Article Text

Abstract
Background Interstitial lung disease (ILD) has emerged as the most common indication for lung transplantation globally. However, post-transplant survival varies depending on the underlying disease phenotype and comorbidities. This study aimed to describe the demographics, disease classification, outcomes and factors associated with post-transplant survival in a large single-centre cohort.
Methods Data were retrospectively assessed for 284 recipients who underwent lung transplantation for ILD in our centre between 1987 and 2020. Patient characteristics and outcomes were stratified by three eras: 1987–2000, 2001–2010 and 2011–2020.
Results Median patients’ age at time of transplantation was significantly higher in the most recent decade (56 (51–61) years, p<0.0001). Recipients aged over 50 years had worse overall survival compared with younger patients (adjusted HR, aHR 2.36, 95% CI 1.55 to 3.72, p=0.0001). Better survival was seen with bilateral versus single lung transplantation in patients younger than 50 years (log-rank p=0.0195). However, this survival benefit was no longer present in patients aged over 50 years. Reduced survival was observed in fibrotic non-specific interstitial pneumonia compared with idiopathic pulmonary fibrosis, which remained the most common indication throughout (aHR 2.61, 95% CI 1.40 to 4.60, p=0.0015).
Conclusion In patients transplanted for end-stage ILD, older age and fibrotic non-specific interstitial pneumonia were associated with poorer post-transplant survival. The benefit of bilateral over single lung transplantation diminished with increasing age, suggesting that single lung transplantation might still be a feasible option in older candidates.
- lung transplantation
- interstitial fibrosis
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Lung transplantation for various end-stage forms of interstitial lung disease has become increasingly common and has emerged as the most common indication for lung transplantation globally.
WHAT THIS STUDY ADDS
Because of the long-standing nature of our lung transplant programme, this study was uniquely positioned to look at differences in patient characteristics, disease phenotypes and post-transplant outcomes over three decades.
Key findings were that idiopathic pulmonary fibrosis remained the main indication for lung transplantation, that patients with fibrotic non-specific interstitial pneumonia had worse survival post-transplant and that patients older than 50 years no longer benefited from bilateral versus single lung transplantation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our data support that single lung transplantation is still a reasonable option and may even be preferred in older transplant candidates.
Our study confirms that survival after lung transplantation is affected by many reasons, making it challenging to select transplant candidates who may benefit most from it and highlighting the importance of multidisciplinary team meetings.
Survival of fibrotic non-specific interstitial pneumonia after lung transplantation needs to be further investigated in larger studies.
Interstitial lung disease (ILD) is an umbrella term for a group of chronic respiratory diseases affecting the lung parenchyma with a variable but often dismal prognosis.1 Among these diseases, idiopathic pulmonary fibrosis (IPF) has worse disease outcomes compared with other types of ILD.2 Lung transplantation offers a life-saving therapy for highly selected patients with severe end-stage ILD, which has now become the most common indication globally.3 However, post-transplant survival is variable depending on a range of factors. Common factors associated with worse post-transplant survival include older age and presence of comorbidities such as gastro-oesophageal reflux disease (GERD), diabetes mellitus, severe pulmonary hypertension, obesity and Pseudomonas aeruginosa colonisation.4–9
On the other hand, transplant techniques, patient selection and management of comorbidities and postoperative complications have improved over time and are expected to advance further with increasing experience, thus improving post-transplant survival.10
The availability of lung transplants remains limited due to a lack of donor organs.11 It is therefore important to identify factors affecting survival in order to transplant candidates who could potentially have the best survival benefits. In the USA and some European countries, the priority for a lung transplant is based on the Lung Allocation Score.12 This score is determined by the predicted survival benefit, which is the difference between the projected waitlist survival and post-transplant survival, and is based on objective and transparent data.13 As a result of the implementation of the Lung Allocation Score, patients with ILD are relatively favoured for transplantation.14 In the UK, an allocation system to determine priority was only implemented in 2017 and this allocation system is based on centre decision and national urgency.11
In this study, we have reviewed our institutional cohort of 284 patients who underwent lung transplantation for ILD between 1987 and 2020. We aimed to describe the demographics and specific diagnostic classification of the cohort, the outcomes and explored factors influencing post-transplant survival.
Methods
Study design
Data were retrospectively analysed from our centre’s lung transplant database and additional data were retrieved from patients’ medical records as needed. In this study, we included consecutive patients who underwent lung transplantation for ILD between 1987 and 2020 at the Freeman Hospital, Newcastle upon Tyne, UK. All post-transplant follow-up until June 2020 was evaluated. Because of the long-standing nature of our lung transplant programme, this study was uniquely positioned to stratify outcomes over three decades, to look at differences in patient characteristics, disease phenotypes and post-transplant outcomes. Due to the low number of transplants performed from 1987 to 1990, the start of our transplant programme, these were added to the 1991–2000 decade. As such, post-transplant outcomes were compared over the following three decades: 1987–2000, 2001–2010 and 2011–2020.
Evaluation
Subtypes of ILD were classified as IPF, fibrotic non-specific interstitial pneumonia (fibrotic NSIP), connective tissue disease-related ILD (CTD-ILD), sarcoidosis, chronic hypersensitivity pneumonitis (cHP) and other types of pulmonary fibrosis (drug-induced pulmonary fibrosis, pulmonary fibrosis secondary to pulmonary surfactant deficiency, silicosis and asbestosis, postradiotherapy pulmonary fibrosis, cryptogenic organising pneumonia, desquamative interstitial pneumonia and unclassifiable idiopathic interstitial pneumonitis).15 The consensus classification of idiopathic interstitial pneumonias was used.15 16 For patients assessed before 2002, patients with cryptogenic fibrosing alveolitis, fibrotic lung disease and pulmonary fibrosis with a usual interstitial pneumonia pattern on imaging were classified as IPF.
All patients underwent pretransplant assessment at the Freeman Hospital and received single lung, bilateral lung or heart-lung transplantation. We assessed the baseline characteristics, survival, incidence of chronic lung allograft dysfunction (CLAD) and other major transplant-associated comorbidities, such as renal dysfunction and malignancy.
Definitions
Pulmonary hypertension
An estimated pulmonary artery systolic pressure of ≥50 mm Hg, determined via tricuspid regurgitation velocity and/or presence of moderate or severe right ventricular dysfunction on transthoracic echocardiogram were considered signs of significant pulmonary hypertension.
Coronary artery disease
Coronary artery disease was defined as a history of myocardial infarction, non-ST elevation myocardial infarction or symptomatic angina, or abnormal coronary imaging. Our centre routinely performs CT coronary angiography or fluoroscopic invasive coronary angiogram for patients aged 50 years and older or those with risk factors for cardiovascular disease. Significant coronary artery disease was defined by coronary angiogram as >50% stenosis of the left main stem, >70% stenosis in a major coronary vessel or 30%–70% stenosis with a fractional flow reserve ≤0.8.17
Gastro-oesophageal reflux disease
GERD was defined as a positive history of reflux symptoms and diagnosed as such by the treating clinician.
Chronic lung allograft dysfunction
CLAD, the clinical syndrome of chronic graft rejection, is an umbrella term which includes two main phenotypes, bronchiolitis obliterans syndrome (BOS) and restrictive allograft syndrome (RAS), and a mixed phenotype with features of both.18 19 Data on CLAD were included based on the diagnosis and phenotype listed in the medical notes according to the then applicable guideline. Consequently, data on RAS and mixed phenotypes were only available for the most recent decade, as these phenotypes were only acknowledged as separate phenotypes of CLAD recently.
Patient and public involvement
As it was a retrospective, observational cohort study, patients were not involved in the design and recruitment of the study.
Statistical analyses
All analyses were performed using GraphPad Prism V.9.4 (San Diego, California, USA). Results are expressed as mean (SD) or median (IQR) wherever appropriate. Baseline characteristics of patients were assessed and compared over time using Student’s t-test, Mann-Whitney U and Kruskal-Wallis tests for continuous data and χ2 tests for categorical data. Factors influencing survival were assessed using Kaplan-Meier curve with log-rank test. Independent predictors of survival were identified using univariate and multivariate Cox proportional hazards regression analysis, with results reported as HRs and 95% CIs. P values are two tailed, and a p<0.05 is considered statistically significant.
Results
Patient characteristics
Between 1987 and 2020, 284 patients with end-stage ILD underwent lung transplantation at our centre. Baseline patient characteristics at time of transplantation are shown in table 1. Median age at time of transplantation was 55 (48–60) years and most of the patients (70.4%) were male. Of the patients who were transplanted, 186 (65.5%) had IPF, 23 (8.1%) fibrotic NSIP, 21 (7.4%) sarcoidosis, 18 (6.3%) cHP, 17 (6.0%) CTD-ILD and 19 (6.7%) pulmonary fibrosis secondary to other causes. Regarding type of transplant, 145 patients (51.1%) received a bilateral lung transplant (BLT), 137 (48.2%) a single lung transplant (SLT) and 2 (0.7%) a heart-lung transplant. Median time on the waiting list was 135 (65–308) days.
Baseline characteristics of all patients and stratified by era
The most common comorbidity at time of transplantation was pulmonary hypertension in 31.3% of patients, followed by GERD in 22.0%, essential hypertension in 12.9%, diabetes mellitus in 11.6% and coronary artery disease in 8.9% of patients.
Differences in basic characteristics over time
As the study spanned over three time periods, we compared the patients’ characteristics across the decades (1987–2000, 2001–2010 and 2011–2020) (table 1). The majority of patients (152, 53.5%) were transplanted in the most recent era compared with 84 (29.6%) in 2001–2010 and 48 (16.9%) in 1987–2000. Median patients’ age at time of transplantation was significantly higher in the most recent decade (56 (51–61)years) compared with before (p<0.0001). We noted a significant shift from single to BLT over the eras. In 1987–2000, SLT was performed in 93.8% of the patients, while in the last decade most patients (75.7%) received a BLT.
Furthermore, there is a change in indication for transplantation. In the earliest decade, the main indication for transplantation was IPF (89.6%), followed by sarcoidosis (10.4%). Nowadays, we see great variation in indications with IPF still the main indication in 59.2%, followed by fibrotic NSIP (11.2%), cHP (9.2%), CTD-ILD (8.6%), sarcoidosis (3.9%) and other causes of pulmonary fibrosis (7.9%). Significantly less patients with ILD were on maintenance corticosteroids at the time of transplantation in the most recent era compared with before (p=0.0303).
With respect to comorbidities, GERD was significantly more common in 2011–2020 compared with before (p=0.004), with no differences in incidence of the other comorbidities. Further pretransplant workup showed that patients transplanted in 2001–2010 had the lowest estimated glomerular filtration rate and 6 min walk test distance at time of assessment. P. aeruginosa was isolated in 19 patients (7.9%) prior to transplantation with the highest incidence in 2011–2020 but without significant difference (p=0.0747).
Median time of follow-up and survival
At the time of the study, 98 (34.5%) patients were still alive (table 1). Median duration of overall follow-up was 3.2 (0.7–6.9) years and, in deceased patients, the median time to death was 2.4 (0.2–6.6) years. Patients who were still alive at the time of the study had a higher 6 min walk distance (293 m (205–366) vs 264 m (150–324), p<0.0107), forced expiratory volume in one second (54% (17) vs 48% (16), p<0.0060) and forced vital capacity (53% (41–63) vs 45% (36–56), p<0.0051) at pretransplant assessment (data not shown).
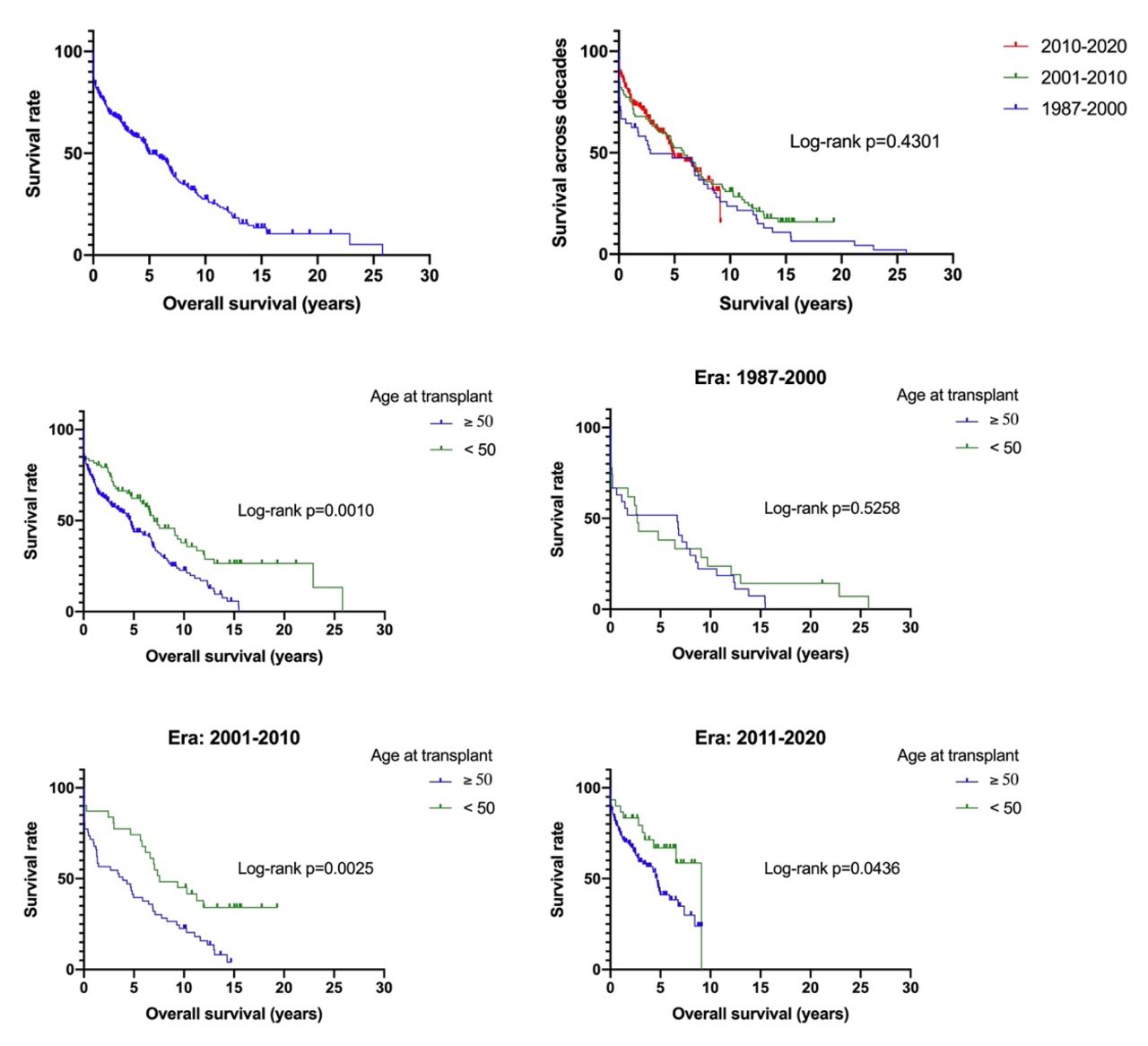
Kaplan-Meier curves of overall survival are displayed in figure 1. Overall median survival was 5.0 years with no difference in survival across the three different eras. The 30-day, 1-year, 3-year, 5-year and 10-year overall survival rates were 86%, 75%, 61%, 50% and 28%, respectively.

Kaplan-Meier curves demonstrating overall survival (top left, median survival 5 years), across the three decades (top right, median survival 1987–2000: 2.8 years, 2001–2010: 5.9 years and 2010–2020: 4.9 years) and according to age (middle left: overall, middle right: 1987–2000, bottom left: 2001–2010, bottom right: 2011–2020).
Predictors of survival
In survival analyses, patients less than 50 years old at the time of transplant had a better post-transplant survival than those who were older (log-rank test p=0.0010). This was seen in the two most recent eras, but not in the earliest era 1987–2020 (figure 1). With respect to type of organ transplantation, no difference in favour of BLT compared with SLT was seen in overall (log-rank test p=0.0561) and across the three eras. However, looking at patients age at transplantation, a difference in favour of BLT was present in younger patients <50 years (log-rank test p=0.0195) (figure 2).

Kaplan-Meier curves comparing post-transplant survival by organ transplanted in all patients (top left), patients aged ≥50 years (middle left), <50 years (bottom left) and across eras: 1987–2000 (top right), 2001–2010 (middle right) and 2011–2020 (bottom right). Median survival in patients aged ≥50 years with bilateral lung transplantation was 4.7 years (30-day, 1-year, 3-year and 5-year overall survival 88%, 73%, 59% and 42%, respectively) compared with 4.3 years in single lung transplantation (30-day, 1-year, 3-year and 5-year overall survival 85%, 70%, 56% and 43%, respectively). Median survival in patients aged <50 years with bilateral lung transplantation was 9.1 years (30-day, 1-year, 3-year and 5-year overall survival 92%, 86%, 80% and 73%, respectively) compared with 5.6 years in single lung transplantation (30-day, 1-year, 3-year and 5-year overall survival 80%, 77%, 59% and 52%).
There was a significant difference in survival across diagnosis (log-rank test p=0.0385). Post hoc analysis showed that significant differences in survival were only present between fibrotic NSIP and IPF (p=0.0082) and sarcoidosis (p=0.0056) (figure 3). Further comparison of characteristics and post-transplant complications of patients with IPF and fibrotic NSIP showed no relevant differences except more NSIP patients were treated with corticosteroids at time of transplant (online supplemental table 1).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves by ILD classification (top) and fibrotic NSIP compared with IPF (middle) and sarcoidosis (bottom). Other comparisons were not significantly different. cHP, chronic hypersensitivity pneumonitis; CTD-ILD, connective tissue disease-related interstitial lung disease; IPF, idiopathic pulmonary fibrosis; NSIP, non-specific interstitial pneumonia.
Cox regression analyses showed that age at transplantation of ≥50 years was associated with poorer survival (unadjusted HR 1.76, 95% CI 1.27 to 2.49, p=0.0010) and remained significant on multivariate analysis (adjusted HR (aHR) 2.36, 95% CI 1.55 to 3.72, p=0.0001). Stratified according to the different eras, this difference in survival outcome was seen in the 2001–2010 and 2011–2020 eras but not 1987–2000 (table 2). Overall, BLT was not associated with better survival compared with SLT (unadjusted HR 0.75, 95% CI 0.55 to 1.00, p=0.0569), but a survival benefit of BLT over SLT was present in patients aged less than 50 years (unadjusted HR 1.93, 95% CI 1.06 to 3.72, p=0.0387).
Cox proportional hazard regression analyses of factors affecting lung transplant survival
According to primary lung disease, fibrotic NSIP and CTD-ILD had worse survival outcomes compared with IPF (aHR 2.61, 95% CI 1.40 to 4.60, p=0.0015 and aHR 2.11; 95% CI 0.96 to 4.16, p=0.0435, respectively). When looking at the different eras, this difference in survival outcome was only seen in fibrotic NSIP in the 2001–2010 era. Maintenance treatment with corticosteroids at the time of transplantation negatively affected outcome (unadjusted HR 1.50, 95% CI 1.04 to 2.24, p=0.0378), however, this difference was no longer present in multivariate analysis.
Finally, isolation of P. aeruginosa at the time of transplantation carried a significant mortality risk (unadjusted HR 3.29, 95% CI 1.00 to 7.91, p=0.0202) (data not shown). However, because of the low number, this variable was not included in the multivariate model. Other baseline characteristics (see table 1) did not significantly affect survival.
Post-transplant complications
Overall, essential hypertension and chronic kidney disease were the most common post-transplant complications in 52.5% and 51.3% of patients, respectively (online supplemental table 2). Seven patients (2.5%) developed end-stage renal failure requiring long-term renal replacement therapy and two patients underwent renal transplantation, of which one underwent renal retransplantation.
Of 261 patients, 98 (37.5%) had pulmonary function decline consistent with CLAD with a median time from transplant to occurrence of 2.7 (1.7–5.3) years. In the most recent era, BOS was the most common phenotype in 87%. Five out of 40 patients (12.5%) were classified with a mixed phenotype and one patient developed RAS ab initio.
Skin malignancy was the most frequent type of malignancy in 27 patients (10.3%), followed by solid-organ malignancy and post-transplant lymphoproliferative disorder in 3.8% and 3.4% of patients, respectively. Ten patients (3.8%) had significant bronchial stenosis requiring stenting. The incidence of CLAD and bronchial stenosis was higher in the 2001–2010 era compared with the other eras (p=0.0173 and p=0.0244, respectively).
Discussion
ILD is currently the most common indication globally for lung transplantation and represents a very heterogeneous group of progressive lung diseases with varying rates of post-transplant survival.3 The key findings of this single-centre analysis were that IPF remained the leading indication for lung transplantation within the ILD category, although the landscape has become more diverse, and that patients under 50 years of age had better overall survival, with also a significant difference in survival favouring BLT in this patient cohort.
In recent decades, more knowledge has been gained about the range of disease phenotypes within ILD.15 This is also reflected in the diversity of indications for transplantation for ILD that we see today. IPF was still by far the main indication for transplantation, but transplants for other end-stage forms of ILD have become increasingly common. This is also likely due to a better classification of patients with ILD due to widespread adoption of specialist ILD clinics and multidisciplinary team meetings to accurately phenotype patients, with those patients previously falling under a different subclass. For example, the IPF subclass in the earliest decade will probably also have included other causes of end-stage ILD, such as fibrotic NSIP or cHP. Interestingly, patients transplanted for end-stage fibrotic NSIP had significantly worse survival than those transplanted for IPF. More patients with fibrotic NSIP were on maintenance corticosteroids at the time of transplantation compared with IPF patients and it is conceivable that patients with fibrotic NSIP received higher cumulative doses of corticosteroids. We were unable to identify other differences in characteristics or post-transplant complications between both groups, but some possibly relevant data on cause of death might be lacking. Also, the number of cases of fibrotic NSIP in our cohort was low. Therefore, survival of fibrotic NSIP after lung transplantation needs to be studied further in larger studies.
Although data are limited, several studies reported that post-transplant survival for CTD-ILD was similar to IPF.20 21 However, in our multivariate analysis, we observed worse survival in patients with CTD-ILD compared with IPF. The subgroups were too small for further subclassification (eg, scleroderma)22 23 and subanalyses regarding comorbidities (eg, GERD) and CLAD incidence.
In addition to a change in indication, the median patient’s age at time of transplantation has also increased over time, as can be seen in other indications for lung and other solid organ transplants generally and is due to increased experience and an ageing population.21 24 Worldwide data indicated an increase in the proportion of lung transplant recipients aged >65 years from 2.6% in 2004 to 17% in 2016, mainly due to an increase in older IPF patients being transplanted.22 Irrespective of the cause of underlying disease, older recipients have more comorbidities and higher post-transplant mortality compared with younger recipients.4 25 26 This increase in age also raises concerns regarding a higher risk of malignancy, the third most common cause of death in survivors >5 years, after CLAD and infections, and may be more pronounced in this population due to the development of age-associated neoplasms.20 Next to this, older recipients appear to be at greater risk for drug toxicity, vascular events and cognitive decline.21 27 For these reasons, age ≥65 years is considered a contraindication to lung transplantation in some centres. However, IPF patients are particularly negatively affected when such age-specific restrictions are applied.28
In our study, we also noticed a significant increase in age over time and worse overall survival in patients older than 50 years with a 1.76 times higher risk of death (95% CI 1.27 to 2.49) compared with those who were younger. This is at a slightly lower age than that recorded in the ISHLT registry.3 Indeed, in post hoc analyses, we observed a significant increase in mortality from the age group 45–50 years to 50–55 years (1-year and 3-year overall survival 81% and 72%, and 70% and 56%, respectively, p=0.0007) and beyond. There were no differences in indication for transplantation and baseline patient characteristics between these two age categories, except for a higher incidence of severe pulmonary hypertension in the latter category. This may have contributed to the significantly higher mortality rate and emphasises the importance of careful patient selection, monitoring and risk assessment. On the other hand, transplant benefit might be similar in older and younger recipients, provided older recipients are carefully selected and we have transplanted well-selected patients up to 72 years old in our centre. In essence, age itself should not necessarily exclude the possibility of lung transplantation, but more data are needed to better risk-stratify older patients. This is especially important in the antifibrotic era, where attenuation of disease progression could delay the need for lung transplantation beyond the age of eligibility.28 The International Society for Heart and Lung Transplantation does not endorse a strict upper age limit, and candidacy in elderly patients remains a centre-specific decision.29
With respect to type of organ transplantation, a transition from single to BLT has been observed over time, also in our centre. The debate regarding the ideal procedure for IPF, BLT versus SLT, is still ongoing and based on conflicting reports.25 30–36 This debate is based not only on post-transplant outcome, but also on the risk of death on the waiting list. Two recent studies looked at restrictive listing for BLT compared with unrestricted listing (BLT and SLT) and found that unrestricted listing was associated with lower rates of removal from the waiting list and death,37 higher transplant rates37 and, interestingly, even lower 1-year and 3-year survival rates in BLT in patients with ILD with severe pulmonary hypertension and a high Lung Allocation Score.38
Overall, we noticed a trend towards better survival in favour of BLT, which was significant in patients <50 years (median overall survival 9.1 years in BLT vs 5.6 years in SLT, log-rank p=0.0195; HR 1.93, 95% CI 1.06 to 3.72, p=0.0387) but not in older patients (median overall survival 4.7 years and 4.3 years, respectively, log-rank p=0.6529). This supports the fact that SLT is still of value, especially in elderly patients. Ultimately, the choice of procedure is often centre dependent and, apart from the underlying indication, mostly driven by donor availability and ethical considerations (helping two vs one patient with one donor).20
The strength of our study was that we included patients over a long period of 34 years, which gave us the possibility to stratify by era. However, the current study should also be interpreted in light of several limitations. First of all, the main limitation is the single-centre setting; as such, centre-specific bias could be large, and findings need to be correlated with other large centre data. Furthermore, the retrospective nature may limit the generalisability of the results. As with all retrospective studies using large databases, there is the possibility of potential unmeasured confounders that have not been accounted for. In particular, our work was limited by the unavailability of data in some patients (especially the earliest era) and specific data regarding early postoperative complications and cause of death. The latter was difficult to retrieve because the death of our patients mainly occurred in other centres distant to the transplant centre and details about cause of death were not always reported back to our centre. Furthermore, the incidence of CLAD might be underestimated and accurate phenotyping over all eras according to the latest guideline was not possible as we were unable to review pulmonary function tests and CT in retrospect. Second, it has become very clear that telomeropathies may negatively impact post-transplant complications and survival in a subgroup of IPF and other patients with ILD.39 40 Unfortunately, we currently do not have the ability to routinely measure telomere lengths or common telomerase mutations at our centre.
In conclusion, in patients transplanted for end-stage ILD, older age and fibrotic NSIP correlated with poorer survival post-transplant. This should not preclude these patients from undergoing a lung transplant, as this is often the best and perhaps only treatment modality to improve survival and quality of life of these patients. It does, however, highlight that survival after lung transplantation is affected by many reasons, making it challenging to select transplant candidates who may benefit most from it.
Moreover, our data support better survival after BLT compared with SLT in younger patients, which was not seen in older patients and the overall cohort. However, as previous studies have shown, there is still a lack of high-quality evidence to recommend one type of organ transplant over another. Although it seems plausible that the advantage of BLT over SLT disappears in elderly candidates, demonstrating that SLT is still a reasonable option and may even be preferred based on donor availability and ethical considerations in a certain subset of patients with ILD in some centres.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request and are not publicly available.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Dr. Zhe K Law (Department of Medicine, National University of Malaysia, Kuala Lumpur, Malaysia) for his help with the statistical analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SWL and SB are joint first authors.
AJF and GM are joint senior authors.
Contributors SWL: performed research, collected and analysed the data, wrote the manuscript; SB: checked and analysed the data, wrote the manuscript; JLL and AN: critically revised the manuscript; AJF and GM: guarantor, coordinated and designed the research, critically revised the manuscript.
Funding Following authors are supported by a research fellowship, but received no specific funding for the current study: SB is funded by the Paul Corris International Clinical Research Training Scholarship; AJF is deputy director of the NIHR Blood and Transplant Research Unit in Organ Donation and Transplantation at the Universities of Cambridge and Newcastle.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.