Article Text

Abstract
Objective The renin–angiotensin system (RAS) has been shown to play a role in the pathogenesis of chronic obstructive pulmonary disease (COPD) because of the inflammatory properties of the system. Many patients with COPD use RAS-inhibiting (RASi) treatment. The aim was to determine the association between treatment with RASi and the risk of acute exacerbations and mortality in patients with severe COPD.
Methods Active comparator analysis by propensity-score matching. Data were collected in Danish national registries, containing complete information on health data, prescriptions, hospital admissions and outpatient clinic visits. Patients with COPD (n=38 862) were matched by propensity score on known predictors of the outcome. One group was exposed to RASi treatment (cases) and the other was exposed to bendroflumethiazide as an active comparator in the primary analysis.
Results The use of RASi was associated with a reduced risk of exacerbations or death in the active comparator analysis at 12 months follow-up (HR 0.86, 95% CI 0.78 to 0.95). Similar results were evident in a sensitivity analysis of the propensity-score-matched population (HR 0.89, 95% CI 0.83 to 0.94) and in an adjusted Cox proportional hazards model (HR 0.93, 95% CI 0.89 to 0.98).
Conclusion In the current study, we found that the use of RASi treatment was associated with a consistently lower risk of acute exacerbations and death in patients with COPD. Explanations to these findings include real effect, uncontrolled biases, and—less likely—chance findings.
- COPD epidemiology
- COPD Exacerbations
- COPD Pathology
- COPD Pharmacology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The renin–angiotensin system (RAS) has been shown to play a role in the pathogenesis of chronic obstructive pulmonary disease (COPD) because of the inflammatory properties of the system. Yet, the association between the use of RAS acting agents and the risk of severe exacerbations has not previously been systematically explored in patients with severe/very severe COPD.
WHAT THIS STUDY ADDS
We found that the use of RAS-inhibiting treatment was associated with a consistently lower risk of acute exacerbations and death in patients with COPD.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
It seems very unlikely that treatment with RAS-inhibiting drugs should increase the risk of exacerbations in patients with COPD and our finding is biologically plausible; however, it should be interpreted with caution because of the observational nature of the data. Randomised controlled trials should be performed to clarify whether the use of RAS-inhibiting treatment is causative for such a protective effect.
Background
Chronic obstructive pulmonary disease (COPD) is a leading cause of chronic morbidity and mortality worldwide.1 A key feature of the disease is airway obstruction due to inflammation in the airways, breakdown of the lung parenchyma and loss of elastic recoil.2 Acute exacerbations of COPD (AECOPD) are often related to an increase in both respiratory and systemic inflammation,3 4 and the high mortality of COPD is associated with exacerbations.5
The renin–angiotensin–system (RAS) has—other than the well-known role in blood pressure homeostasis—shown to participate in the pathogenesis of pulmonary and extra pulmonary manifestations of COPD.6 More specifically, the system affects the development of pulmonary fibrosis, pulmonary hypertension and skeletal muscle dysfunction, which are all observed in COPD.6–9
Angiotensinogen is converted to Angiotensin (Ang) I with stimulation by renin, after which the protease ACE cleaves Ang I to Ang II. Ang II is the central effector molecule in RAS. ACE is present at high concentrations in the lung capillaries, and therefore, the lungs are an important organ in the synthesis of Ang II.10 With stimulation by aminopeptidases, Ang II can further be metabolised to Ang III, IV and V.6 These downstream products of the RAS have been shown to stimulate a proinflammatory response, and thus, the RAS may play a role in COPD exacerbations via its influence on inflammatory processes in the airways. Furthermore, it has been shown that Ang II—through stimulation of both Ang II Type 1 (AT1)-receptor and Ang II Type 2 (AT2)-receptor—mediates the activity of fibroblasts to increase production of collagen, which plays an important role in the pathogenesis of pulmonary fibrosis.6 The RAS may also influence the pathogenesis of COPD by stimulation of proinflammatory mediators such as interleukin-6 (IL-6) and tumour necrosis factor-α (TNF- α).11–13
Previous studies substantiate the theory on the advantage of blocking the RAS in persons with COPD. Various observational studies have indicated that RAS-inhibiting (RASi) treatment of patients with COPD reduce all-cause mortality as well as myocardial infarction.14–16 Furthermore, one of these studies demonstrate a reduced risk of AECOPD in patients with COPD who use RASi, but it is unclear whether this effect is caused by the RAS acting agents or by the concomitant statin treatment.15
We hypothesised that the use of RASi, either by treatment with an ACE-inhibitor (ACEi) or an angiotensin II receptor blocker (ARB), is associated with a reduced risk of AECOPD.12 17 The aim of the current study was thus to determine the association between treatment with RAS acting agents and the risk of acute exacerbations and mortality in patients with severe COPD.
Materials and methods
Study design
This study was a national observational cohort study based on data from Danish registries. The period of inclusion was from 1 January 2010 to 31 December 2018 and patients were followed 1 year after inclusion. Study entry was defined as the first outpatient clinic visit registered in Danish Registry of COPD (DrCOPD).
The primary outcome was severe exacerbations of COPD within 12 months after study entry or death in the same period. Death was included as a primary outcome as it is a prominent competing risk in patients with COPD. The secondary outcome was moderate exacerbations of COPD. Severe exacerbations were defined as leading to hospital admission, whereas moderate exacerbations were defined as leading to the patient receiving a prescription of oral corticosteroids and/or antibiotics, following the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification.1 Oral corticosteroids were defined as prednisolone. Respiratory antibiotics were amoxicillin, amoxicillin with clavulanic acid, benzylpenicillin, phenoxymethylpenicillin, moxifloxacin, azithromycin, roxithromycin, clarithromycin, doxycycline and ciprofloxacin. All Anatomical Therapeutic Chemical classification codes are presented in online supplemental appendix 1.
Supplemental material
Reporting adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.18 A study protocol was web published prior to completing the study.19
Data sources
Three registries were used in the study. Each Danish citizen is given a personal identification number at birth, allowing linkage between registries. The used registries are as follows:
The DrCOPD20 is a national database, which contains information on health status and treatment of patients diagnosed with COPD in Denmark. From DrCOPD, we obtained inclusion date, forced expiratory volume in 1 s (FEV1), Medical Research Council dyspnoea scale, body mass index (BMI), tobacco history, age, sex and—if relevant—death date of the patients.
The Danish National Health Service Prescription Database,21 is administered by The Danish Health and Medicines Authority and it contains information on all prescriptions dispensed in Denmark. We retrieved data on date of dispensations, as well as dose and strength of prescriptions.
The Danish National Patient Register (DNPR)22 is also administered by The Danish Health and Medicines Authority. The database contains information on all hospital admission and outpatient clinic visits registered with the International Classification of Disease 10th revision (ICD-10 codes).
Study population
The participant population for this study includes all patients diagnosed with COPD with an outpatient clinic visit registered in DrCOPD from 2010 to 2018, aged >40 years.
Patients with a malignant cancer diagnosis within 5 years before study entry (except non-melanoma cancer of the skin) were excluded from the study. Furthermore, we excluded participants with chronic renal failure, type 1 diabetes mellitus with renal complications and typ -2 diabetes mellitus with renal complications. Patients diagnosed with heart failure in the DNPR and patients with prescriptions of furosemide, carvedilol or bumetanide within the preceding twelve months were also excluded from the study to reduce confounding by indication. Heart failure is the main indication for prescribing these drugs, which enables us to also exclude the patients with heart failure not diagnosed in the DNRP. All diagnoses are presented by ICD-10 codes in online supplemental appendix 2.
Supplemental material
Patient and public involvement
No patients were involved in the design or conduct of this study.
Permission for our use of registry data was given by the Danish Data Protection Agency. Such retrospective use of data does not require ethical permission or patient consent in Denmark.
Statistical analyses
Baseline characteristics were presented as frequencies and proportions for the active comparator and unmatched populations. A p<0.05% was considered statistically significant.
We performed an ‘active comparator analysis’ as our main analysis, which provides an overlap of measured characteristics between the compared groups and thereby reduces the risk of unmeasured confounding.23 24 Bendroflumethiazide was used as the active comparator because its primary indication—such as ACEi and ARB—is hypertension, which enables us to create two comparable groups. All these three drugs (bendroflumethiazide, ACEi and ARB) are used as first-choice drugs for arterial hypertension in our country.25 26
For this analysis, we propensity-score matched the population on GOLD stage (1–4), age group (1–4), sex (male/female), BMI group (1–5), smoking history (group I: active smoker/group II: previous smoker or never smoker), number of AECOPD 12 months prior to baseline (0, 1, >2), inclusion year, Charlson Comorbidity Index 10 years prior to inclusion date (group I: 0–2 points=mildly ill, group II: 3–4 points=moderately ill, group III: >5 points: severely ill,27 28), prescription of long-acting β2-agonists (LABA), long-acting muscarinic antagonists (LAMA) and inhaled corticosteroids (ICS) 1 year before inclusion in the study. Other than that, the participants were matched on having at least two prescriptions of an RASi 1 year before study entry or at least one prescription of bendroflumethiazide 1 year prior to inclusion.
For both groups separately, we calculated the incidence rates (IRs) of AECOPD 1 year before starting the treatment and 1 year after to use the participants as their own control.
A propensity score-matched cohort was created by matching the entire, eligible population on the same variables as described for the active comparator analysis. We then used an unadjusted Cox proportional hazards regression model to assess the outcome of the propensity score-matched population. Lastly, a multivariable Cox proportional hazards model was performed on the entire, unmatched population, which was adjusted for the same variables as matched for in the previously described analyses.
Model control of the assumptions for the Cox proportional hazards model was performed and continuous variables, which failed linearity, were categorised. No interaction between time and exposure was found, confirming the assumption of hazard proportionality.
Missing values for FEV1, smoking history and BMI variables (we only had missing data for these three variables) were handled with stochastic regression imputation. In cases where this was not possible, we performed multiple imputation to avoid selection bias.
Data management and statistical analyses were performed using Statistical Analysis Software V.9.4 (SAS Institute). Multiple imputation and subsequent analyses were performed in R studio V.1.4.1106 using the SMCFCS V.1.6.1 and MITOOLS V.2.4 packages. The settings in SMFCS were 50 imputations, 10 iterations and a rejection limit of 10 000. Propensity score matching was performed in the SAS PSMATCH-procedure based on the logit of propensity score, with a calliper of 0.25 and using an extended common support region. In all survival analyses, ties were handled with the Efron method.
Results
Study participants
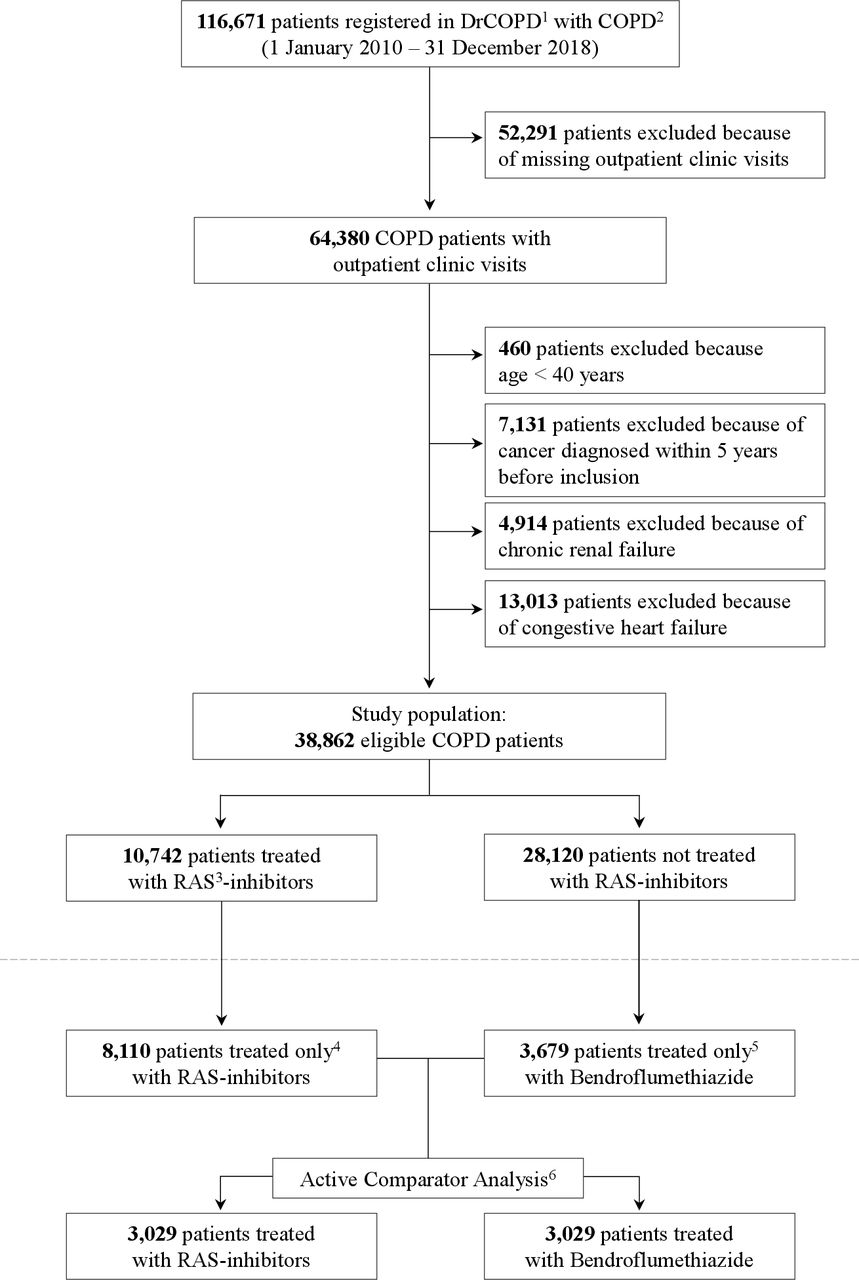
We identified 116 671 patients registered in DrCOPD, of which 38 925 met all criteria for inclusion in the study, as seen in figure 1. Of these patients, 10 742 were exposed to an RASi. The baseline characteristics of the individuals in the unmatched population are presented in table 1 for both the exposed and the non-exposed group.
Baseline characteristics
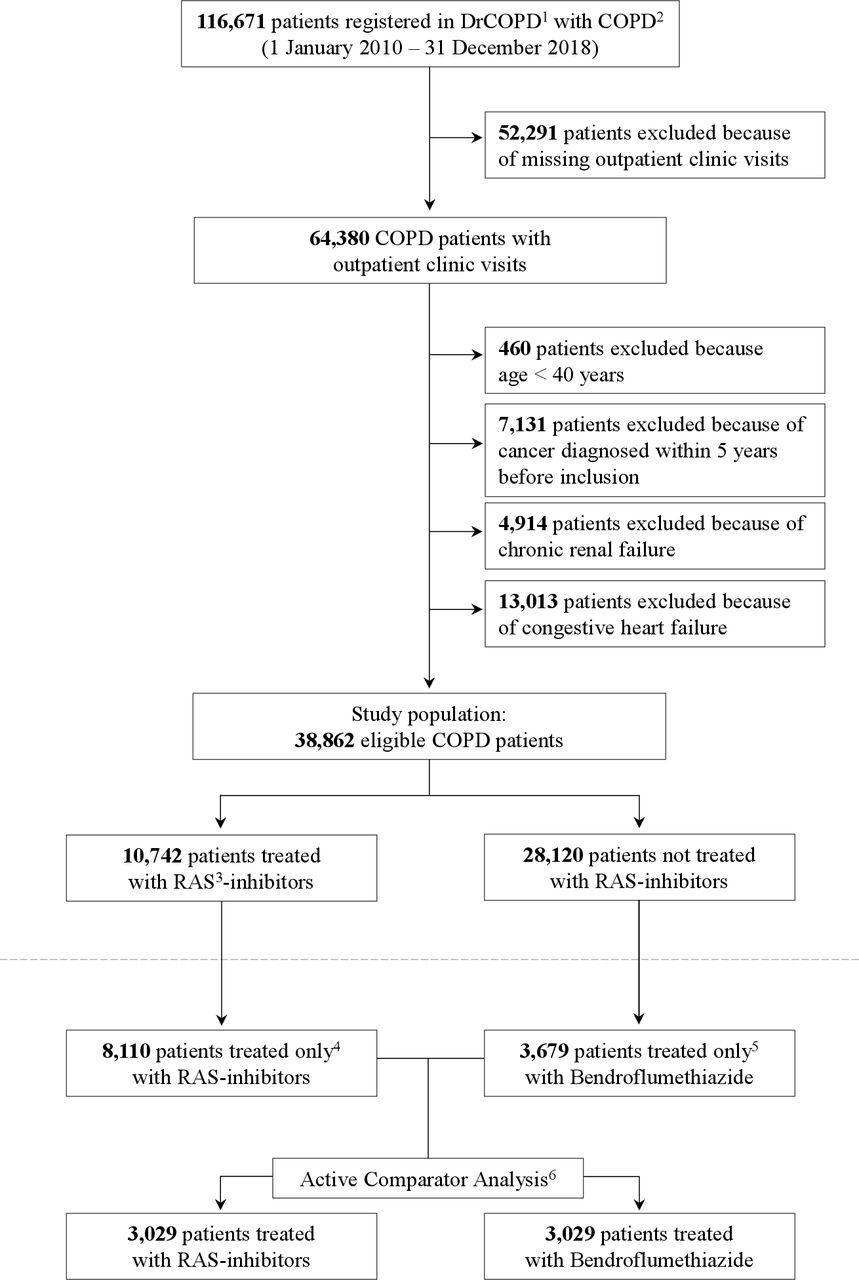
Study flowchart. 1. Danish register of chronic obstructive pulmonary disease; 2. Chronic obstructive pulmonary disease; 3. Renin-Angiotensin-system; 4. not concomitant treatment with Bendroflumethiazide; 5. not concomitant RAS-inhibiting treatment (ACEi/ARB); 6. propensity-score-matched on GOLD Stage, age-group, sex, BMI-group, smoking history, number of AECOPD 12 months prior to baseline, inclusion year, Charlson Comorbidity Index 10 years prior to inclusion date, prescription of long-acting β2-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS) one year before inclusion in the study.
The unmatched population consisted of 15 564 females and 12 556 males in the control group and 5771 females and 4971 males in the group exposed to an RASi. In general, persons in the RASi group had a lower GOLD stage, higher BMI, were less likely to smoke, and had more comorbidities than the control group. Other than that, the two groups were comparable.
Of the complete, eligible population, 6311 patients received bendroflumethiazide, which was the drug used as the active comparator to RASi (n: 10 742). Of the entire population receiving the drugs, 5264 had a prescription of both drugs and were thus excluded from the active comparator analysis. This reduced the numbers to 3679 patients with a prescription of bendroflumethiazide and 8110 patients with a prescription of RASi, as seen in figure 1. Baseline characteristics for both these groups are presented in table 1. In total, 6058 patients were matched on the variables described previously—3029 from each group. We assessed that these groups were large enough for the active comparator to be our primary analysis.
Main outcome analysis
The primary analysis was an active comparator analysis with patients receiving an RAS-active agent compared with patients receiving bendroflumethiazide. Of the people receiving an RASi, 498 had a severe exacerbation of COPD and 286 died with a total of 784 (25.9%) having an event within the following year, whereas 591 of the people receiving bendroflumethiazide had an exacerbation and 299 died in the same period with a total of 890 (29.4%). Treatment with other antihypertensive drugs was balanced between the two groups, with calcium channel blockers as the most frequently used of these drugs. In the RASi group, 39.8% had a prescription of this, compared with 33.4% in the bendroflumethiazide group (table 1). The risk of AECOPD or death after 12 months follow-up was lower for the RASi group compared with the bendroflumethiazide group (HR 0.86, 95% CI 0.78 to 0.95), as presented in figure 2A.
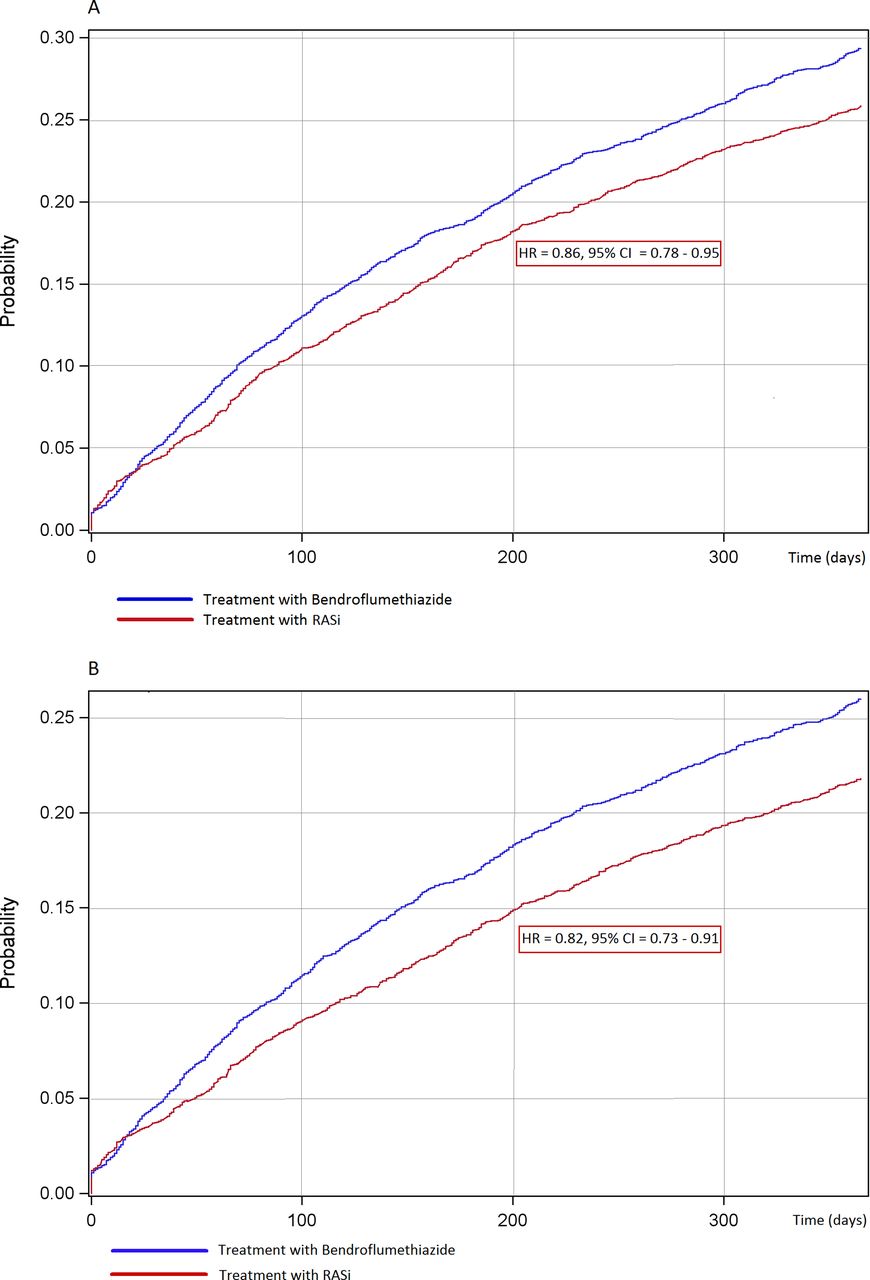
(A) Cumulative incidence function presenting risk of AECOPD or death (hazard ratio (HR) and 95% confidence interval (CI)) within one year with RAS-inhibiting treatment compared to Bendroflumethiazide treatment. (B) Cumulative incidence function presenting risk of only AECOPD (hazard ratio (HR) and 95% confidence interval (CI)) within one year with RAS-inhibiting treatment compared to Bendroflumethiazide treatment. RAS-i, renin–angiotensin system inhibitors.
In a subsequent analysis, we found that the risk of AECOPD isolated within the following year was also significantly lower for the RASi group than for the bendroflumethiazide group (HR 0.82, 95% CI 0.73 to 0.91) (figure 2B).
Sensitivity analyses
An adjusted Cox proportional hazard model was performed on the unmatched population at 12 months follow-up, which was adjusted for the same variables as were used to match in the primary analysis. In the group not exposed to RASi, 6897 (24.5%) patients had an exacerbation or died within the follow-up period, whereas 2455 (22.8%) of the patients who were exposed to RASi had a similar event. Treatment with an RAS-acting agent showed a slight reduction in risk of AECOPD or death (HR 0.93, 95% CI 0.89 to 0.98). The adjusted HRs for all variables are presented in figure 3.

{kind=link}
{kind=link}
{kind=link}
Forest plot presenting risk of AECOPD or death (hazard ratio (HR) and 95% confidence interval (CI)) demonstrated in three different analyses. 1. propensity-score matched on GOLD Stage, age-group, sex, BMI-group, smoking history, number of AECOPD 12 months prior to baseline, inclusion year, Charlson Comorbidity Index 10 years prior to inclusion date, prescription of LABA, LAMA, and ICS one year before inclusion in the study; 2. Angiotensin converting enzyme-inhibitor/Angiotensin II receptor-blocker, at least two prescriptions within the last year; 3. GOLD 1: FEV1 >80% = mild, GOLD 2: 50% < FEV1 < 80% = moderate, GOLD 3: 30% < FEV1 < 50% = severe, GOLD 4: FEV1 < 30% = very severe,[1]; 4. Age group 1 <60 years, group 2 = 60-68 years, group 3 = 78-76 years, group 4 >76 years; 5. BMI group 1 <18.5, group 2 = 18.5-25, group 3 = 25-30, group 4 = 30-35, group 5 >35; 6. 0, 1 or >2 severe exacerbations 12 months before baseline; 7. Charlson comorbidity index, Group I: 0-2 points = mildly ill, group II: 3-4 points = moderately ill, group III: > 5 points: severely ill,[29]; 8. prescription if long-acting β2-agonists 12 months before baseline; 9. Prescription of long-acting muscarinic antagonists 12 months before baseline; 10. prescription of inhaled corticosteroids 12 months before baseline
The propensity score matching of the entire population created two comparable groups consisting of 8734 patients each: one group receiving RASi and one group not receiving the drugs. The sensitivity analysis of the propensity-score-matched population showed similar results as the primary, active comparator analysis (HR 0.89, 95% CI 0.83 to 0.94).
We also analysed the IR of AECOPD for both the RASi group and the Bendroflumethiazide group 1 year before versus after initiating the treatment. The risk in both treatment groups proved to be higher in the succeeding year than in the time before starting treatment (RASi IR ratio (IRR)=1.77, bendroflumethiazide IRR=1.53), as expected due to the increased risk of events in new users of a drug.
Discussion
In this nationwide, registry-based cohort study, we found that use of RAS-acting agents was associated with decreased risk of severe exacerbations of COPD or death 12 months after initiation of treatment, both in the primary active comparator analysis and in the propensity matched analysis. Similar results were evident in the adjusted Cox proportional hazards regression.
The association between the use of RAS-acting agents and the risk of severe exacerbations has not previously been systematically explored in patients with severe/very severe COPD. Previous studies have investigated the effect of RASi in combination with statins,14 15 or only specifically ARB,16 29 with mortality and myocardial infarction as primary outcomes and a shorter follow-up period. Furthermore, the statistical power in these studies was presumably low due to small sample sizes.
Only one study investigated AECOPD as outcome, and they found results similar to ours. However, this study had an older population (>65 years), their primary outcome was all-cause mortality and myocardial infarction as well as exacerbations, and they had a longer follow-up period.15
There is an ongoing discussion on whether the use of statins play a role in the prevalence of AECOPD.30 31 However, in this study, there was only approximately 13% absolute difference in statin user prevalence between the RASi group and the bendroflumethiazide group in the main analysis (table 1). The relative risk reduction of statins would thus not be able to drive a difference in our results. Neither the active comparator analysis nor the adjusted Cox analysis was adjusted for the use of statins. Meanwhile, the signal on the protective effect of RASi treatment was strongest in the active comparator analysis, which indicates that adjusting for the use of statins would not make a significant difference in the results.
To our knowledge, this study is the first large observational nationwide registry study that investigates the impact of RASi treatment on severe and moderate exacerbations of COPD in a real-life outpatient cohort with 12 months follow-up. The study had a large population size with almost 40 000 patients meeting all inclusion criteria, of whom more than 10 000 were exposed to the drugs of interest. All patients were registered in national Danish registries, which allowed us to control for important confounders and thereby reduce the risk of bias and ensure no loss to follow-up. Furthermore, all patients with cardiac failure were excluded from the study before the primary analysis was conducted, which eliminated an important source of confounding in patients with COPD. DrCOPD enabled us to ensure a correct COPD diagnosis, made by a respiratory specialist and verified at annual outpatient visits with spirometries, thereby reducing the risk of misclassification bias. For our primary analysis, we used bendroflumethiazide as an active comparator, which reduces the risk of unmeasured ‘new user’ bias. For the same reason, we propensity-score matched the sensitivity analysis on several known predictors of the outcome and the survival analysis was adjusted for the same variables. Of note, the matching, both in the primary active comparator analysis and in the propensity-score-matched cohort, seemed quite balanced on key confounders. In the primary analysis, the effect was very similar on AECOPD alone as it was on AECOPD and all-cause mortality, which validates our findings and substantiates their relevance to pulmonary disease.
However, there are also limitations to this study. First, despite having adjusted the analyses for known confounders, the survival analysis suggested an increased risk of AECOPD with the use of LABA, LAMA and ICS, which indicates some residual bias by indication, since at least LAMA and ICS are documented to reduce AECOPD.32–34 Second, it was not possible, qua the registry design, to monitor the patients’ adherence, as exposure to the drug was defined by a collected prescription. This leaves some uncertainty as to whether patients used the medication, which is an inborn error in the design of the retrospective registry study. However, the uncertainty is limited because we know the prescriptions are collected, which makes it very likely that the drugs were also used by the patients. Non-adherence would lead to a conservative bias since actual non-users would be classified as users. Third, the IRs implied an increased risk of AECOPD after initiating treatment with RASi compared with before exposure to the drug. But a similar result was evident with exposure to bendroflumethiazide, and the explanation is probably the increased risk of events in a new user of a drug as well as the fact that the risk of a patient with COPD having an exacerbation simply increases over time as the disease progresses. This is the main reason for performing the active comparator analysis. Fourth, we acknowledge that finding the perfect drug to use as active comparator is very challenging, as no two treatment groups are completely alike. We have accommodated this issue by using two drugs that are both first-line drugs in treatment for hypertension. Furthermore, all patients that could have other indications for the treatment (renal failure and heart failure) were excluded from the study before performing the primary analysis.
In conclusion, we observed a consistent signal suggesting an association between treatment with an RASi and a reduced risk of acute exacerbations and death in patients with COPD. Our data thus support the safety of such very frequently used drugs among people with COPD. This finding is biologically plausible; however, it should be interpreted with caution because of the observational nature of the data. Randomised controlled trials (RCTs) can clarify the degree of residual confounding and whether the use of RASi treatment is actually causative for such a protective effect. This remains an unanswered hypothesis, but it seems very unlikely that treatment with drugs inhibiting the RAS should increase the risk of AECOPD.
Since both COPD and treatment with RASi are very frequent, we argue that the size of potential benefit is large enough that such RCTs should be performed.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but permission for our use of registry data was given by the Danish Data Protection Agency. Such retrospective use of data does not require ethical permission or patient consent in Denmark. Such retrospective use of data does not require ethical permission or patient consent in Denmark.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors FV carried out the statistical analyses and wrote the manuscript with support from CKH, PK and CH. TB-S, RS, SK, OH, LP, TKL, TWK and KGS contributed with input to the manuscript. JE and PS helped supervise the project. J-USJ conceived the original idea, provided the data, and supervised the data processing, interpretation and writing of the study. FV acts as gauntor and takes responsibility for the finished work.
Funding This study was funded by Grant no. NNF20OC0060657 from the Novo Nordisk Foundation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.