Article Text

Abstract
Introduction Hospital and emergency department discharge for patients with chronic obstructive pulmonary disease (COPD) is often poorly organised. We developed a patient-centred, evidence-based and consensus-based discharge care bundle for patients with acute exacerbations of COPD.
Methods A purposeful sample of clinicians and patients were invited to participate in a two-round Delphi study (July–November 2015). In round 1, participants rated on a seven-point Likert scale (1=not at all important; 7=extremely important) the importance of 29 unique COPD care actions. Round 2 comprised items selected from round 1 based on consensus (>80% endorsement for Likert values 5–7). A list of 18 care items from round 2 was discussed in a face-to-face nominal group meeting.
Results Seven care items were included in the COPD discharge bundle based on clinician and patient input: (1) ensure adequate inhaler technique is demonstrated; (2) send discharge summary to family physician and arrange follow-up; (3) optimise and reconcile prescription of respiratory medications; (4) provide a written discharge management plan and assess patient’s and caregiver’s comprehension of discharge instructions; (5) refer to pulmonary rehabilitation; (6) screen for frailty and comorbidities; and (7) assess smoking status, provide counselling and refer to smoking cessation programme.
Conclusion We present a seven-item, patient-centred, evidence-based and consensus-based discharge bundle for patients with acute exacerbations of COPD. Alignment with clinical practice guidelines and feasibility of local adaptations of the bundle should be explored to facilitate wide applicability and evaluation of the effectiveness of the COPD discharge bundle.
- copd exacerbations
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
How is the consensus among expert clinicians and patients about the inclusion of individual care items into a discharge care bundle for patients with acute exacerbation of chronic obstructive pulmonary disease (COPD)?
Seven evidence-based care items were included in a COPD discharge bundle based on clinician and patient input.
This is the first use and reporting of a modified Delphi method to develop a COPD discharge care bundle informed by evidence, multidisciplinary clinical consensus and patients’ perspectives.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, chronic lung disease characterised by progressive and not fully reversible airflow limitation. Acute exacerbations of COPD are defined by worsening in patients’ baseline symptoms of dyspnoea, cough and sputum (quantity and purulence); exacerbations become more frequent and severe as the disease progresses.1 These events constitute the single most important determinant of health status in patients with COPD2 and account for increased morbidity, frequent emergency department (ED) visits, hospitalisations and death.3 4
A cornerstone of COPD management is preventing acute exacerbations of COPD and breaking the cycle of recurrence. A large body of evidence supports both pharmacological and non-pharmacological interventions to reduce the risk of acute exacerbations of COPD and improve overall health status.5 Despite this evidence, important care gaps remain as patients are often discharged from hospital or the ED following an acute exacerbation of COPD with no clear plan to prevent future episodes.6 Information exchange between hospital, ED and primary care physicians about the acute exacerbation of COPD is often incomplete or unavailable at the first postdischarge outpatient appointment.7 Often, patients and families assume care coordination responsibilities and personally convey follow-up instructions to primary care physicians. Information is sometimes provided verbally, and patients often struggle with health literacy issues.8 9 This creates a critical situation in which inaccurate information is translated from acute to community care settings. There is a need to improve transitions of care for patients with COPD across ED, hospital and community settings and ensure coordination and continuity of care.10
Care bundles aim to meet these challenges and overcome inconsistencies in clinical decision-making while supporting the translation of evidence to enhance COPD care. The Institute for Healthcare Improvement has defined care bundles as ‘a structured way of improving the processes of care and patient outcomes: a small, straightforward set of evidence-based practices that, when performed collectively and reliably, have been proven to improve patient outcomes’.11 A COPD discharge care bundle comprises a short list of evidence-based interventions that should be implemented prior to discharge of all patients with acute exacerbations of COPD.12
A systematic review on the effectiveness of COPD discharge care bundles13 found moderate evidence that their implementation is likely to reduce readmissions after acute exacerbations of COPD. The review highlighted the importance of documenting the individual components of care bundles and understanding their interactions to influence patient outcomes. Ideally, the decision to include individual interventions in a COPD discharge bundle should be guided by best evidence, clinical expertise and patient values.14 Despite the existence of clinical practice guidelines for COPD,1 4 15–18 there is no consensus about the core COPD care items that should be implemented at discharge to ensure a smooth transition to the community and reduce the risk of relapse.19 This study describes the development of a discharge care bundle for patients with COPD that is based on evidence, consensus among clinical experts and patients’ feedback.
Methods
The study was conducted from July to November 2015 and consisted of a two-round, modified Delphi survey plus one face-to-face nominal group meeting.20 The Delphi procedure is an explorative approach that uses a series of questionnaires to gather information about a topic of relevance to the participants in the study.21 It comprises distinct characteristics: anonymity, iteration, controlled feedback and statistical group response as expression of the degree of consensus.21 22 The aim of the process is to find consensus within a group of experts. In this study, patients were also regarded as experts for their individual experiences with accessing COPD care.
A purposeful sample of 340 clinician experts was invited to participate. They were selected based on their clinical and research experience in the evaluation and treatment of patients with COPD. The study population included health providers involved in various aspects of COPD care (ie, hospital, emergency and primary care) in Alberta (Canada), and all members of the Canadian Thoracic Society (CTS) COPD Clinical Assembly. Names of Alberta clinician experts were obtained from websites of the College of Physicians and Surgeons of Alberta, the College and Association of Respiratory Therapists of Alberta, clinical departments at the University of Alberta and University of Calgary, and Alberta Health Services, which is the single health authority for the province. A convenience sample of 34 patients with COPD was recruited from two multidisciplinary respiratory clinics in Edmonton and Calgary (Alberta) using flyers distributed during their clinical appointments and by health providers’ referral. Since the aim was to recruit ‘representative’ patients in terms of their experiences with COPD care at hospital discharge and not a representative overall sample, no exclusion criteria by COPD severity or demographic characteristics were applied.
Clinical experts were individually contacted by email, and patients were contacted in person. Each received a letter of consent describing the study and the expectations regarding their participation. A list of 29 unique COPD care actions occurring at either hospital or ED discharge was derived from a systematic review of the literature13 and clinical practice guidelines,4 15–18 23 and included in the round 1 questionnaire. The questionnaires were pretested with a sample of two clinician experts and two patients not involved in subsequent Delphi rounds. The content of the patients’ questionnaires was adapted for a grade 6 level of reading to enhance comprehensiveness and acceptance.
Figure 1 describes the study flow. In round 1, participants rated the importance of 29 unique COPD discharge care items on a seven-point Likert-type scale (1=extremely unimportant and 7=extremely important). In round 2, participants were presented with a list of COPD discharge items for which consensus was achieved in round 1 along with the group’s ratings. Participants were asked to reflect on the group responses and rate the importance of each COPD discharge item. For all Delphi rounds, consensus about the importance of individual COPD care items was defined a priori as at least 80% of endorsement for Likert values 5–7. Both first-round and second-round questionnaires for clinicians were distributed online via Research Electronic Data Capture (Vanderbilt University; Nashville, Tennessee, USA). The round 2 questionnaire was sent to all clinicians regardless of their participation in the first round. Non-respondents were sent two reminders at 2-week intervals after the initial distribution. Patients participating in round 1 were invited to complete the round 2 questionnaire at their next follow-up clinical visit. A face-to-face, nominal group meeting was convened in Edmonton on 16 November 2015. The 44 participants included the CTS COPD Clinical Assembly, clinicians, researchers and health administrators from Alberta with experience in COPD care. Results of Delphi rounds 1 and 2 were presented to meeting participants. They were invited to add new care items and review their wording prior to voting. Using a dot-counting method,24 participants selected individual care items for inclusion in the COPD discharge bundle based on the information gathered from the Delphi rounds, the systematic review,13 clinical expertise and patients’ feedback. The level of consensus for voting of individual COPD care items during the nominal group meeting was indicated by values above the median rank value.25
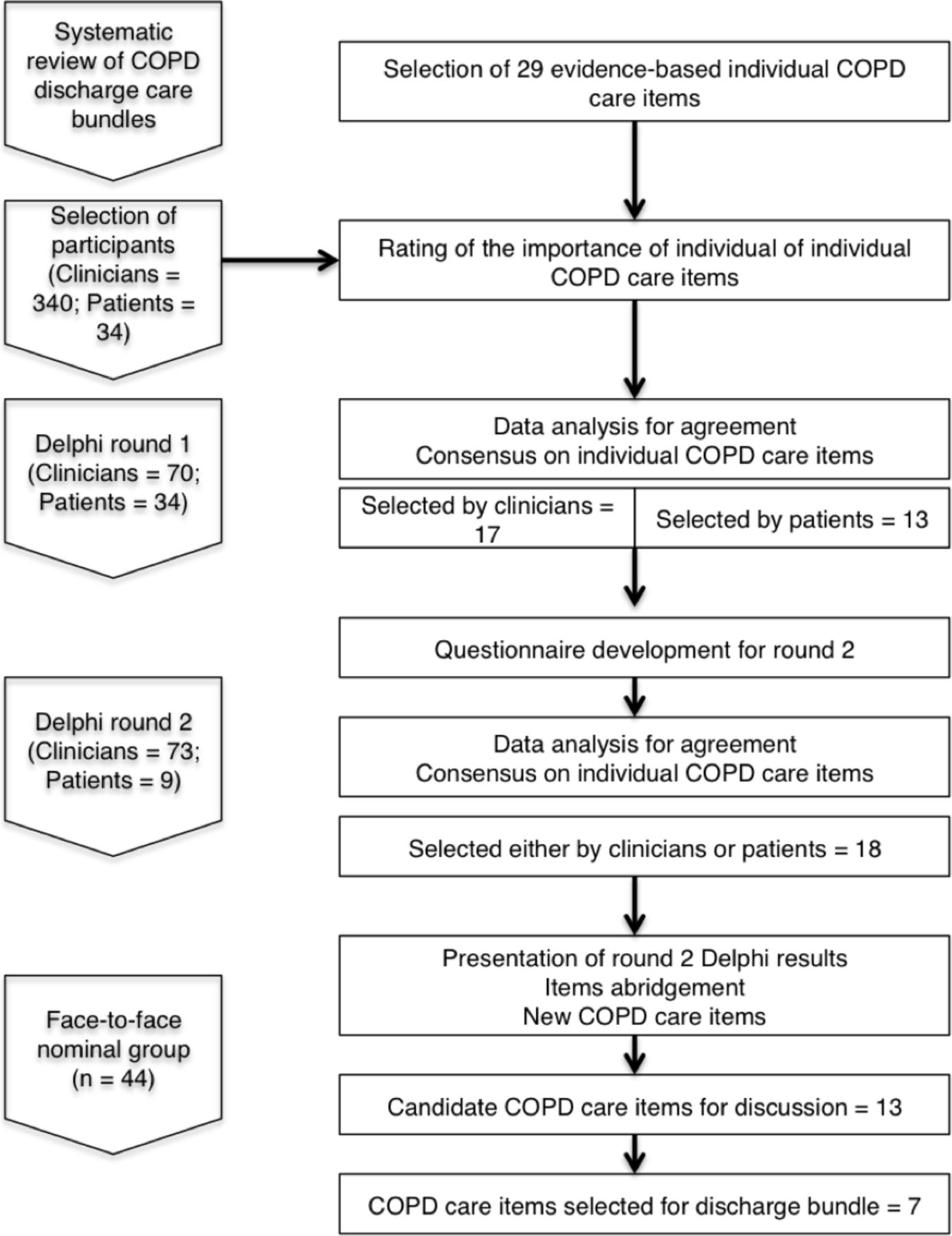
Flow diagram of Delphi procedures and study participants. COPD, chronic obstructive pulmonary disease.
Descriptive statistics were used to report consensus. The level of agreement between clinicians and patients in Delphi round 1 was calculated using κ26 with 95% CIs, and classified as poor (κ<0.00), slight (k=0–0.20), fair (κ=0.21–0.40), moderate (κ=0.41–0.60), substantial (κ=0.61–0.80) and almost perfect (κ>0.80).27 Data from Likert scales were treated as categorical data and reported as proportions with percentages. Predictive Analysis Software Statistics for Mac (PASWV.18.0, IBM SPSS, Somers, New York, USA) was used for all the analyses.
Results
Delphi participants
Of 340 potentially eligible clinicians that were approached via email, 70 (20.5%) completed the first Delphi round and 73 (21.4%) participated in round 2. The expert panel that completed Delphi round 2 (see table 1) included medical practitioners such as pulmonologists (27.1%), internists (14.3%), family/general practitioners (11.4%), emergency physicians (7.1%), geriatricians (2.9%) and allied health providers including respiratory therapists (27.4%), physical therapists (4.1%) and primary care nurses (2.7%). Clinicians were mostly based at academic hospitals (68.1%), specialty clinics (36.2%) and the ED (23.1%). The majority of them had between 16 and 30 years of experience within their disciplines (41.2%).
Characteristics of clinician participants in Delphi study
A total of 34 patients (table 2) completed the round 1 questionnaire and 9 participated in round 2. Patients were mostly female (67.6%), older than 60 years of age (58.8%) and diagnosed with COPD in the last 10 years. Further, 70.6% of them had one or more admissions for acute exacerbation of COPD in the last year.
Characteristics of patient participants in Delphi study
Delphi results
From 29 individual care items that were presented in round 1, clinicians selected 17 COPD care items, while patients endorsed 13 COPD care items (table 3). The level of agreement between clinicians and patients in the round 1 selection of COPD items was moderate (κ=0.46; 95% CI 0.15 to 0.76). There were some discrepancies between clinicians and patients in the prioritisation of COPD care items in round 1. The COPD care items endorsed by clinicians but not by patients were (1) assess smoking status and provide counselling, (2) refer to smoking cessation programme, (3) assess need for home care, (4) refer to pulmonary rehabilitation, (5) provide recommendations about influenza vaccination and (6) administer influenza vaccine. In contrast, two COPD care items were endorsed by patients but not by clinicians: (1) provide written education about COPD, a written action plan and ongoing case management, and (2) arrange follow-up appointment with a specialist.
Delphi round 1 endorsement (%) of clinicians and patients on individual care items for inclusion in the chronic obstructive pulmonary disease (COPD) discharge bundle
In round 2, clinicians were presented with the 17 COPD care items that were selected in round 1 and retained 15 of them. Patients in round 2 were presented with the 13 COPD care items selected from round 1, of which they retained 9 (table 4). There were discrepancies between clinicians and patients in their round 2 decisions: three COPD care items were endorsed by clinicians but not by patients: (1) ensure adequate inhaler technique is demonstrated, (2) arrange follow-up appointment with family physician and (3) assess need for oxygen therapy. Care items selected by patients but not by clinicians at the end of round 2 were the same as those in round 1.
Delphi round 2 endorsement of clinicians and patients on individual care items for inclusion in the chronic obstructive pulmonary disease (COPD) discharge bundle
Nominal group meeting: participants and results
Participants in the nominal group meeting (n=44) were members of the CTS COPD Assembly (n=9), pulmonologists (n=8), researchers (n=7), health administrators (n=7), respiratory therapists (n=5), primary care physicians (n=5), emergency physicians (n=2) and geriatricians (n=1). They were presented with 18 care items selected either by clinicians or patients in Delphi round 2 (n=18).
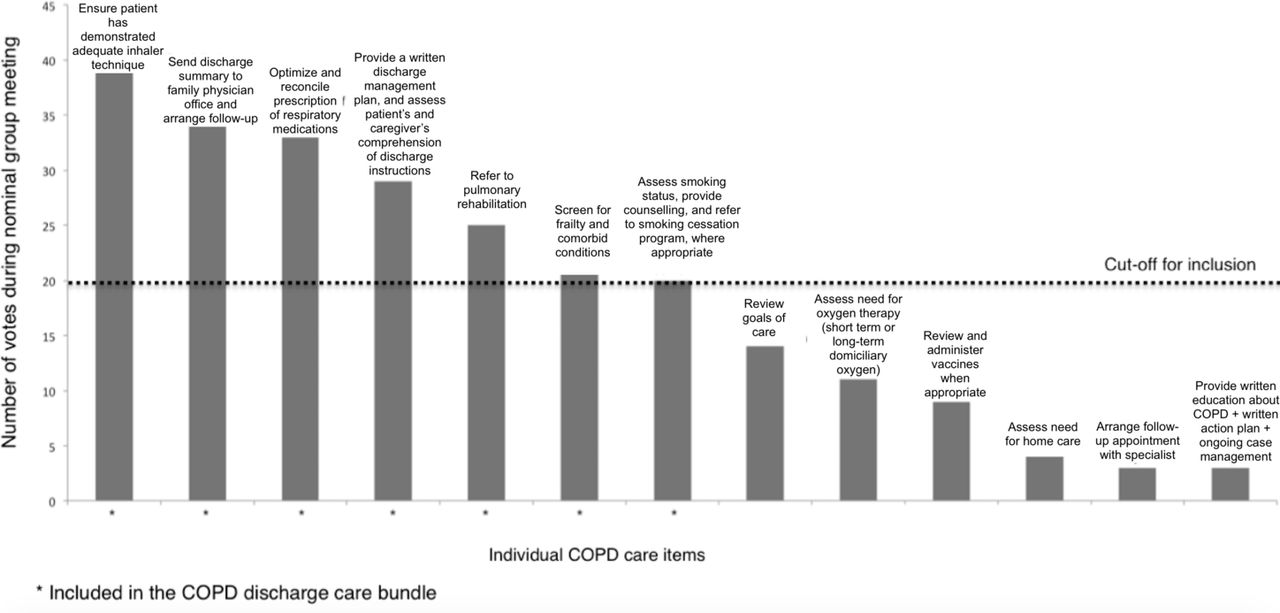
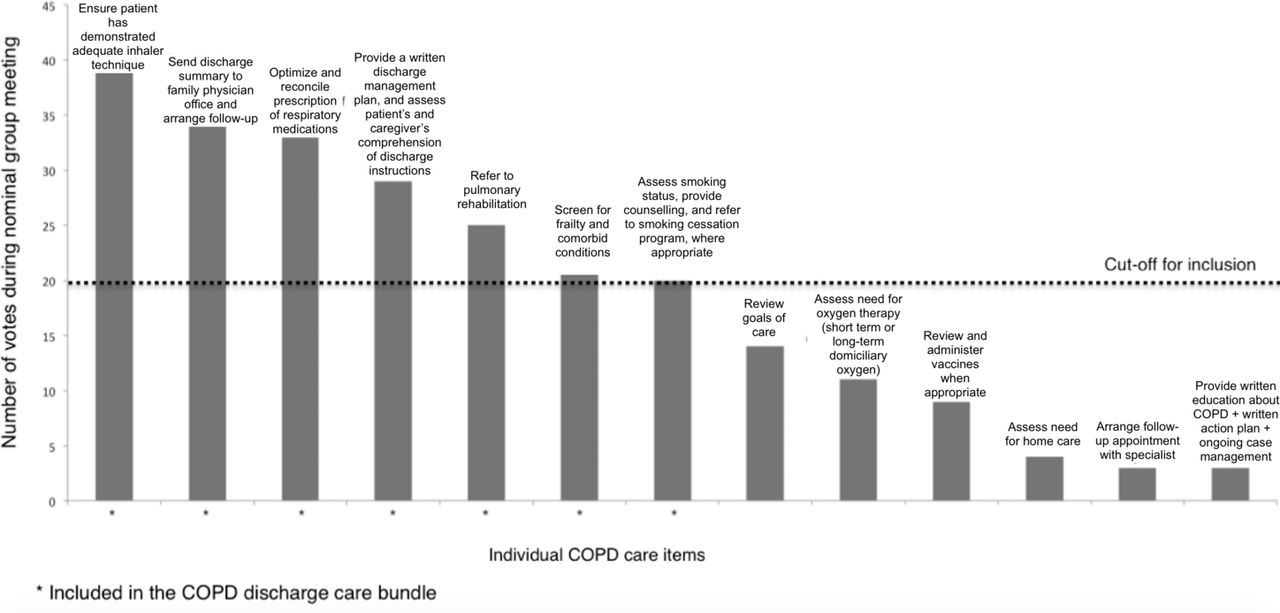
The nominal group meeting started with an interactive activity in which the content and wording of the 18 candidate care items were reviewed. Multiple statements were condensed into one care item, where possible. In this process, 12 original items were compressed into five statements. These five abridged statements were reworded to make sure the meanings were unchanged. Two new care items that were not considered in Delphi rounds were added during the nominal group meeting: (1) screening for frailty and comorbid conditions, and (2) review goals of care. This process resulted in a final list of 13 COPD care items candidate for inclusion in the discharge bundle that were dot-counted during the nominal group meeting. Meeting participants voted on the 13 care items refined during the interactive activity. Each participant had a maximum of eight votes that she/he could use to select individual COPD care items for inclusion in the discharge care bundle. During an open discussion, meeting participants agreed on the cut-off mark for inclusion at 20 votes. The nominal group reached consensus on the inclusion of seven unique care items in the COPD discharge bundle (figure 2): (1) ensure adequate inhaler technique is demonstrated; (2) send discharge summary to family physician and arrange follow-up; (3) optimise and reconcile prescription of respiratory medications; (4) provide a written discharge management plan and assess patients’ and caregivers’ comprehension of discharge instructions; (5) refer to pulmonary rehabilitation; (6) screen for frailty and comorbid conditions; and (7) assess smoking status, provide counselling and refer to smoking cessation programme.
{kind=link}
{kind=link}
Results of the nominal group voting on the inclusion of individual care items in the chronic obstructive pulmonary disease (COPD) discharge bundle.
Discussion
To our knowledge, this is the first reporting of a modified Delphi method to develop a COPD discharge care bundle informed by evidence, multidisciplinary clinical consensus and patients’ perspectives. Using a mixed-methods approach we developed a seven-item patient-centred, evidence-based and consensus-based discharge bundle for patients with acute exacerbations of COPD.
There are important variations in the number and content of individual components of COPD discharge bundles published in scientific studies.13 Our discharge bundle incorporated seven care items, a number that is aligned with recommendations about the optimal number of individual items for inclusion in care bundles.11 Others have included between 2 and 12 individual interventions, with a median number of 5 care items per bundle.13 Some care items in the COPD discharge bundle have been part of other published bundles. For example, care item #1 was part of COPD discharge bundles in 9 out of 14 studies included in the Ospina et al systematic review.13 Care items #2, #4 and #5 were included in bundles of eight studies, and care item #7 was included in seven studies evaluating other bundles. Care items #3 (three studies) and #6 (none) were less frequently included in other bundles. In contrast, educational programmes on self-management (included in nine studies) were not selected for the COPD discharge bundle.
This study is one of the few initiatives to inform the selection of individual components of COPD discharge bundles. The majority of studies in the field have not explained how individual care items were generated or selected for inclusion.13 19 This lack of detail limits the ability of readers to understand how these bundles work, how they incorporate the best available evidence and whether individual components are accepted by patients and clinicians.
Care bundles were originally developed to improve adherence to clinical practice guidelines28 and to decrease variations in care29; however, consistent uptake of recommendations from clinical practice guidelines into care bundles remains challenging.28 For example, in North America, the American College of Chest Physicians (CHEST) and the CTS have developed recommendations about both pharmacological and non-pharmacological treatments to prevent acute exacerbations of COPD (the Acute Exacerbations of Chronic Obstructive Pulmonary Disease (AECOPD) Guidelines).4 Not all AECOPD Guideline recommendations were translated into individual items in the COPD discharge bundle. Of 10 non-pharmacological recommendations in the AECOPD Guidelines,4 3 (ie, refer to pulmonary rehabilitation, having a written plan and case management for the prevention of acute exacerbations of COPD and smoking cessation counselling) were included in the COPD discharge bundle. Others (ie, administration of pneumococcal and influenza vaccines) were not included. One potential explanation for this lack of agreement is that the AECOPD Guidelines were based on a critical appraisal of the evidence supporting individual actions for preventing acute exacerbations of COPD,4 whereas selection of care items in the COPD discharge bundle was based on evidence supporting bundles as a sum of individual components, plus clinician consensus and patients’ perspectives on their relative importance. Alignment with clinical practice guidelines and feasibility of local adaptations of the COPD discharge bundle should be further explored to ensure wide applicability.
Strengths and limitations
The Delphi procedure is a valid method to determining consensus for clinical improvement practices in healthcare settings.30 The number of experts (both clinicians and patients) who participated in both the Delphi and nominal group phases of the study surpassed the sample size recommended for content validation (ie, 5–10 experts)31 of the COPD discharge care bundle. They represent multidisciplinary professional groups that directly influence patient care and the development of clinical practice guidelines. An important strength of this study was the participation of the CTS COPD Assembly and different types of clinicians, including primary care physicians who are instrumental in the integration of acute and chronic care of patients with COPD after discharge. This is key from a knowledge translation perspective. Also, incorporating the perspectives of patients with COPD is an important strength in the development of a patient-centred bundle that is more likely to lead to treatment adherence and better outcomes.32 Lastly, the COPD care bundle represents a balance between pragmatism and completeness. The total number of items is not evidence-based, but the seven items identified in this study represent a consensus of what is possible, feasible and valid in practice.
This study has some limitations. Because clinician and patient samples were selected using non-random procedures (ie, purposeful and convenience sampling, respectively), representativeness, in a statistical sense, was not assured. Clinicians were predominantly experts from large, urban, academic hospitals, thereby limiting generalisation of results to rural, non-academic settings. The importance given to individual care items may vary according to local criteria and their availability in the settings from which the clinicians practice. Similarly, patients in the Delphi study may not fully represent those with very severe COPD that are more likely to have frequent admissions for acute exacerbations of COPD and require implementation of the discharge care bundle more often.
This Delphi study was conducted in Canada, a country with a publicly funded universal healthcare system. The selection of individual care items for a COPD discharge care bundle in countries with other health insurance models may differ as financial and insurance barriers often impede access to some individual COPD care items considered such as access to pulmonary rehabilitation services and appropriate inhaler medication. Therefore, generalisability of the COPD discharge bundle to other health systems may be limited. Local adaptations of the bundle should be evaluated prior to implementation in health systems supported by other financial and insurance arrangements. Adjustments in the content of COPD discharge bundles can be guided by consideration of system-level failures and unmet patient needs.33
An aspect that should be explored in future studies is whether individual components are perceived as more important for bundle effectiveness than the sum of all components. Some may argue that the strength of a COPD discharge bundle is that all individual interventions should be implemented in every eligible patient with COPD under a ‘all-or-none’ approach.34 Others have questioned whether a ‘one-size-fits-all’ model is appropriate for discharge bundles that are meant to be implemented for the spectrum of patients with COPD and the diverse settings where they receive care.19
The work presented here is the second step of a multistage process aimed at evaluating the implementation and effectiveness of an evidence-based, patient-oriented discharge care bundle for patients with COPD. The first step was a systematic review of the scientific literature13 that provided the evidence base for the discharge bundle development. Since the completion of the Delphi study, the research team engaged in the design and planning of a multicentre trial (www.clinicaltrials.gov; study ID: NCT03358771) to evaluate the implementation and effectiveness of the COPD discharge bundle. Enrolment in the trial is expected to conclude in 2019, with the goal to obtain sufficient data for reliable estimates of the treatment effect for clinical decision-making.
Conclusions
This study proposes a patient-centred, evidence-based and consensus-based discharge care bundle for patients with acute exacerbations of COPD. The goal is that the discharge care bundle will ensure that patients with COPD are managed appropriately, effectively and in ways that are acceptable for them. This COPD discharge bundle provides a foundation for further research and critical evaluation of barriers and facilitators for implementation, implementation fidelity and effectiveness in healthcare settings.
Acknowledgments
none
References
Footnotes
Contributors MBO, RL, BHR, MB and MKS contributed to study conception and protocol development. MO, MM, LD, MB, RL, BHR and MKS contributed to study design and coordination of Delphi and nominal group phases. MBO performed the statistical analysis and drafted the paper. All authors provided critical revisions and contributed to editing of the paper for important intellectual content. MKS had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The study was funded by Alberta Innovates Health Solutions Partnership for Research and Innovation in the Health System Program; (AIHS PRIHS 201400390); Alberta Health Services.
Competing interests BHR’s research is supported by a Tier I Canada Research Chair in Evidence-based Emergency Medicine from the Canadian Institutes of Health Research (CIHR) through the Government of Canada.
Ethics approval University of Alberta Health Research Ethics Board (PRO00055500).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from this work would be provided for those interested.
Collaborators Writing Committee Members for the COPD PRIHS-2 Group: Ron Damant (University of Alberta), Irvin Mayers (University of Alberta), Jerry Hall (Royal Alexandra Hospital), Lee Green (University of Alberta), Charles Yan (Institute of Health Economics), Sachin Pendharkar (University of Calgary), Chris Mody (University of Calgary), Stephen Field (University of Calgary), Brandie Walker (University of Calgary), Tara Lohman (University of Calgary), Michael Roman (University of Calgary), Jim Graham (Alberta Health Services), Peter Farris (Alberta Health Services), Allan Ryan (Alberta Health Services), Kelly Mrklas (Alberta Health Services), Roberta Dubois (Alberta Health Services).
Presented at Poster presentation at (1) American Thoracic Society 2016 International Conference; 13-18 May 2016; San Francisco, California (USA); and (2) Canadian Respiratory Conference 2016; 14-16 April 2016; Halifax, Nova Scotia (Canada).