Article Text

Abstract
Background Research on cigarettes and adult asthma offers mixed findings, perhaps due to overlap with chronic obstructive pulmonary disease (COPD) and inadequate adjustment for other smoke exposures. Associations between other tobacco products, including e-cigarettes, and asthma are also understudied.
Research question Using Population Assessment of Tobacco and Health Study waves 2–4 (2014/2015–2016/2017) data, we assessed the relation between tobacco product use and asthma in persons unlikely to have COPD.
Study design and methods Prospective study of 10 267 adults aged 18–39 years without COPD diagnoses. Past-month tobacco use at wave 2 was modelled first as combustible versus non-combustible use and second as specific product categories (former, cigarettes, e-cigarettes, cigars, hookah, smokeless tobacco). Outcomes included lifetime asthma prevalence at wave 2, incidence (waves 3 and 4) and Asthma Control Test score (lower=worse). Multivariable regressions adjusted for predictors of asthma, including other smoke exposures: cigarette pack-years, secondhand smoke and marijuana use. Sensitivity analyses examined findings when persons >39 years and those with both COPD and asthma were added, and when smoke exposure adjustments were removed.
Results No product, including cigarettes and e-cigarettes, was associated with prevalence or incidence of asthma. Among people with asthma at wave 2, combustible tobacco (beta=−0.86, 95% CI (−1.32 to –0.39)) and cigarettes (beta=−1.14, 95% CI (−1.66 to –0.62)) were associated with worse asthma control. No tobacco product was associated with asthma control over time. In sensitivity analyses, tobacco use became associated with incident asthma as adults >39 years and those with asthma+COPD were added, and as adjustments for other smoke exposures were omitted.
Interpretation Although cigarette use was associated with worse asthma control, there were no longitudinal associations between combustible tobacco or e-cigarette use and new onset or worsening asthma in these preliminary analyses. Research on tobacco and asthma should exclude COPD and adjust for smoking history and other smoke exposures.
- Asthma
- Tobacco and the lung
Data availability statement
Data are available in a public, open access repository. PATH data are available for public use at https://www.icpsr.umich.edu/web/NAHDAP/studies/36498.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous research on the relationship between tobacco use and adult asthma is mixed. Studies with positive findings often did not account for the effects of confounders such as other smoke exposure and presence of comorbid chronic obstructive pulmonary disease (COPD) in study subjects.
WHAT THIS STUDY ADDS
This study avoids the problem of confounding seen in previous studies. After removing participants with comorbid COPD and adjusting for pack-years of smoking, secondhand smoke and use of cannabis, the cross-sectional analyses found that cigarette smoking was associated with poorer asthma control, but longitudinal analyses found that cigarettes and e-cigarettes were not associated with new-onset asthma or worsening of asthma over time.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Future research on tobacco and adult asthma should select samples to avoid confounding comorbid conditions and carefully adjust for other smoke exposures.
Introduction
Asthma is the most prevalent chronic respiratory disease worldwide.1 2 Unlike chronic obstructive pulmonary disease (COPD), which primarily begins in middle age among people with host risk factors and long-term exposure to tobacco smoke or air pollutants,3–5 asthma is a heterogeneous disease of reversible expiratory airflow limitation, often beginning in childhood.6 Asthma is thought to result from the complex interaction between genetic factors and environmental exposures at critical periods throughout life.7 8
The relationship between tobacco product use and adult asthma is complex. Cigarette smoking has long been thought to contribute to asthma onset and severity in adults (see reviews of prospective studies9 and cross-sectional studies in clinical populations10–13). Yet, several prospective studies found no association or mixed findings.14–18 Moreover, cigarette smokers with asthma frequently use other products, including electronic (e-)cigarettes,19 20 about which there are very few prospective studies.21
Methodological problems may have contributed to previous mixed findings. Many studies of tobacco use and asthma did not assess cigarette smoking history, use of multiple tobacco products and other smoke exposures, such as secondhand smoke and marijuana use, that could be confounders,16 18 22–25 and most prospective studies of asthma and tobacco did not account for COPD.16 17 22–26 (Up to one-third of adults with asthma eventually develop comorbid COPD,27 28 when patients present with features distinct from asthma.29 30) For example, a recent paper22 noted that combustible tobacco and e-cigarette use were both associated with adult-onset asthma; however, that study addressed neither comorbid COPD, nor history of cigarette smoking and other smoke exposures, all important potential confounders. Careful, prospective research is needed to clarify the relation between tobacco product use and asthma outcomes.
The Population Assessment of Tobacco and Health (PATH) Study is a large, national, longitudinal survey of tobacco product use and self-reported health outcomes.31 This report evaluated the relationships between tobacco product use and asthma diagnosis and symptoms among people aged 18–39 years old without comorbid COPD. Sensitivity analyses explored how adding participants over 40 years and those with comorbid COPD, as well as removing adjustments for cigarette smoking history and other smoke exposures, affected the association between tobacco product use and asthma.
Methods
Study design, setting and participants
The PATH Study recruitment employed a stratified address-based, area-probability sampling design at wave 1 (W1; 2013–2014) that oversampled adult tobacco users, young adults (18–24 years) and African-American adults.
Respiratory symptoms, including asthma symptoms, were first assessed in wave 2 (W2: 2014–2015, N=28 362), which served as the baseline assessment for this study. The weighted response rate at W2 was 83.2%. Follow-up data were collected at waves 3 and 4 (W3: 2015–2016; W4: 2016–2017) including 28 148 and 27 757 adult participants, respectively, with weighted response rates of 78.4% and 73.5% of W2 participants, respectively. Respondents were assessed in person with a computer-assisted interview approximately yearly.
For this study, we selected all W2 adults aged 18–39 years, excluding adults over 39 years and those who reported COPD (including chronic bronchitis or emphysema) or other non-asthma respiratory diseases at W1–4, to increase certainty that we were studying adult asthma (N=11 675). Participants with missing data on independent or dependent variables (N=1408, 12.1%) were also excluded, for a complete case analytical sample of 10 267.32 (Multiple imputation analyses were also conducted on the full sample, as described in the Statistical analysis section below.)
Complete PATH Study design methods have previously been published in detail;33 34 interviewing procedures, questionnaires, sampling, weighting and response rates can be found at https://doi.org/10.3886/Series606. All adult respondents provided informed consent.
Patient and public involvement
Patients or the public WERE NOT involved in the design, or conduct, or reporting, or dissemination plans of our research.
Patient-reported asthma diagnosis and symptoms
Asthma diagnosis
Similar to the National Health and Nutritional Examination Survey (NHANES),35 lifetime asthma diagnosis was assessed at baseline by asking: ‘Has a doctor, nurse or other health professionals EVER told you that you had any of the following lung or respiratory conditions? Choose all that apply. Asthma, COPD, etc.’ New diagnosis was assessed by asking: ‘IN THE PAST 12 MONTHS, has a doctor ever told you that you had any of the following lung or respiratory conditions? Choose all that apply. Asthma, COPD, etc.’ The asthma diagnosis questions were validated by demonstrating that self-reported asthma diagnosis in the PATH Study was associated with greater respiratory symptoms and impairments in functional status (see online supplemental appendix 1). Additionally, the prevalence of asthma diagnosis in the PATH Study was similar to the prevalence of asthma diagnosis in NHANES (see online supplemental appendix 1). Asthma at baseline (W2) and new asthma at follow-up (W3 or W4) were assessed by a combination of these two questions.
Supplemental material
Asthma control
The Asthma Control Test (ACT), a validated questionnaire designed for patients with asthma, includes five items on self-reported asthma symptoms (online supplemental table 1), each with answer options 1–5. Summary scores range from 5 to 25 (higher=better asthma control, for example, fewer symptoms; ACT score <20 indicates poorly controlled asthma).36 It has high internal consistency (Chronbach’s alpha=0.79), test–retest reliability (r=0.77) and criterion validity (correlation with specialist rating of asthma control r=0.52).37 An ACT score of 19 provided an optimum balance of sensitivity (71.3%) and specificity (70.8%) for detecting poorly controlled asthma in non-smokers37 and a score of 18.6 provided the maximum area under the receiver operator characteristic curve in smokers.38 The asthma symptom questions in the PATH Study were validated by demonstrating that self-reported asthma symptom severity was associated with functional status, and prevalence of asthma symptoms (wheeze) was similar to the prevalence of symptoms in NHANES (see online supplemental appendix 1). People with asthma were also asked whether they used asthma medications in the past 12 months (‘treated asthma’) and what class of medications they regularly used.
Exposures
Tobacco product use
Participants reported lifetime and past-month use of combustible products (cigarettes, traditional cigars, cigarillos, filtered cigars, pipe tobacco and hookah) and non-combustible products (snus pouches, other smokeless tobacco (loose snus, moist snuff, dip, spit or chewing tobacco) and e-cigarettes). Pictures and descriptions were displayed for each product to ensure accuracy.
Tobacco product use was modelled two ways. First, models included four mutually exclusive past-month categories—never use, former use but none in the past month, current non-combustible use only and current combustible product use (including those with non-combustible use).
Second, six product type categorical variables were developed that described past-month use: tobacco use but none in the past 30 days (‘former users’), and past 30-day use of cigarettes, e-cigarettes, cigars, smokeless tobacco, pipe or hookah. These 30-day use groups were not mutually exclusive, so individuals could be counted in several groups if they had used multiple products.
Finally, a variable for intensity of product use was created for each product type (frequency of use in the past month×quantity used per day on the days used). This variable was used in a series of additional analyses to assess for any linear or non-linear dose–response relationships between each product and both asthma prevalence and asthma incidence using bivariate and multivariable analyses. Lowess curves were created to examine whether there was a threshold at which exposure impacted asthma incidence or control (online supplemental file 2). Because no threshold was observed, we did not create any ‘threshold of use’ variables.
Covariates
As described in table 1, covariates were derived mostly from W2 data, and included variables that could be associated both with tobacco exposure and asthma (or respiratory symptoms in people with asthma). Sociodemographic variables included age, sex, race/ethnicity, education and urbanicity. Other W2 smoke-related exposures that could be associated with respiratory symptoms included pack-years of cigarette smoking,39 secondhand smoke exposure40 and past-month marijuana use.41 We included obesity categories based on self-reported height and weight (underweight: body mass index (BMI) <18.5; normal: BMI=18.5–24.9, overweight: BMI=25–29.9, class 1 obesity: BMI=30–34.9, class 2 obesity: BMI ≥35).
Characteristics of adults 18–39 years at wave 2 of the PATH Study*, by lifetime asthma status (percentages and means are weighted to reflect US population)
Statistical analysis
All main analyses were weighted using the W4 longitudinal (all waves) full-sample and replicate weights to adjust for the complex sample design and loss to follow-up. Weighted estimates from W1 to W4 of the PATH Study represent the residents of the USA at W4 who were in the civilian, non-institutionalised population at W1 (only W1 cohort was used). Variances were estimated using the Balanced Repeated Replication (BRR) method42 with Fay’s adjustment set to 0.3 to increase estimate stability.43 Pack-years of cigarette smoking, tobacco product past 30-day frequency variables and secondhand smoke exposure were Winsorised at the 95th, 95th and 99th percentiles, respectively, to limit the influence of outliers.44
Missing data
Participants who had missing asthma diagnosis data, tobacco product use/intensity data, or covariate data were omitted from the analytical sample. Compared with the analytical sample, the non-analytical sample was older (online supplemental table 6), included more men and racial/ethnic minorities, and had lower education level, contained more cigarette smokers (14.9% vs 10.8%, respectively) and more with ever asthma diagnosis (16.1% vs 12.2%, respectively). We repeated all main analyses (model 1 in tables 2–5) using multiple imputation to address missing data for all predictors and covariates using BRR, as was done in the complete case analyses. The multiple imputation analyses found only very small differences for a few variables, primarily in the CIs; thus, we report the complete case analyses here.
Weighted cross-sectional associations between past 30-day tobacco use and lifetime asthma diagnosis at wave 2 of the PATH Study*
Weighted prospective associations between wave 2 past 30-day tobacco use and new-onset asthma diagnosis at waves 3 or 4 of the PATH Study*
Weighted cross-sectional associations between past 30-day tobacco use and Asthma Control Test (ACT) score among adults 18–39 years with asthma at wave 2 of the PATH Study, lower coefficients reflect worse asthma control*
Weighted prospective associations between wave 2 past 30-day tobacco use and wave 3 Asthma Control Test (ACT) score among adults aged 18–39 years at wave 2 of the PATH Study, controlling for wave 2 ACT score, negative coefficients reflect worsening of asthma symptoms over time*
Analytical approach
We first examined the associations between tobacco use and covariates using either Χ2 or analysis of variance, as appropriate. We then examined cross-sectional associations between tobacco product use at W2 and both the presence of lifetime asthma diagnosis and asthma control (symptom severity) at W2. Finally, we evaluated the longitudinal associations between W2 tobacco product use and both new asthma diagnoses at W3 and W4 and ACT score at W3.
Multivariable weighted Poisson regression was used to obtain adjusted risk ratios (aRRs) and 95% CIs for each of the dichotomous outcomes. Multivariable linear regression was used to model asthma symptom control (ACT scores) at W3, adjusted for W2 ACT values to control for baseline asthma symptom severity.45 Similar regressions were used in two sensitivity analyses (online supplemental table 7) in which we first included adults over 40 years and those with both COPD and asthma diagnoses, and then also removed adjustments for cigarette pack-years, marijuana use and secondhand smoke exposure. All analyses were conducted using Stata survey data procedures, V.15.1 (StataCorp, College Station, Texas, USA), and using PATH Study W1–W4 Restricted Use Files.
Results
Participants with asthma
The weighted prevalence of lifetime asthma was 12.2% (SE=0.4). Characteristics and tobacco use of people with asthma are shown in table 1. About one-fifth of people with asthma (288 of the 1432) had taken asthma medication in the past 12 months. Tobacco use characteristics were largely similar between those never having asthma, those with untreated asthma (not taking medication) and those with treated asthma (taking medication), although those with untreated asthma were more likely to be past 30-day cigar smokers and current marijuana users than the other groups (p=0.03 and p<0.01, respectively). Four tables present the association between tobacco product use and asthma prevalence (table 2), asthma incidence (table 3), cross-sectional asthma control (table 4) and prospective asthma control (table 5), as described below.
Cross-sectional relationships between tobacco exposure and asthma prevalence
Multivariable models showed significant associations between lifetime asthma (table 2, model 2) and current cigar use (lifetime prevalence 14.5% in past 30-day cigar smokers vs 11.9% non-past 30-day cigar smokers, aRR=1.17, 95% CI (1.00 to 1.36)); marijuana use (15.1% vs 11.7%, aRR=1.26, 95% CI (1.07 to 1.48)); and weight status (16.4% vs 11.0%, aRR=1.62, 95% CI (1.30 to 2.01) for class 2 obesity vs normal weight). However, the relationship between cigars and lifetime asthma was borderline statistically significant (p=0.057). Additional analyses with quantity/frequency measures of tobacco product use did not detect a dose–response relationship between intensity of tobacco product use and lifetime asthma (not shown).
Relationship between tobacco exposure and asthma incidence
New-onset asthma at W3 or W4 was diagnosed in 1.3% (SE=0.2) of young adults aged 18–24 years, and 0.9% (SE=0.1) of adults aged 25–39 years (online supplemental table 10). In the multivariable longitudinal analyses (table 3, models 1 and 2), we found no association between any type of tobacco product use and new-onset asthma; we did find significant associations between new asthma and weight status (aRR=3.12, 95% CI (1.67 to 5.86) for class 2 obesity vs normal weight). Similar to the cross-sectional findings, additional analyses using quantity/frequency measures of tobacco product use were consistent with the lack of association (not shown).
Cross-sectional relationships between tobacco exposure and asthma control among people with asthma
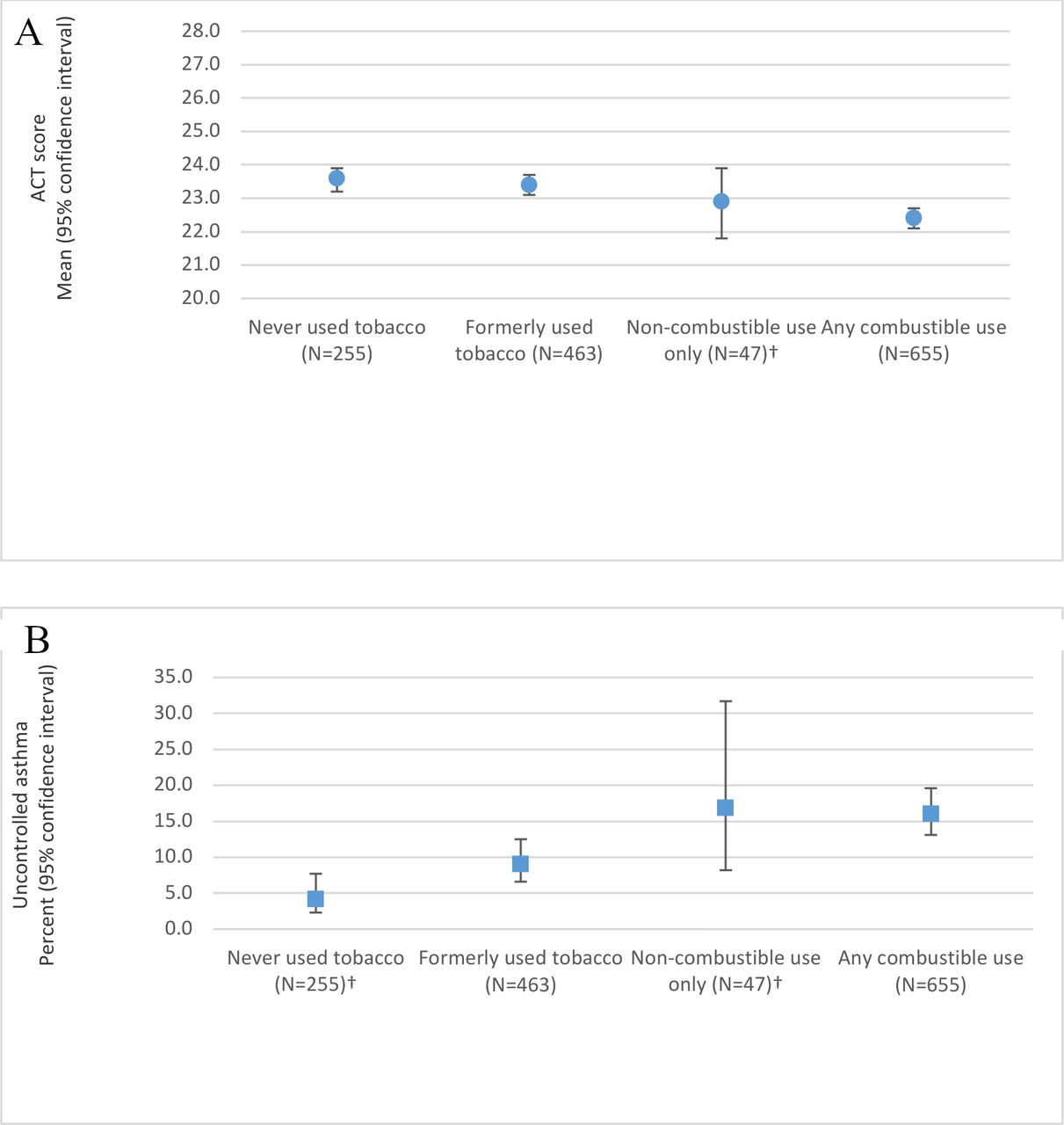
Figure 1 illustrates asthma control (as measured by ACT scores) by four categories of tobacco use in W2. Figure 1A shows that mean ACT score was about 1 point lower in combustible tobacco users compared with people who had never used tobacco (22.4 (SE=0.1) vs 23.6 (SE=0.2), respectively, two-sample t-test p<0.01). To illustrate the clinical significance of this finding, figure 1B shows that this difference translated into a higher percentage of combustible tobacco users with uncontrolled asthma symptoms compared with never tobacco users with uncontrolled asthma symptoms (16.1% (SE=1.6) vs 4.2% (SE=1.3), two-sample Χ2 p<0.01). Although non-combustible tobacco users had numerically lower asthma control (mean ACT scores) and higher proportions of people with uncontrolled symptoms than never tobacco users, the size of the non-combustible user group was small and these differences were not statistically significant.

Asthma control by Wave 2 tobacco usea among adults age 18-39 of the PATH Study,bPanel A, Weighted mean Asthma Control Test (ACT) score, and Panel B, Percent with uncontrolled asthmac. aNever used tobacco = Never used tobacco, not even one puff; Formerly used tobacco = ever used tobacco, but not in the past 30 days; Non-combustible use only = exclusive non-combustible (e-cigarette, smokeless tobacco, or snus) use in the past 30 days; Any combustible use = combustible (cigarette, pipe, hookah, or cigar) use in the past 30 days regardless of non-combustible use. bN = 1,420 Wave 2 adult (age 18-39 years) respondents with valid Wave 2 ACT scores, without chronic obstructive pulmonary disease or other non-asthma respiratory disease at Waves 2-4, and with Wave 4 Population Assessment of Tobacco and Health (PATH) Study longitudinal (all-waves) weights and complete data on all analytic variables. cUncontrolled asthma is defined as an ACT score of 19 or less. The ACT has a possible range of 5 to 25, where a higher score represents better controlled asthma. †Estimate should be interpreted with caution because it has low statistical precision. It is based on a denominator sample size of less than 50, or the coefficient of variation of the estimate or its complement is larger than 30%. ACT, Asthma Control Test.
In the cross-sectional, adjusted, multivariable analyses of asthma control (ACT scores; table 4), scores were lower (worse control) among current combustible tobacco users (beta=−0.86, 95% CI (−1.32 to –0.39); model 1) and cigarette users (beta=−1.14, 95% CI (−1.66 to –0.62); model 2). We also found significant associations between asthma control and sex (male sex beta=0.47 (0.16 to 0.78)) and education (eg, for some college beta=0.72 (0.13 to 1.32)). ACT scores among those with treated asthma were lower than ACT scores in untreated asthma by about 3 points (beta=−3.26, 95% CI (−4.05 to –2.46); model 1). Additional analyses with quantity/frequency measures of each tobacco product use also found a negative association between intensity of cigarette use and ACT scores (not shown).
Longitudinal relationships between tobacco exposure and asthma control among people with asthma
In the longitudinal multivariable analyses, there was little association with asthma control (mean ACT score) over time (W3 ACT score, while controlling for W2 ACT score). No tobacco use category at W2 was associated with ACT score at W3 (table 5, models 1 and 2). Of all the predictor variables, higher ACT score at W2, male sex and higher education were significantly associated with better W3 asthma control in both models, while using asthma controller medication at W2 predicted significantly worse W3 asthma control in both models. Additional analyses that modelled quantity/frequency of tobacco product use were consistent with the lack of a longitudinal association between presence or absence of specific product use and ACT scores.
Sensitivity analyses examining the relationships between tobacco exposure and asthma prevalence and incidence
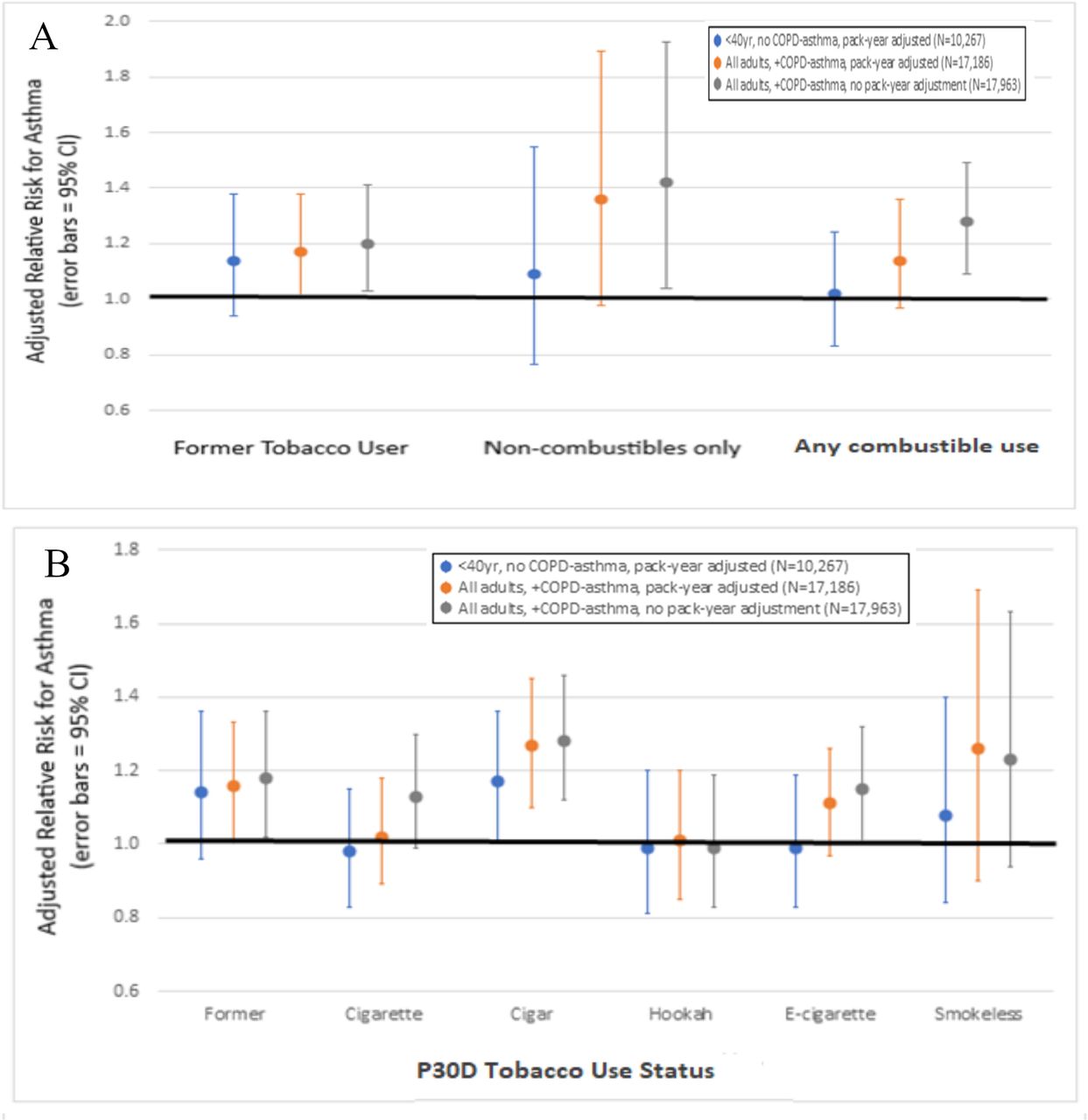
To examine why these findings differed from a previous report using PATH Study data,22 a series of sensitivity analyses were conducted to explore how including older people (≥40 years), those with COPD and asthma, and covariates indicating other smoke exposures and pack-years of smoking impacted the estimates described above. As illustrated in figure 2A, expanding the sample resulted in significant cross-sectional associations between tobacco use and asthma, suggesting that these associations are due to the relationship between tobacco and COPD rather than tobacco use and asthma. As shown in figure 2B, associations with asthma became statistically significant for former smokers, cigar users and e-cigarette users. Longitudinal associations also became larger, and the associations between new-onset asthma and any combustible use and cigarette use become statistically significant (online supplemental table 7).
{kind=link}
{kind=link}
Weighted and adjusteda sensitivity analysesb for cross-sectional associations between past 30-day combustible v. non-combustible tobacco usec (Panel A) and past 30-day tobacco product used (Panel B) and lifetime asthma diagnosis among adults 18+ at Wave 2 of the PATH Study. aAll relative risks are adjusted for body mass index, age, sex, race/ethnicity, education, and lives in urban area. Relative risks in the “<40, No COPD” and “All, COPD+Asthma” groups are also adjusted for cigarette pack-years, past-week secondhand smoke, and past-month marijuana use. b<40 years, No COPD = Wave 2 adult (age 18-39 years) respondents without chronic obstructive pulmonary disease or other non-asthma respiratory disease at Waves 2-4, with Wave 4 Population Assessment of Tobacco and Health (PATH) Study longitudinal (all-waves) weights, and complete data on all analytic variables; All adults, COPD+asthma = Wave 2 adult (age 18+ years) respondents without chronic obstructive pulmonary disease at Waves 2-4, unless also having asthma at Waves 2-4, or other non-asthma respiratory disease at Waves 2-4, with Wave 4 PATH Study longitudinal (all-waves) weights, and complete data on all analytic variables; All adults, COPD+asthma, without adjustment = Wave 2 adult (age 18+ years) respondents without chronic obstructive pulmonary disease at Waves 2-4, unless also having asthma at Waves 2-4, or other non-asthma respiratory disease at Waves 2-4, with Wave 4 PATH Study longitudinal (all-waves) weights, and complete data on all analytic variables. For this group, cigarette pack-years, past-week secondhand smoke, and past-month marijuana use are not involved in defining the analytic sample and are not included in the models. cNever used tobacco (reference group) = Never used tobacco, not even one puff; Formerly used tobacco = ever used tobacco, but not in the past 30 days; Non-combustible use only = exclusive non-combustible (e-cigarette, smokeless tobacco, or snus) use in the past 30 days; Any combustible use = combustible tobacco (cigarette, pipe, hookah, or cigar) use in the past 30 days regardless of non-combustible use. dEach past 30-day tobacco product use category is dichotomous as any use versus no use in the past 30 days. COPD, chronic obstructive pulmonary disease.
Discussion
In this large, nationally representative, prospective study, combustible tobacco and cigarettes were associated with poorer asthma control compared with control among non-users in the cross-sectional analysis. These findings strengthen the body of research showing adverse effects of cigarette exposure, even in a young population. No type of tobacco use was associated with a new diagnosis of asthma among adults nor with worsening asthma control over time in analyses that carefully excluded persons with COPD and adjusted for smoking history and other smoke exposures.
In contrast, unadjusted sensitivity analyses including older adults and those with COPD and asthma resulted in significant associations between tobacco use and asthma, suggesting that these associations between tobacco product use and asthma in the sensitivity analyses are spurious, or due to the relationship between tobacco and COPD rather than between tobacco and asthma. A recent meta-analysis of eight epidemiological studies concluded that smoking was related to incident asthma (RR 1.61, 95% CI (1.07 to 2.42)),9 but most failed to exclude people with COPD,16 17 22–26 and many did not adjust for other smoke exposures,16 18 22–25 which may explain the different conclusion in the present study.
Other cross-sectional research has also shown that smoking was associated with poor asthma control,10 11 13 and unadjusted prospective studies have also indicated that smoking predicted poor asthma control and asthma exacerbation over time,46 47 but these studies also did not remove people with COPD or adjust for cumulative past smoking and other smoke exposures. In contrast, at least one study that carefully controlled for these factors did not show an association between smoking and new asthma48; rather, similar to our study, use of controller medications at baseline was associated with persistence of asthma.48
Similar to other recent research, cigarette smoking was not associated with a higher or lower risk of lifetime asthma in W2 of the PATH Study (2014–2015),10 14 49 indicating that asthma is not deterring smoking in the USA. Because smoking is associated with worse asthma control in this and other studies,50 51 and causes or exacerbates multiple other diseases, people with asthma should still be encouraged to quit. Tailored interventions may be useful.52
Little is known about e-cigarette use and the development of asthma in adults. Our study conclusion—that there is no association between e-cigarette use and new-onset asthma—contrasts with cross-sectional epidemiological studies53 and the only other prospective epidemiological study of e-cigarette use and asthma.22 The prospective study used the same data as our study but included older adults as well as those with asthma and COPD and did not adjust for history of smoking and other smoke exposures. By omitting people with COPD and those over age 40 years from this study, as well as by adjusting for other smoke exposures, we carefully isolated the effect of tobacco product use on the development of asthma in adulthood. It should be noted that about 80% of e-cigarette users in this cohort also smoked cigarettes. The small numbers of e-cigarette-only users in this study limited the ability to test for modest associations.
The heterogeneity of asthma may also contribute to mixed findings in epidemiological research, with some types of asthma potentially being more sensitive to smoking. For example, in a longitudinal study that measured lung function, smoking did not worsen the decline of lung function among those with childhood-onset asthma but was associated with greater decline in lung function among patients with adult-onset asthma.14 The PATH Study did not obtain information that would allow us to determine asthma subtypes.
Several additional study limitations warrant discussion. At the time of these analyses, PATH Study data for tobacco, asthma and asthma symptoms were available W2 through W4, or for only three waves. Analyses over longer time periods will be able to elucidate the longer-term impact of tobacco product use on asthma. Additionally, the e-cigarettes used during the years of these analyses were different from the fourth-generation e-cigarettes now on the market. E-cigarette devices are changing rapidly and are still relatively recent; thus, additional research should examine e-cigarettes over time. Finally, the PATH Study does not measure all subject characteristics and exposures associated with asthma risk, such as allergy or atopy,54 environmental ozone specifically,26 55 environmental air pollution in general56 and prenatal smoke exposure.57 Such measures could enable more specific predictive models. Despite these limitations, these carefully adjusted analyses of a US population sample provide important, current information about the impact of tobacco products on asthma.
Conclusion
Combustible tobacco and cigarette use were associated with worse asthma control cross-sectionally, but combustible tobacco product and e-cigarette use were not associated with asthma prevalence, incident asthma or change in symptom severity in adults with asthma when individuals with COPD were excluded and analyses were adjusted for other smoke exposures. Clinicians caring for patients with asthma should address smoking, and research on the impacts of tobacco on health should carefully measure and adjust for these potential confounders.
Data availability statement
Data are available in a public, open access repository. PATH data are available for public use at https://www.icpsr.umich.edu/web/NAHDAP/studies/36498.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The study was conducted by Westat and approved by the Westat Institutional Review Board (IRB) (Westat IRB # 0000695; PATH project number #8954). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @stkidsdoc
Contributors JDS, MFB and SET were involved in the initial conception of the research questions. All authors were involved in the planning of the data analyses and interpretation of the data analyses. MJH analysed the data. MFB wrote the manuscript. All authors were involved in reviewing, editing and final approval of the manuscript. MFB is responsibile for the overall content.
Funding This manuscript is supported with federal funds from the National Institute on Drug Abuse, National Institutes of Health, and the Center for Tobacco Products, Food and Drug Administration (FDA), Department of Health and Human Services, under contract to Westat (contract nos. HHSN271201100027C and HHSN271201600001C).
Disclaimer The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the US Department of Health and Human Services or any of its affiliated institutions or agencies.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.