Article Text

Abstract
Objectives: Little is known about the potential health effects of the coarse fraction of ambient particles. The aim of this study is to estimate the links between fine (PM2.5) and coarse particle (PM2.5−10) levels and cardiorespiratory hospitalisations in six French cities during 2000–2003.
Methods: Data on the daily numbers of hospitalisations for respiratory, cardiovascular, cardiac and ischaemic heart diseases were collected. Associations between exposure indicators and hospitalisations were estimated in each city using a Poisson regression model, controlling for confounding factors (seasons, days of the week, holidays, influenza epidemics, pollen counts, temperature) and temporal trends. City-specific findings were combined to obtain excess relative risks (ERRs) associated with a 10 μg/m3 increase in PM2.5 and PM2.5−10 levels.
Results: We found positive associations between indicators of particulate pollution and hospitalisations for respiratory infection, with an ERR of 4.4% (95% CI 0.9 to 8.0) for PM2.5−10 and 2.5% (95% CI 0.1 to 4.8) for PM2.5. Concerning respiratory diseases, no association was observed with PM2.5, whereas positive trends were found with PM2.5−10, with a significant association for the 0–14-year-old age group (ERR 6.2%, 95% CI 0.4 to 12.3). Concerning cardiovascular diseases, positive associations were observed between PM2.5 levels and each indicator, although some did not reach significance; trends with PM2.5−10 were weaker and non-significant except for ischaemic heart disease in the elderly (ERR 6.4%, 95% CI 1.6 to 11.4).
Conclusions: In accordance with other studies, our results indicate that the coarse fraction may have a stronger effect than the fine fraction on some morbidity endpoints, especially respiratory diseases.
Statistics from Altmetric.com
The association between particulate air pollution and cardiorespiratory hospitalisations has been reported in many epidemiological studies over the past decade.1 2 However, most of the reports have focused on particles with an aerodynamic diameter of <10 μm (PM10) or <2.5 μm (PM2.5). Fewer studies have examined the potential health effects of the coarse fraction, that is, particles ranging in size from 2.5 to 10 μm (PM2.5−10).3 On the one hand, it is widely accepted that smaller particles offer a larger surface area and hence potentially larger concentrations of adsorbed or condensed toxic air pollutants per unit mass. Hence PM2.5 were taken to be more relevant as an exposure indicator than larger particles.4 On the other hand, the physiopathological mechanisms of particles on human health are not fully understood. Moreover, particles size is associated with different chemical, biological and physical properties that may contribute to specific physiopathological mechanisms. Coarse particles originate mainly from the soil and abrasive mechanical processes, and thus may also carry biological materials such as bacteria, moulds or pollens, and are therefore likely to produce adverse health effects.5 6 However, coarse particles do not penetrate as deeply into the respiratory tract as fine particles and so are more likely to affect the upper respiratory tract.7
Regarding the relative sizes of the health effects associated with fine and coarse particles, results from epidemiological studies are inconsistent. In some studies, especially when respiratory health effects are considered, coarse particles are associated with larger risk estimates than fine particles,8 9 but other results suggest a stronger effect of fine particles.10 11 Better knowledge of the health risks associated with exposure to fine and coarse particles, therefore, is still needed as suggested in a recent review on this topic.3 The present study aims to analyse the associations between both coarse and fine particle levels and hospital admissions for cardiorespiratory diseases in six French cities for the general population and for child (0–14 years old) and elderly (⩾65 years of age) subgroups.
METHODS
Study population and period
This study was conducted in six French urban areas which were representative of the diversity of geographical locations in France and large enough to generate daily numbers of hospitalisations suitable for statistical analysis: Le Havre, Lille, Marseille, Paris, Rouen and Toulouse. Study areas included the main city and bordering cities where urbanisation and background air pollutants levels were considered to be homogeneous. The length of the study period ranged from 31 to 48 months, between 2000 and 2003, depending on the city.
Pollution exposure estimates
Local air pollution monitoring networks provided data on the levels of PM10 and PM2.5 which were measured continuously by background monitoring stations using TEOM (tapered element oscillating microbalance) analysers. Background monitoring stations measuring both PM2.5 and PM10 levels (one in Toulouse, four in Paris and two in all other cities) were utilised because they are not directly influenced by occasional sources of pollution, as they are located some distance from major roads and industries. The maximal distance between residential addresses and monitoring stations was 20 km, and all study areas were homogeneous regarding urbanisation and background air pollution levels according to local air quality monitoring experts. For each study area, temporal variations in the concentrations of pollutants measured by selected stations could therefore be considered as a good proxy of temporal variations in population exposure.
For each monitoring station, daily mean levels (in μg/m3) were calculated if at least 75% of hourly values were available, otherwise the data were considered as missing. The mass concentration of the coarse fraction (PM2.5−10) was calculated by subtracting PM2.5 levels from PM10 levels. The correlation of PM2.5, and PM2.5−10 levels between the different monitoring stations of each study area was checked (correlation coefficient >0.6), as well as the closeness of levels from one monitoring station to another (overlapping interquartile range). Exposure indicators were then calculated as the arithmetic mean of the daily mean concentrations of PM2.5 and PM2.5−10 measured by the different monitoring stations.
Hospitalisation data
The daily numbers of cardiorespiratory admissions to public and major private hospitals located within each study area were extracted from the French hospital information system (PMSI) using ad hoc software. These data were obtained for people living within each of the study areas. To approximate the diagnosis at the time of hospitalisation, stays were selected according to the main discharge diagnosis (ICD-10) coded in the first unit to which the patient was admitted.
The following health indicators were built: daily numbers of hospitalisations for cardiovascular (ICD-10: I00–I99), cardiac (I00–I52) and ischaemic heart diseases (I20–I25), all respiratory diseases (J00–J99) and respiratory infection (J10–22).
As the PMSI does not allow emergency hospital admissions to be distinguished from scheduled admissions (which cannot be related to short-term changes in air pollution levels), stays in outpatient units as well as stays following a transfer from another hospital were excluded.
Potential confounding factors
Temperature data were obtained from the national meteorological institute (Météo-France). Holiday dates were obtained from the Ministry of Education. The dates of influenza epidemics were obtained from the French communicable diseases computerised surveillance network (GPs network), except in Paris where dates for local epidemics were obtained from the regional group for influenza surveillance (GROG). Pollen daily counts monitored by a Hirst-type impact volumetric sampler in each city were obtained from the French national network of aerobiological surveillance (RNSA).
Statistical analysis
The daily data from the six cities were analysed with time-series methods, using mono-pollutant generalised additive Poisson regression models allowing for overdispersion.12 PM2.5 and PM2.5−10 were included in the models as a linear term of the mean level during the current day and the previous day (0–1-day lag). Possible confounders, including long-term trend, seasonality, days of the week, holidays, influenza epidemics, pollen counts, minimum temperature of the current day and maximum temperature of the previous day, were controlled using APHEA-2 methodology.13 Long-term trend and seasonality were modelled using a penalised regression spline of time. A large set of basis functions (equal to 50 per year) was used, and smoothing was used to remove autocorrelation of the model’s residuals (by minimising the absolute value of the sum of the partial autocorrelation function of the model’s residuals).14 Dummy variables for days of the week and holidays were included as other independent variables. A dummy variable for the months of July and August allowed the fact that many hospital units are closed during this period to be taken into account. Temperature and influenza terms were modelled using natural splines with 3 degrees of freedom for each. Both minimal and maximal temperatures were taken into account because the combination of these two parameters could be associated with health effects rather than an extreme minimal or maximal temperature alone.15 Furthermore, inclusion in the model of non-linear functions of current and previous day temperatures are a classic way of adjusting for confounding in such time-series analysis,16 17 and combined estimates of air pollution related relative risks have been shown to be robust to model specification to weather confounding.18 Autoregressive terms were added if serial correlations remained in the residuals of the final models. City-specific results were then combined using a random effects model following DerSimonian and Laird’s methodology.19 All analyses were performed using the MGCV package in R software (R 2.1.1).20
For cardiovascular diseases, analyses were performed for the whole dataset (all ages) and were then repeated while restricted to elderly people (⩾65 years of age). For all respiratory diseases, analyses were conducted for the following age groups: 0–14 years, 15–64 years and ⩾65 years. For respiratory infections, analyses were performed for the whole data set (all ages) because of the small daily numbers of hospitalisations for these diseases in some of the participating cities.
All results are presented as the excess relative risk (ERR 100(RR–1)), in percentage, which expresses the increase in the relative risk (RR) associated with:
-
a 10 μg/m3 increase in particle level and
-
an increase in pollutant levels corresponding to the difference between the lowest of the 5th percentiles and the highest of the 95th percentiles of the cities’ distribution.
The choice of a fixed and a relative increase in air pollutant levels allows comparison of the ERRs associated with the particulate air pollution indicators studied here for a fixed increase while taking into account the levels of these indicators encountered across time and cities.
RESULTS
The six cities have a total population of nearly 10 million, including 6 million in the Paris metropolitan area, with a large diversity of climate and air pollution levels and sources. For each city, detailed information was collected on 49–84% of the total number of respiratory hospital admissions and on 52–76% of the total number of cardiovascular hospital admissions within the study area, depending on the availability of data (table 1).
The daily mean numbers of respiratory and cardiovascular hospitalisations varied according to the size of the city and ranged from 1.1 to 22.5, and from 2.5 to 91.9, respectively (table 1).
Over the study period, missing data for PM levels ranged from 1.1% to 7.6% according to city. Mean levels of PM2.5 and PM2.5−10 showed low variability across the cities: mean levels of PM2.5 ranged from 13.8 to 18.8 μg/m3 and mean levels of PM2.5−10 ranged from 7.0 to 11 μg/m3 (table 2).
PM2.5 represented about two thirds of the PM10 mass (fig 1). The correlation coefficient between PM2.5 and PM2.5−10 levels differed across cities, ranging from 0.28 to 0.73.

Concerning hospitalisations for all respiratory diseases, positive although non-significant combined ERRs were observed in association with a 10 μg/m3 increase in PM2.5 levels, irrespective of the age group (0.4% for 0–14 years, 0.8% for 15–64 years and 0.5% for ⩾65 years) (table 3). For the same increase in PM2.5−10 levels, higher ERRs of hospitalisations for respiratory diseases were observed, and a significant association was observed in the 0–14-year-old age group (ERR 6.2%, 95% CI 0.4 to 12.3). ERRs for this age group were positive in all participating cities (fig 2).

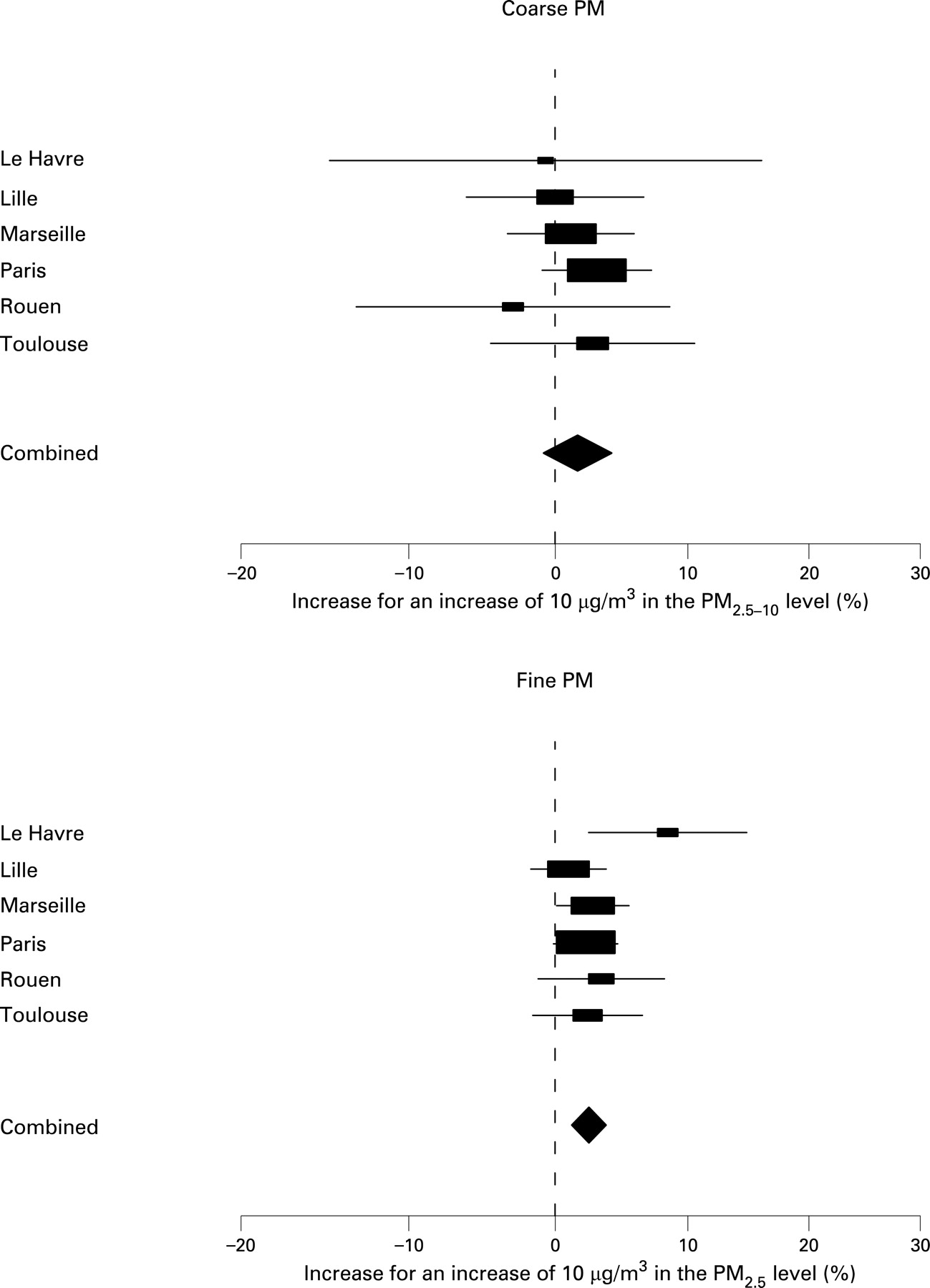
When hospitalisations for respiratory infections were considered, combined ERRs associated with a 10 μg/m3 increase in levels of PM2.5 or PM2.5−10 were both positive and significant. The central estimate for PM2.5−10 (ERR 4.4%, 95% CI 0.9 to 8.0) was higher for PM2.5 (ERR 2.5%, 95% CI 0.1 to 4.8) (table 3). Local ERRs ranged from −2.9% to 6.9% for PM2.5 and from −2.8% to 18.6% for PM2.5−10.
Regarding hospitalisations for cardiovascular diseases, we observed positive associations between hospitalisations and PM2.5 levels. However, combined ERRs of hospitalisation associated with a 10 μg/m3 increase in PM2.5 levels in the general population (all ages) were not significant, except for all cardiovascular diseases (ERR 0.9%, 95% CI 0.1 to 1.8) (table 3). When the analysis was restricted to the elderly (⩾65 years of age), we found higher and significant combined ERRs for cardiovascular diseases as a whole and for the other two subgroups of cardiac diseases. Central estimates increased with the specificity of the causes of hospital admissions taken into account, ERR 1.9% (95% CI 0.9 to 3.0), ERR 2.4% (95% CI 1.2 to 3.7) and ERR 4.5% (95% CI 2.3 to 6.8) for cardiovascular, cardiac and ischaemic heart diseases, respectively. Local ERRs of hospitalisation for cardiovascular diseases in the elderly ranged from 1.0% to 8.4% for PM2.5 and from −3.0% to 2.7% for PM2.5−10 (fig 3).

{kind=link}
{kind=link}
{kind=link}
Compared to ERRs associated with an increase in PM2.5 levels, ERRs of cardiovascular hospitalisation associated with the same increase in PM2.5−10 levels were weaker and non-significant except for ischaemic heart diseases in the elderly (ERR 6.4%, 95% CI 1.6 to 11.4).
When comparing ERRs obtained for an increase in the pollutant levels corresponding to the difference between the lowest of the 5th percentiles and the highest of the 95th percentiles of the cities’ distribution, the same differences between PM2.5 and PM2.5−10 can be observed except for ischaemic heart disease. The ERR associated with such an increase in PM2.5 levels (ERR 12.7%, 95% CI 6.3 to 19.5) was then comparable to that associated with a similar increase in PM2.5−10 levels (ERR 12.4%, 95% CI 3.1 to 22.6) (table 3).
DISCUSSION
This study is one of the few that have investigated the association between fine and coarse particles and cardiorespiratory hospitalisations, and is the first European multicentric study on this topic. It was conducted in six geographically and climatically diverse French cities with various air pollution levels and sources.
We found significant relationships between indicators of exposure to fine and coarse particles and several indicators of hospital admissions. The highest significant excess risks in the present study were observed for children (<15 years old, 6.2% ERR of hospitalisation for respiratory diseases in association with a 10 μg/m3 increase in PM2.5−10) and for the elderly (6.4% ERR of hospitalisation for ischaemic heart diseases in association with the same increase in PM2.5−10). For the same particulate air pollution indicator, the results differed according to the health indicator and the age group considered. These results support the robustness of our analysis: ERRs increased with the specificity of health indicators and were higher in children and the elderly. They favour the hypothesis that exposure to ambient air pollution is more likely to cause or exacerbate cardiorespiratory diseases in vulnerable populations such as children or the elderly. The higher excess of relative risk of respiratory diseases associated with an increase in coarse particles that we found in children compared to other age groups is suggested by the literature. Indeed, studies modelling age-related particle deposition in humans indicate that tracheobronchial and pulmonary deposition fractions are greatest for infants and decrease with age,21 which is why children may be at a greater health risk from exposure to airborne particulate matter and noxious materials. Such a difference was not observed for fine particles (for which no significant excess of relative risk was found whatever the age group considered), and this result needs to be further explored since our study is the first to investigate the effect of fine and coarse particles on respiratory diseases in children.
Although the range of daily levels observed for the two pollutants is different, our results suggest that, even while taking into account such differences (table 3), the coarse fraction may have a stronger effect on respiratory morbidity than the fine, whereas fine particles may be more associated with some cardiovascular outcomes. It was not possible to examine the joint effects of coarse and fine particles in a two-pollutant model given their high correlation levels (table 2).
These results are consistent with previous epidemiological studies. Indeed, among the few other studies that investigated both PM2.5 and PM2.5−10 effects on cardiorespiratory morbidity, several suggested that the coarse fraction could have a greater effect than the fine fraction. In a Canadian study, levels of fine and coarse particles were both significantly associated with the risk of acute hospitalisations for cardiorespiratory diseases, but the excess risk was higher for the coarse fraction than for the fine fraction,22 which is in accordance with our results on respiratory diseases. Similar results were found in Detroit, Michigan, with more specific indicators of respiratory admissions (pneumonia and COPD) in the elderly.23 In a study from Chile on respiratory emergency visits in children aged <15 years,24 results were quite inconsistent according to diagnoses and seasons, but coarse particles seemed to have a higher effect than fine particles in the warm season. In the present study, the difference between fine and coarse particles was also particularly obvious in children, as noted previously.
As regards cardiovascular morbidity, in a study concerning older subjects suffering from coronary artery disease, high levels of ambient coarse particles adversely affected heart rate variability, whereas no clear association was found with PM2.5.25 However, other epidemiological studies did not find any significant difference between the two fractions of particles and their effects on morbidity.26–28 Concerning mortality, most studies conducted on the effects of various fractions of PM found a higher effect of fine particles, even though some of those studies also showed some effects of coarse particles.3 The only other European study which investigated the effects of fine and coarse particles also failed to discern clear differences between the two fractions,10 but suggested that the active component resided mostly in the fine fraction, even if effects of the coarse fraction could not be excluded. Results from the literature are therefore quite heterogeneous, but most studies either conclude that the coarse fraction may be a more important predictor of cardiorespiratory morbidity, or at least cannot exclude an effect. In a review of the health effects of fine particles,29 Englert suggested that the relative sizes of the effects attributed to fractions of PM10 depended on their relative contributions, in terms of mass concentration, suggesting that the fraction which had the higher contribution had the higher effect. The author concluded that, considering that the contribution of PM2.5−10 to PM10 was rather low, the probability of finding significant associations with coarse particles was also expected to be low. However, in the present study, coarse particles represented about a third of PM10 mass concentration in every city, but higher ERRs were observed in association with coarse particles levels for several health indicators, which really suggests a specific effect of this fraction.
A possible explanation for such specific effects of the coarse and the fine fraction of PM is their differences in size and chemical composition which are likely to result in different types of diseases and severity of effects. PM adverse effects on the function of the respiratory system, the blood vessels and the heart have been demonstrated through toxicological studies in humans and animals.30 However, only in recent years have investigators begun to separately address the health effects of coarse particles, firstly because coarse particles were initially considered as potentially less toxic than fine particles due to their large size and small surface area to mass ratio and secondly because it is only recently that PM2.5 particles have been measured separately. However, many arguments indicate that both the fine and coarse particles have a potentially toxic role. First, particle agglomerates that are large enough to be in the coarse fraction may contain many ultrafine particles and other attached constituents. Furthermore, results from toxicological studies showed that on an equal mass basis, coarse and fine particles both produce pulmonary inflammation.31 32 Other studies even showed a stronger effect for the coarse fraction and a lack of effect for ultrafine particles.33 34 Some authors have investigated whether some specific constituents could explain these differences of effects between the two fractions.7 35 36 Since pollen counts were included as possible confounding factors, pollens that could be contained in the coarse fraction cannot explain the differences observed in the present study. However, according to various reports, endotoxin on coarse particles could account for their ability to induce adverse health effects36 37; moreover, inhalation of low levels of endotoxins could be responsible for airway diseases.38
Oxidative stress, which can lead to both cardiovascular and respiratory damage, could also be induced by coarse as well as fine particles.31 32 Studies which focused on oxidative stress in blood cells suggest that although haemolytic potential was greater for fine particles than for coarse particles in equal mass concentration, the two fractions did not show any significant haemolytic differences when data were expressed in terms of PM surface per volume unit of suspension.35
Given these considerations, the higher effects of coarse particles on some cardiorespiratory endpoints that we observed in our study are not surprising. Indeed, their toxicological potential could enhance morbidity leading to increases in cardiorespiratory hospitalisations.
As regards the methods, all the data used in our multicentric study were collected through a standardised protocol. Hospitalisation data were obtained from the French hospital information system (PMSI) which was not initially created for an epidemiological but for a medico-economic purpose. Diagnoses coded in the PMSI database are known to be subject to some degree of misclassification, especially for respiratory and cardiovascular diseases, which are often associated with frail patients such as elderly individuals with multiple pathologies. However, this should not introduce a directional bias in our daily time-series analyses since patterns of diagnosis misclassification are not a priori temporally associated with variations in air pollutant levels. Scheduled hospitalisations, which are not related to air pollution levels, could not be distinguished from emergency admissions, and this may have limited the specificity of our indicators; however, we were able to exclude stays in outpatient units and admissions following a transfer from another hospital. Residual misclassification due to the inclusion of scheduled admissions could not be evaluated. However, this may effect the precision of our results but not estimations of ERRs, since scheduled admissions are not related to temporal variations in particulate air pollution levels. Hospitalisation data were not exhaustive because we could not obtain data from all of the hospitals in the study areas. This could have induced a selection bias since most of the hospitals which were not included were private facilities, and it is known that people with a low socioeconomic level have recourse to public rather than private hospitals. However, this bias does not vary across time and therefore should not affect the results obtained in a time-series analysis such as the present one.
One of the issues often raised concerning the time-series analyses used in the present study is the inadequate control of seasonality. However, other methods available up to now (eg, case cross-over analyses) do not allow this limitation to be overcome.39 Furthermore, time-series analyses allow controlling for over-dispersion, which is particularly important for data such as those analysed in the present study, while case-crossover analyses typically do not.40 As others,41 given that no data on confounding factors were available at the individual level, we therefore thought that the choice of time-series analysis was more appropriate. The decision to use the average levels of lags 0 and 1 systematically, based on previous evidence,42 could have introduced an underestimation of the relationships observed,43 but avoids a potential bias resulting from multiple testing and selectively reporting the most significant results.44 All temporal confounding factors known to be associated with both air pollution and morbidity were taken into account in our models, and we also controlled for influenza epidemics which can be linked with cardiovascular diseases through pro-inflammatory and pro-thrombotic effects.45
Indicators of particulate air pollution exposure were based on measurements from background monitoring stations, which were all located in relation to air pollution sources in accordance with national guidelines. These stations were selected with the advice of local experts who considered them to be representative of the population’s exposure within each study area.
In conclusion, in view of our findings and the results of other studies, it appears that both fine and coarse PM fractions are able to elicit adverse health effects. The coarse fraction may play an important role in certain aspects of morbidity, particularly in children, and therefore should not be ignored, even if further studies are needed to obtain valid and robust exposure-response functions. However, there is sufficient concern about the health effects of coarse particles to suggest that they should be taken into account in the various plans and actions aimed at reducing air pollution health effects.
Main messages
-
Although further studies are needed to better understand the specific physiopathological mechanisms of coarse particles, both fine and coarse PM fractions seem able to elicit adverse health effects.
-
These effects can be observed even in cities where levels are very close to European air quality guidelines.
Policy implications
-
Both fractions should be considered as relevant air quality indicators and the effects of the coarse fraction should not be overlooked.
Policy makers should try to reduce pollutant emissions and guidelines since current levels are linked to a short-term increase in morbidity.
REFERENCES
Footnotes
-
Competing interests: None.