection and cardiac dysrhythmias are common.5–7 However, this high complication rate, alongside the planned nature of surgery and the clear timing of the surgical insult, makes oesophagectomy a potentially useful model to undertake trials to reduce perioperative complications.8
Both the Beta Agonists in Lung Injury Trial-Prevention (BALTI-P),9 which completed recruitment in 2011, and the Vitamin D to Prevent Acute Lung Injury Following Oesophagectomy (VINDALOO) trials, completed in 2015,10 used oesophagectomy as a model of ARDS. We observed that the incidence of ARDS in the VINDALOO (8 out of 68, 11.8%) cohort was substantially lower than in the BALTI-P (83 out of 331, 25.1% and 14 out of 61, 23%) substudy (see the Methods section below), independent of a pharmacological effect of the agents trialled, suggesting that there had been changes between the groups that were expected a priori to be similar.
The aims of this work were to determine which clinical features were different between the two cohorts that might explain the differences in postoperative ARDS and complications. The combined cohorts were analysed to seek further risk factors not apparent in the individual cohorts and potential therapeutic targets for further investigation.
Methods
Details of the methods of the BALTI-P trial and the associated translational substudy have been published previously.9 Patients were randomised to either placebo or inhaled salmeterol preoperatively and postoperatively. At two hospital sites (Queen Elizabeth Hospital Birmingham and Birmingham Heartlands Hospital, UK), patients were recruited to the translational substudy. The VINDALOO trial protocol has been published.10 Patients were recruited at Queen Elizabeth Hospital Birmingham and Birmingham Heartlands Hospital, UK, and randomised to either placebo or a single dose of 300 000 IU of vitamin D. In both studies, patients underwent oesophagectomy with care provided as deemed clinically appropriate by the attending surgeons and anaesthetist and followed for their hospital stay.
Databases of the outcomes from the two trials were available for analysis. Smoking status was self-reported in both trials. We collected additional data retrospectively using medical notes, intensive care unit (ICU) charts, electronic patient databases and clinical letters, which provided the preoperative drug history, data for preoperative risk scoring and intraoperative drugs used. The administration of regular medications on the morning of surgery was at the discretion of the attending anaesthetist. In the BALTI-P substudy, patients were excluded if they did not undergo an oesophagectomy with attempted one lung ventilation (OLV). In VINDALOO, only patients who passed the primary endpoint of oesophagectomy with OLV and postoperative PICCO readings were included (consistent with the VINDALOO trial’s analysis).
Differences in the baseline characteristics and perioperative care between trials were assessed. Outcomes for both trials were determined by a clinical endpoints committee. ARDS was defined using the Berlin criteria11 for the VINDALOO trial. The BALTI-P trial pre-dates the Berlin criteria, which could not be applied, as applied positive end-expiratory pressure was not recorded. Therefore, we defined ARDS in the BALTI-P trial participants as those with a Pao2:Fio2 (P:F) ratio of 39.9 kPa or below, bilateral chest X-ray infiltrates, attending physician exclusion of cardiogenic dysfunction and requiring invasive ventilation (ventilation with positive end-expiratory pressure of 5 cm H2O was standard care in the ICUs involved and non-invasive ventilation was contraindicated in patients following upper gastrointestinal surgery at the time both trials were undertaken).
Continuous variables were subject to normality testing using the Kolmogorov-Smirnov test. For the patients’ baseline data and univariate analysis of perioperative factors, normally distributed continuous variables were analysed with Student’s t-test, non-normally distributed data with the Kruskal-Wallis test and Mann-Whitney U-test and categorical data with the Χ2 or Fisher’s exact test as appropriate. Those factors that were significant (P<0.05) were then subject to multivariate analysis. Multivariate analysis of ARDS status was undertaken using forward conditional multivariable binomial logistic regression of the two significant factors in the univariate analysis. Analyses of baseline and univariate data were undertaken using GraphPad Prism V.6.07 for Windows (GraphPad Software, La Jolla, California, USA). Multivariate analyses were performed using SPSS Statistics V.22.0 for Windows.
Results
Table 1 shows the baseline demographic data from the BALTI-P substudy and VINDALOO groups. Patients in VINDALOO were heavier, received a lower mean tidal volume, received more intravenous fluid, more were on beta-blockers, more received ketamine and dexamethasone and fewer remifentanil and thoracoscopic approach was more common.
Demographic data from the two trials
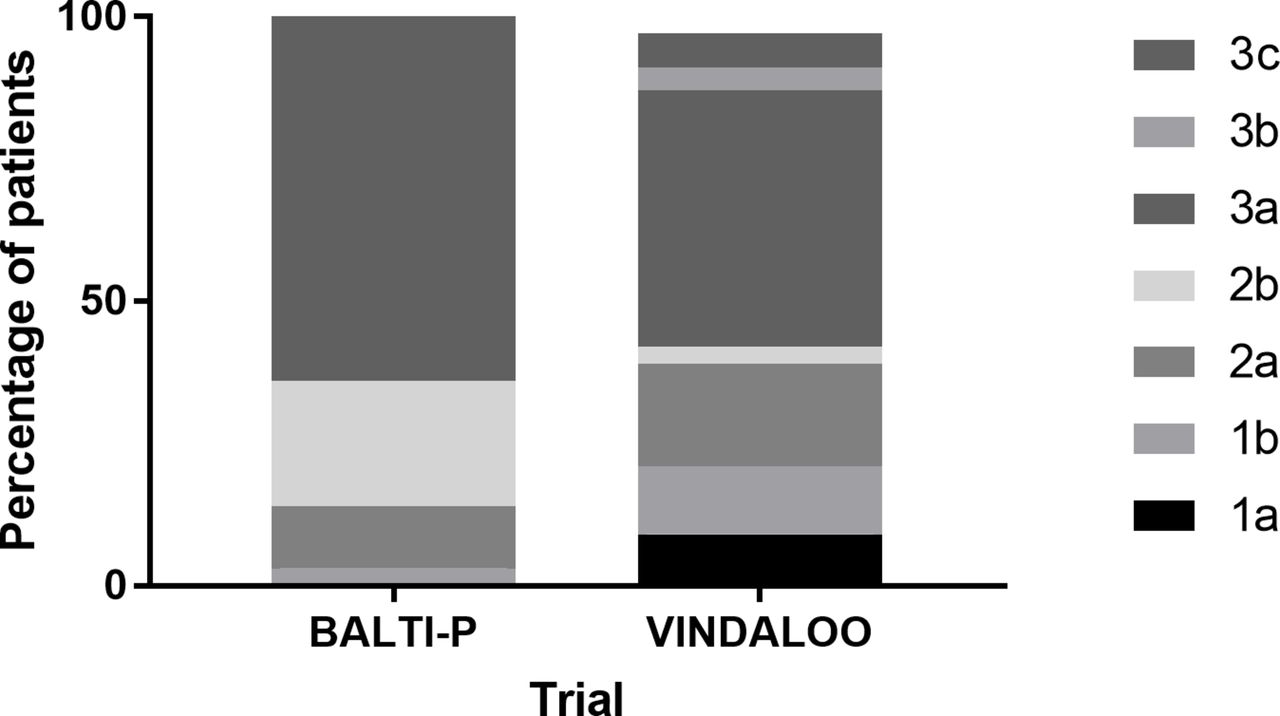
Staging of malignancy was both more widely distributed and overall higher in the VINDALOO cohort (figure 1). Pre-existing Charlson Index was not different between groups (BALTI-P median 2 (IQR 2–3), VINDALOO 2 (IQR 2–3), P=0.872). Perioperative risk scores were not different between the groups (P-POSSUM Mortality (BALTI-P median 2.4 (IQR 1.9–37) vs VINDALOO 2.4 (IQR 1.5–5.4), P=0.759), P-POSSUM Morbidity (BALTI-P median 8.5 (IQR 4.6–13) vs VINDALOO 8.7 (IQR 6.3–17), P=0.141), O-POSSUM (BALTI-P median 8.5 (IQR 4.6–13) vs VINDALOO 8.7 (IQR 6.3–17), P=0.141)).

{kind=link}
Percentage of patients per stage of oesophageal cancers in the two trials, overall difference P<0.001. BALTI-P Stage 1b n=2, 2a n=6, 2b n=12, 3a n=34, missing/incomplete n=7; VINDALOO 1a n=6, 1b n=8, 2a n=12, 2b n=2, 3a n=29, 3b n=3, 3c n=4, missing/incomplete n=4. BALTI-P, Beta Agonist Lung Injury Trial-Prevention; VINDALOO, Vitamin D to Prevent Acute Lung Injury Following Oesophagectomy.
To assess risk factors further, the two cohorts were combined and assessed according to ARDS status (table 2). Univariate analysis showed that current smoking and dihydropyridine use were associated with the development of ARDS postoperatively. These variables were then subject to multivariate analysis, which showed that both active smoking (OR 3.91; 95% CI 1.33 to 11.5) and dihydropyridine use (OR 5.34; 95% CI 1.56 to 18.3) remained associated with ARDS risk.
Comparison of patients with ARDS
The effect of these factors on length of stay as a measure of outcome was assessed, as this outcome was collected in both trials. This showed that those patients on dihydropyridines had longer hospital stays (dihydropyridine median 29 days (IQR 17–42), no dihydropyridine 13 days (IQR 10–18), P=0.0007), as did those with diabetes mellitus (diabetes median 25 (IQR 14–39) vs no diabetes 13 (IQR 10–19), P=0.023). There was no difference in length of stay related to smoking (median in never/ex-smokers 13 (IQR 10–23) vs active smokers 15 (IQR 11–20), P=0.73).
Discussion
Lower tidal volume is now well established in the management of ARDS following the landmark ARDS Clinical Network trial12 and there is increasing evidence of its role in intraoperative ventilation.13 14 Tidal volumes were lower in the VINDALOO trial, which is likely to represent the increasing adoption of lung protective strategies, including lower tidal volumes, higher positive end-expiratory pressure and permissive hypercarbia.5 Whether the reduction of 0.8 mL/kg is clinically significant is not certain, but may be in the context of OLV during oesophagectomy, where less than half the lung volume is subject to intermittent positive pressure ventilation.15 This may have played an important role in the change in ARDS incidence. More fluid was administered to the VINDALOO cohort; this might represent a reduction in colloid and increased crystalloid administration and/or more balanced fluid use improving anastomosis perfusion.6 Similarly, increasing the use of thoracoscopic techniques and anaesthetic agents with immunomodulatory effects may reduce the inflammatory response to surgery and so the risk of ARDS.3 5
This study has indicated that there are two major targets for reduction in postoperative ARDS: cigarette smoking and diyhdropyridines. Smoking has been previously demonstrated to be a risk factor for ARDS,16 17 and the fewer current smokers in VINDALOO may have had a marked effect on the ARDS incidence between the two trials. Smoking has been associated with severe perioperative complications in another oesophagectomy cohort.18 This work supports the premise of efforts to reduce smoking perioperatively.19 Use of nicotine replacement therapy in critical care medicine is controversial, and trials in the perioperative setting are required to ensure safety as well as efficacy.20 Evidence of the safety and effectiveness of e-cigarettes and nicotine replacement in the perioperative period also need to be confirmed by randomised trials.21
The association between dihydropyridine calcium channel blockers and ARDS was unexpected. ARDS has been reported following dihydropyridine overdose.22 Pulmonary oedema following administration of the dihydropyridine nimodipine has been described in the context of subarachnoid haemorrhage.23 Potential mechanisms include worsened ventilation-perfusion mismatching due to pulmonary arterial dilatation, reduced cardiac function and pulmonary or inflammatory modulatory effect. Calcium channel blockade has been associated with immunomodulation, although mostly downregulating inflammatory processes.24–26 It may be that dihydropyridine use is a marker of worse systemic disease and therefore perioperative risk, although we did not find an association with aspirin, beta-blockers or statins. It would be premature to recommend not using dihydropyridines in the perioperative period, but there is a need for further studies on the effects of concurrent medications on patients undergoing surgery. Such work is underway studying ACE inhibitors (SPACE trial EudraCT 2016-004141-90). Identifying the mechanisms through which dihydropyridines have this effect would also be useful.
A major problem in ARDS prevention trials is identifying a cohort with a high ARDS risk.8 Even in the VINDALOO cohort, the ARDS incidence remains higher than that defined by the Lung Injury Prediction Score27 28 and the postoperative complication incidence is very high, with the advantages of an initial insult of surgery at a specific time and a defined postoperative care pathway,3 which facilitates the conduct of efficacy trials. We believe this work demonstrates that oesophagectomy continues to be a useful model for trialling translational therapeutic and preventative strategies for critical illnesses prior to engaging in larger, more complex and expensive trials.8 Examples include the Prevention of Postoperative Pulmonary and Cardiac Complications By Using HMG-CoA Reductase Inhibitor in Patients Undergoing Oesophagectomy (EudraCT Number: 2007-002454-37) and a trial of novel agent GSK2862277 (TFR116341 Trial EudraCT Number: 2014-000643-33).
There are several weaknesses with this investigation. This is a retrospective study and may well be underpowered for some factors, although this work was intended only to be exploratory and hypothesis generating. Much of the data we collected were retrospective and full data were not available for every patient. Additionally, some factors that may be important risk factors for both ARDS and oesophageal cancer, including alcohol consumption,17 were not recorded. There were significant differences in potentially important factors in anaesthetic management, discussed above, which potentially complicate comparisons made over time without protocolised surgical or anaesthetic management.
In conclusion, smoking has been associated with higher rates of ARDS following oesophagectomy. The association of dihydropyridines and ARDS requires validation in a larger cohort and mechanistic elucidation. Oesophagectomy continues to have a high risk of ARDS, which continues to offer a useful model for perioperative studies.
Acknowledgments
We would like to thank Dr Peter Nightingale, Statistician at the University of Birmingham, for his advice on the analyses used in this paper. The BALTI-P study was supported by the National Institute for Health Research. The VINDALOO study was funded by the Medical Research Council. PAH is funded by a grant provided by GlaxoSmithKline. DRT is funded by the Medical Research Council. FG and GDP receive support as National Institute for Health Research Senior Investigators. GDP is supported as a Director of Research for the Intensive Care Foundation.
References
Footnotes
Contributors PAH and DRT conceived the study. OT, RCAD, FG, GDP and DRT were involved in the design and execution of the trials on which this work was based. PAH and KAA collected additional data and conducted the statistical analysis. All authors were involved in the revision and substantial intellectual contributions to the manuscript.
Competing interests PAH is supported by a grant from Glaxo Smith Kline. DP and DRT are supported by the Medical Research Council. GDP has undertaken paid consultancy for Glaxo Smith Kline. GDP and FG are National Institute for Health Research Senior Investigators. GDP is supported as a Director of Research for the Intensive Care Foundation.
Patient consent Obtained.
Ethics approval South Birmingham Research Ethics Committee approved both trials from which data were retrieved.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.