Article Text

Abstract
Acute respiratory distress syndrome (ARDS) related to SARS-CoV-2 infection has some unusual characteristics that differentiate it from the pathophysiology described in the more ‘typical’ ARDS. Among multiple hypotheses, a close similarity has been suggested between COVID-19 ARDS and neonatal respiratory distress syndrome (RDS). With this opinion paper, we investigated the pathophysiological similarities between infant respiratory diseases (RDS and direct neonatal ARDS (NARDS)) and COVID-19 in adults. We also analysed, for the first time, similarities in the response to exogenous surfactant administration in terms of improved static compliance in RDS and direct NARDS, and adult COVID-19 ARDS. In conclusion, we believe that if the pathological processes are similar both from the pathophysiological point of view and from the response in respiratory mechanics to a recruitment treatment such as surfactant, perhaps the latter could be considered a plausible option and lead to recruitment in clinical trials currently ongoing on patients with COVID-19.
- COVID-19
- ARDS
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
The COVID-19 pandemic has been characterised by many hospitalisations and, to date, over two million deaths worldwide. Critically ill patients with COVID-19 may develop incremental respiratory compromise leading to acute respiratory distress syndrome (ARDS). However, ARDS related to SARS-CoV-2 infection has some unusual features, which differentiate it from the pathophysiology described in more ‘typical’ ARDS, as defined by the BERLIN criteria.1 Among the multiple pathophysiological hypotheses relating to the development and progression of this ‘atypical’ form of ARDS, a close similarity between COVID-19 ARDS and neonatal respiratory distress syndrome (RDS) has been suggested in the early phases of ARDS in critically ill patients.2 This concept has raised questions about whether the similarities in the pathophysiology of RDS and COVID-19 ARDS favours trials of lung surfactant therapy in the management of COVID-19 ARDS, at the time of writing seven randomised controlled trials (RCTs) ongoing in this setting.
Acute lung injury in SARS-CoV-2 infection appears to result, at least partly, from the host-driven exaggerated inflammatory response. Furthermore, the so-called ‘cytokine storm’ alongside intravascular coagulation generates microthrombi of the pulmonary vessels. This process can lead to ARDS development and subsequently interfere with the pulmonary repair mechanisms, thus predisposing individuals to fibrosis.3 However, the pathophysiology of COVID-19-induced lung damage cannot be limited to the inflammatory hypothesis alone. Indeed, a recent exploratory study suggested that the hyperinflammatory phenotype is less prevalent, although more severe, in patients with COVID-19 than in previous non-COVID-19 cohorts.4
Whichever cascade phenomena contribute to progressive lung damage, the initial trigger is the infection of the host’s respiratory cells by the SARS-CoV-2 virus. In this host–virus interaction, a key role of the ACE2 is recognised.5 At the same time, recent gene-ontology studies have shown that 83% of lung cell expression of the ACE2 gene is on alveolar type 2 (AT2) cells.5 These findings explain the extensive cytopathic viral effect on AT2 in the lower respiratory tract seen in pathological studies.6 This progressive damage of AT2 limits surfactant production. It will predispose to the formation of atelectasis, inflammation and damage of the alveolar-capillary barrier with interstitial oedema and subsequent thrombosis of the lung capillary bed.7 This mechanism is similar to that observed in neonatal RDS.
Neonatal RDS, previously also referred to as hyaline membrane disease, is largely secondary to the immaturity of the alveolar epithelium, causing surfactant deficiency in the immature preterm lung.8 It is widely accepted that increased surface tension in the lungs of preterm infants is primarily responsible for the hypoxia and atelectasis, characteristic features of neonatal RDS, which has proven responsive to exogenous surfactant therapy.9 Over the last decade, the management of preterm infants with neonatal RDS has changed due to the move toward using early continuous positive pressure ventilation and keeping exogenous surfactant therapy as a rescue remedy if the infant does not improve.10 11
Interestingly, initial thoughts concerning the causation of neonatal RDS had focused on concepts of pulmonary vascular pathology leading to hypoperfusion12 and activation of the coagulation cascade.13 As in RDS, these microthrombotic phenomena are also described in adults with SARS-CoV-2 infection, generating pulmonary hypoperfusion in COVID-19 lung disease. Microvascular coagulation disorders in neonatal RDS were not responsive to fibrinolytic therapy.14 Similarly, in COVID-19 lung disease, preliminary results of therapeutic intravenous unfractionated heparin do not seem to improve outcome15, despite this treatment is still under extensive investigation by ongoing RCTs.16 17
As stated above, preterm infants with neonatal RDS demonstrate high alveolar surface tension and low compliance of the respiratory system18 (Crs). In clinical practice, administration of surfactant either as prophylaxis or rescue rapidly results in the lung being able to expand, with Crs improvement and consequent low ventilatory pressures needed to generate tidal volume.9 10 19 The clinical presentation (table 1) in critically ill patients with COVID-19 lung disease is reminiscent of the preterm infant with RDS. Clinical symptoms of respiratory distress and severe hypoxia are described in both these patient groups. Furthermore, the histology is also similar because they both demonstrate alveolar infiltration, hyaline membranes and oedema.11 Moreover, the use of corticosteroids seems to be effective in both scenarios, antenatal administration for neonatal RDS8 and during acute respiratory failure under oxygen delivery in COVID-1920 (table 1).
Clinical features, histological features, Crs and steroid treatment seen in preterm infants and observed in patients with COVID-19 ARDS and as reported by Grasselli et al.3 See text for details
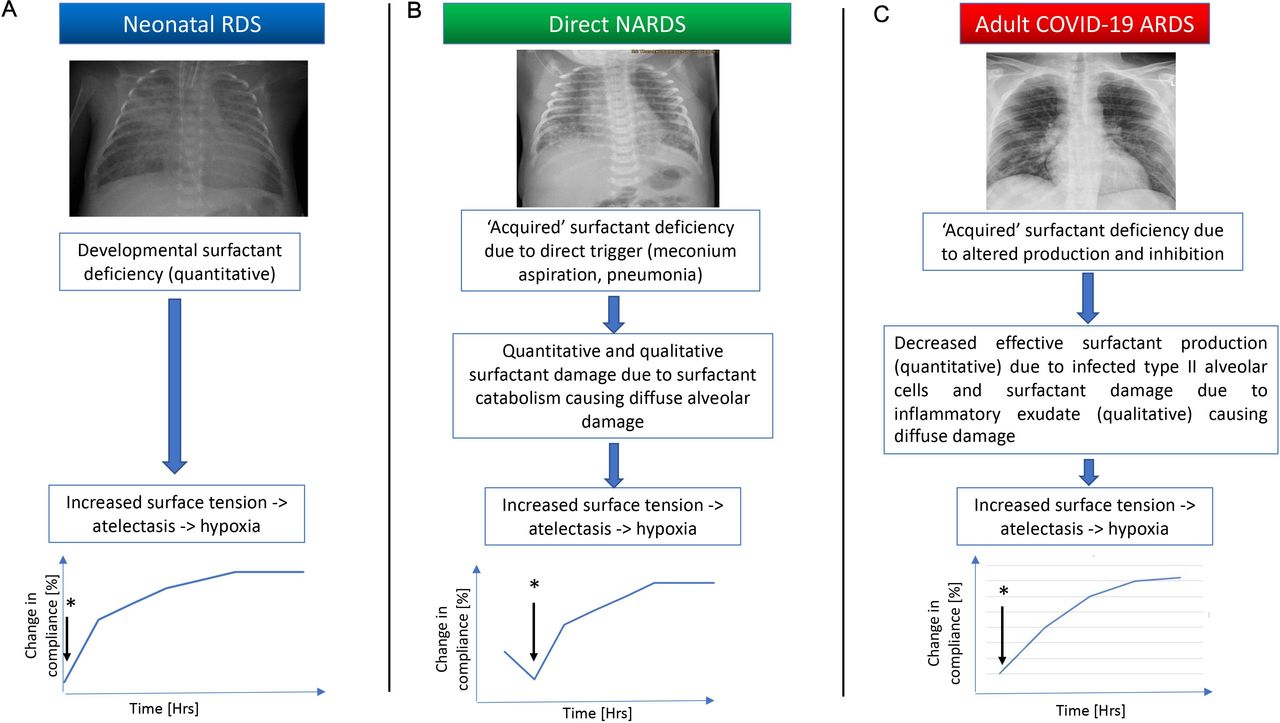
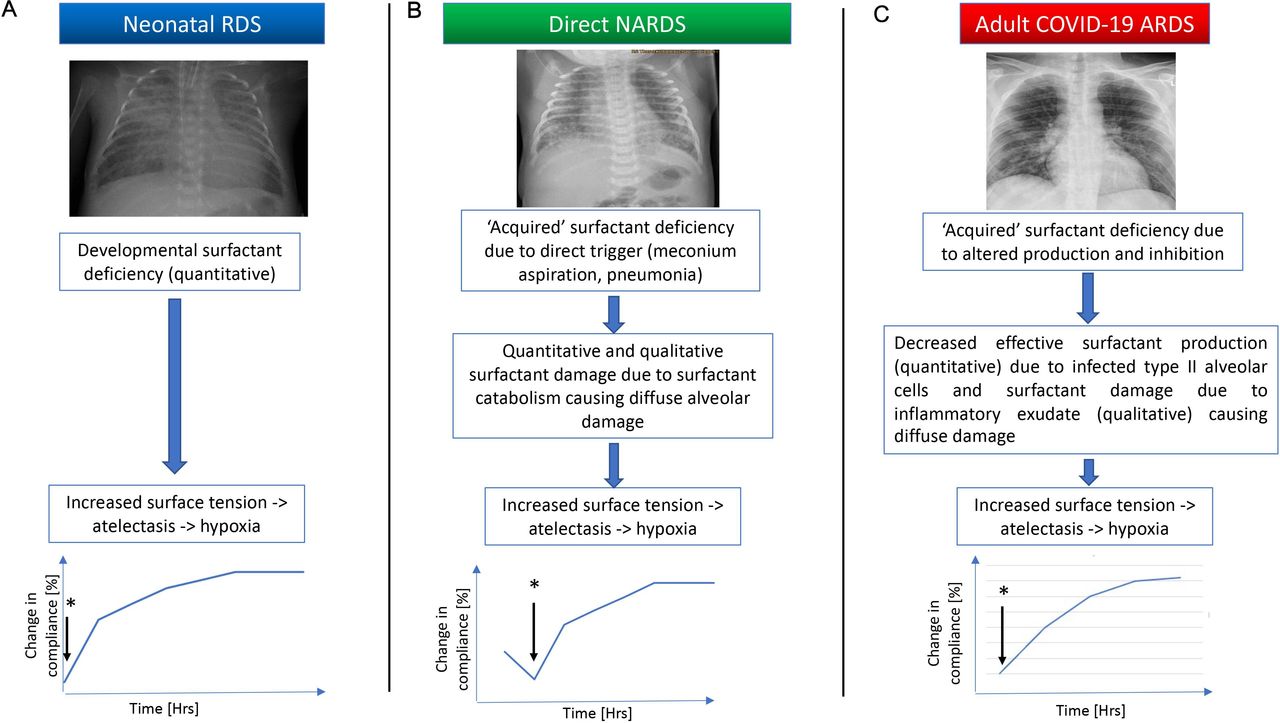
Although this paper mainly focuses on neonatal RDS, it is pertinent to mention that there is another group of infants with respiratory failure that could maybe resemble COVID-19 ARDS, infants with neonatal ARDS (NARDS). The damage related to the endogenous surfactant in this newborn respiratory disease is both quantitative and qualitative accordingly with what happens in the adult with COVID-19 ARDS (figure 1). The Montreux definition of NARDS21 highlighted the need for recognition of ARDS in the neonatal period that has distinct pathophysiology compared with RDS, thus the management and clinical course of these patients is different. Although, there is a need for further trials using surfactant therapy in patients with NARDS,22 surfactant therapy is used in infants on neonatal units as rescue therapy. An example of the surfactant use in direct NARDS is the meconium aspiration syndrome (MAS); exogenous surfactant as treatment provides an increased pool of alveolar surfactant to overcome the inactivation thus increasing lung Crs.23 The use of exogenous surfactant in MAS has been shown to prevent the need for extracorporeal membrane oxygenation (ECMO) therapy but not reduce mortality.24
{kind=link}
A schematic figure illustrating the pathophysiology in neonatal RDS, direct NARDS and adult COVID-19 ARDS. A and B show concept graphs of changes in static compliance following surfactant administration from baseline in infants. C illustrates a change in static compliance from baseline in the nine patients treated with surfactant on a compassionate basis as rescue therapy to prevent need for ECMO. *Indicates surfactant administration. ARDS, acute respiratory distress syndrome; ECMO, extracorporeal membrane oxygenation; NARDS, neonatal acute respiratory distress syndrome; RDS, respiratory distress syndrome.
Leaving the neonatal setting and entering the merits of the COVID-19 ARDS, there is a strong ongoing debate on Crs and respiratory mechanics. Some authors argue that the values of Crs in severely hypoxic COVID-19 ARDS were higher than that found in ‘typical’ ARDS.25 In contrast, other authors have shown no substantial differences in Crs between the two kinds of ARDS.26 A recent prospective matched cohort study comparing patients with a similar level of hypoxaemia showed that patients with SARS-CoV-2 infection had a mean Crs of 20% higher and had lower driving pressures.27 However, this study enrolled patients with indirect aetiologies and longer intensive care unit length of stay before study entry in the group of ‘typical’ ARDS. Therefore, although it is still unclear whether Crs of typical ARDS and COVID-19 ARDS are comparable, the Crs response to surfactant administration may reflect more substantial parallels, mainly in direct cause of ARDS. A previous study by Tsangaris et al evaluated the administration of natural surfactant in patients with ARDS from a direct traumatic lung injury, demonstrating an increasing curve in Crs that reached a plateau 24 hours post-administration.28 We recorded a similar Crs response curve on nine patients with COVID-19 ARDS with extreme hypoxaemia, refractory to all rescue respiratory therapies, to whom we administered exogenous natural surfactant for compassionate use as a last resort to avoid ECMO (a detailed description of the surfactant supplementation is described elsewhere).29 Therefore, whatever the basal level of Crs between ‘typical’ direct ARDS and COVID-related ARDS, the response to the surfactant appears to be superimposable. This same Crs curve seems very similar to the trajectory occurring in newborn infants with RDS and NARDS after surfactant administration, likely secondary to the common pathophysiology of the diseases (figure 1).
Discussion
SARS-CoV-2 targets the AT2 cells that are vital in surfactant production. We know from studies in preterm infants that surfactant is critical in reducing surface tension and improving lung Crs. Improvement in Crs by increased aeration and reduced surface tension is likely to prevent the vicious cycle that results in worsening hypoxia and acidosis leading to pulmonary damage and an ongoing inflammatory insult to the lungs. A similar mechanism belongs to critically ill patients with COVID-19, higher surface tension worsens hypoxia and inflammation by both reducing Crs and increasing atelectasis, generating further hypoxia and inflammation leading to a vicious cycle that requires mechanical ventilation to maintain adequate oxygenation. Surfactant effectively breaks this cycle with improvement in hypoxia due to improved Crs in infants. We hypothesise that it can have a similar effect in patients with reduced Crs COVID-19 ARDS. However, as in the neonatal population, acknowledging the complexities of surfactant dysfunction in COVID-19 ARDS is crucial. There needs to be recognition and selection of patients’ relevant phenotype to receive surfactant therapy and thought given to dosage and delivery.
In conclusion, we believe that given the overlap in the pathophysiology of RDS and COVID-19 ARDS, the use of surfactant would be a valuable tool in the armoury of treatments for patients that present with direct ARDS secondary to COVID-19. RCTs are needed to identify which subgroup of patients with COVID-19 ARDS would benefit more from exogenous surfactant therapy, and given the difference in lung development and size, what dose and delivery method would be most effective.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical committee approvement was not necessary because of the 'opinion' nature of the study.
Acknowledgments
The authors would like to thank Chiesi Pharmaceuticals (Parma, Italy) for providing Curosurf for compassionate use on COVID-19 patients. We would also like to thank Dr Laura Fabbri for her scientific contribution. Proffesor Clark wants to thank MRC and BRC at UCL/UCLH. Dr Stefano Busani and Professor Massimo Girardis would like to thank all the medical colleagues and nurses who worked during this hard period in the three COVID-19 ICUs of the University Hospital Policlinico di Modena. The authors would like to acknowledge Dr J Cuddihy in proofreading the manuscript.
References
Footnotes
Contributors RMB and HWC planned and wrote the neonatal part of the paper, while MG and SB planned and wrote the adult COVID-19 part of the paper. All authors read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.