Article Text

Abstract
Background Preoperative bronchoscopic tumour ablation has been suggested as a beneficial treatment for bronchopulmonary carcinoid tumours, although data regarding its effects and long-term outcome are lacking.
Methods In our case-matched cohort study with 208 patients with bronchopulmonary carcinoid tumours we investigated the role of preoperative bronchoscopic interventions before subsequent surgery and analysed the safety of this Procedure of Endobronchial Preparation for Parenchyma-sparing Surgery (PEPPS) based on metastasis and recurrence rates as well as survival data from 1991 to 2010. The subsequent surgery was classified into parenchyma-sparing procedures and classical lobectomies, bilobectomies and pneumonectomies. Data were obtained from the tumour registry and medical reports. Outcomes were the frequency of parenchyma-sparing surgery after bronchoscopic treatment as well as rates of metastasis, recurrence and survival.
Results 132 of 208 carcinoids were located centrally. Among them, 77 patients could be recanalised preoperatively. After bronchoscopic preparation, the rate of subsequent parenchyma-sparing surgery methods was higher (p=0.021). The effect was measured by the number of segments removed. The 10-year survival rate was 89% (typical carcinoids) and 68% (atypical carcinoids), respectively. After applying PEPPS, long-term survival was slightly higher (p=0.23). Metastasis and recurrence rates showed no relevant differences between the bronchoscopically treated or non-treated groups, or between the two types of surgery classes or between the PEPPS and non-PEPPS groups.
Conclusions After preoperative bronchoscopic treatment, parenchyma-sparing surgery techniques can be applied more frequently. Furthermore, we detected no negative effects after PEPPS based on metastasis, recurrence and survival rates.
- Thoracic Surgery
- Bronchoscopy
- Lung Cancer
- Equipment Evaluations
- Clinical Epidemiology
- Imaging/CT MRI etc
- Pneumonia
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Thoracic Surgery
- Bronchoscopy
- Lung Cancer
- Equipment Evaluations
- Clinical Epidemiology
- Imaging/CT MRI etc
- Pneumonia
Key messages
More than 60 percent of all carcinoid tumors of the lung were found growing in a central position with a potential connection to the bronchopulmonary main system that makes them potentially accessible for bronchoscopical intervention.
After endoluminal tumor ablation, a parenchyma-sparing surgery procedure was applied more frequently in bronchopulmonary carcinoid tumors.
A combination of bronchoscopical carcinoid ablation and subsequent parenchyma-sparing surgery (called PEPPS – Procedure of Endoluminal Preparation for Parenchyma-sparing Surgery) does not seem to have a negative impact on survival, local recurrence and/or distant metastasis rates in the long-term.
Introduction
Pulmonary carcinoid tumours have been classified as neuroendocrine neoplasms and account for 1.2% of all lung tumours with increasing incidence.1 They are further classified into typical carcinoids (TCs) and the more aggressive atypical carcinoids (ACs), which show a faster growth pattern as well as higher recurrence, and metastasis rates.2 ,3
Carcinoids often grow in a central position involving the main bronchi where they cause luminar obstruction followed by retention pneumonia in distal parts.4 ,5 Owing to this chronic or recurrent infection, irreversible tissue destruction can arise, requiring more aggressive surgical procedures.6 Although surgical tumour resection remains the most important standard therapy option for these tumours,5 there has been some discussion as to whether it is the best approach.7 ,8
Nevertheless, based on their central growth, carcinoids are often resectable by bronchoplastic surgery techniques.4 ,5 This strategy is not only known to spare parenchyma but also has lower complication rates as well as lower morbidity and mortality and an excellent long-term survival.5 ,9 Their location often makes them accessible for bronchoscopic diagnosis and intervention. Whereas, initially, bronchoscopic tumour resection was used only in inoperable10 or palliative patients,11 endoluminal intervention is now often used for tumour debulking and bronchus recanalisation, which allows resolution of retention pneumonia.5
In this study, we investigated whether a preoperative bronchoscopical intervention for tumour ablation/reduction can increase the number of parenchyma-sparing surgery techniques in centrally located typical and atypical pulmonary carcinoid tumours and how safe this approach is long term. We called this approach Procedure of Endobronchial Preparation for Parenchyma-sparing Surgery (PEPPS).
Patients and methods
Approval for this work was obtained from our institutional ethics committee (Project 363-08).
In this case-matched study, we retrospectively analysed records and examinations of patients treated for bronchopulmonary neuroendocrine carcinoid tumours at the Center for Thoracic Surgery of the Asklepios lung centre Munich-Gauting, Germany, from January 1991 to January 2010. All data were anonymised. Subsequently, the results were matched with data from the Tumor Registry of the Tumor Center, Munich. Only patients whose tumour was definitely classified by histopathology as TC or AC according to WHO criteria12 were included.
Standard preoperative evaluation included clinical and radiological investigations (chest X-ray, chest and abdominal CT) and neuroendocrine blood and urine values as well as nuclear medicine imaging. Tumours were classified as ‘central’ if radiologically located close to the main bronchi with a presumable connection to the endobronchial main system, or if visualised directly at bronchoscopy.
All patients underwent diagnostic bronchoscopy including endobronchial ultrasound for tumour evaluation and biopsy for histological classification into subtypes, if technically feasible. An interventional tumour ablation for bronchus recanalisation by laser, cryo or mechanical treatment was also performed whenever possible, usually in the same or subsequent session(s). After this intervention, we administered specific antibiotic therapy to treat retention pneumonia, if indicated. Infection-free status was measured clinically and by inflammatory markers.
Subsequent operative procedures were further classified as extensive ‘class 1’ procedures (such as lobectomies, bilobectomies and pneumonectomies) and parenchyma-sparing ‘class 2’ resections (sleeve lobectomies, main bronchus sleeve resections and segment resections). A lymph node sampling for pathological assessment was performed intraoperatively, and if lymph nodes were positive (or inconclusive) for tumour cells, a radical lymph node dissection was added. Excluded were patients with whom a tumour was not detectable in histological processing after surgical resection and preoperative bronchoscopic treatment.
Follow-up information was obtained after consent from patients’ re-examinations or records of the Tumor Registry Munich, medical records, phone interviews, primary physician, and specialist contacts. The information contained metastasis, recurrence and survival rates and data from operative reports, pathological records and bronchoscopic interventions as well as clinical information. Overall survival time for all patients started at the date of the first bronchoscopic or surgical intervention.
The primary outcome was the frequency of parenchyma-sparing surgery after bronchoscopic treatment with secondary outcomes including rates of metastasis, recurrence and survival.
Statistical analysis: The distribution of qualitative data is presented by absolute and relative frequencies. Continuous data is described by mean (±SD) when normally distributed and by median (range) in any other case. Differences in groups were tested by Fisher's exact test or χ2 test, depending on the cell count of corresponding contingency tables. Likewise, the t test or Mann–Whitney U test was used to compare samples of normally and non-normally distributed data. Numbers of resected segments were compared by means of Poisson regression analysis. Survival and time-to-event data was assessed by Kaplan–Meier estimates and compared by use of the log-rank test. All statistical tests were performed in an exploratory manner on a two-sided 5% significance level using the software packages PASW Statistics (V.17.0.2; SPSS, IBM), R (V.2.10.1; R Foundation for Statistical Computing) and GraphPad Prism (V.6.0b; GraphPad Software).
Results
Demographics
Overall, 59% of our patients reported tumour-related or obstructive symptoms such as retention pneumonia with cough, fever and dyspnoea or haemoptysis, pain or a carcinoid syndrome. On the basis of CT and bronchoscopic findings, 132 of 208 carcinoids (63.5%) were located centrally. Among them, there were 67 females (50.8%) and 65 males (49.2%) with a median age of 55 years (range 17–79 years). The median follow-up, computed by the inverse Kaplan–Meier method, was 70 months (range 1–222). Table 1 summarises the demographic, clinical and histopathological data of patients.
Clinical and histopathological characteristics of 132 patients with centrally located typical and atypical pulmonary carcinoid tumours
Bronchoscopy
The patient regime is shown in figure 1; 77 patients (58.3%) with a centrally localised carcinoid tumour underwent a preoperative interventional bronchus recanalisation with subsequent antibiotic treatment. The remaining patients could not be treated bronchoscopically due to a high risk of bleeding or because the tumour was inaccessible in the endobronchial system. In one case, a serious bleeding occurred in a female patient with a TC during bronchoscopic recanalisation, requiring a subsequent surgical intervention. Overall, this patient had no increased morbidity in the observation period.
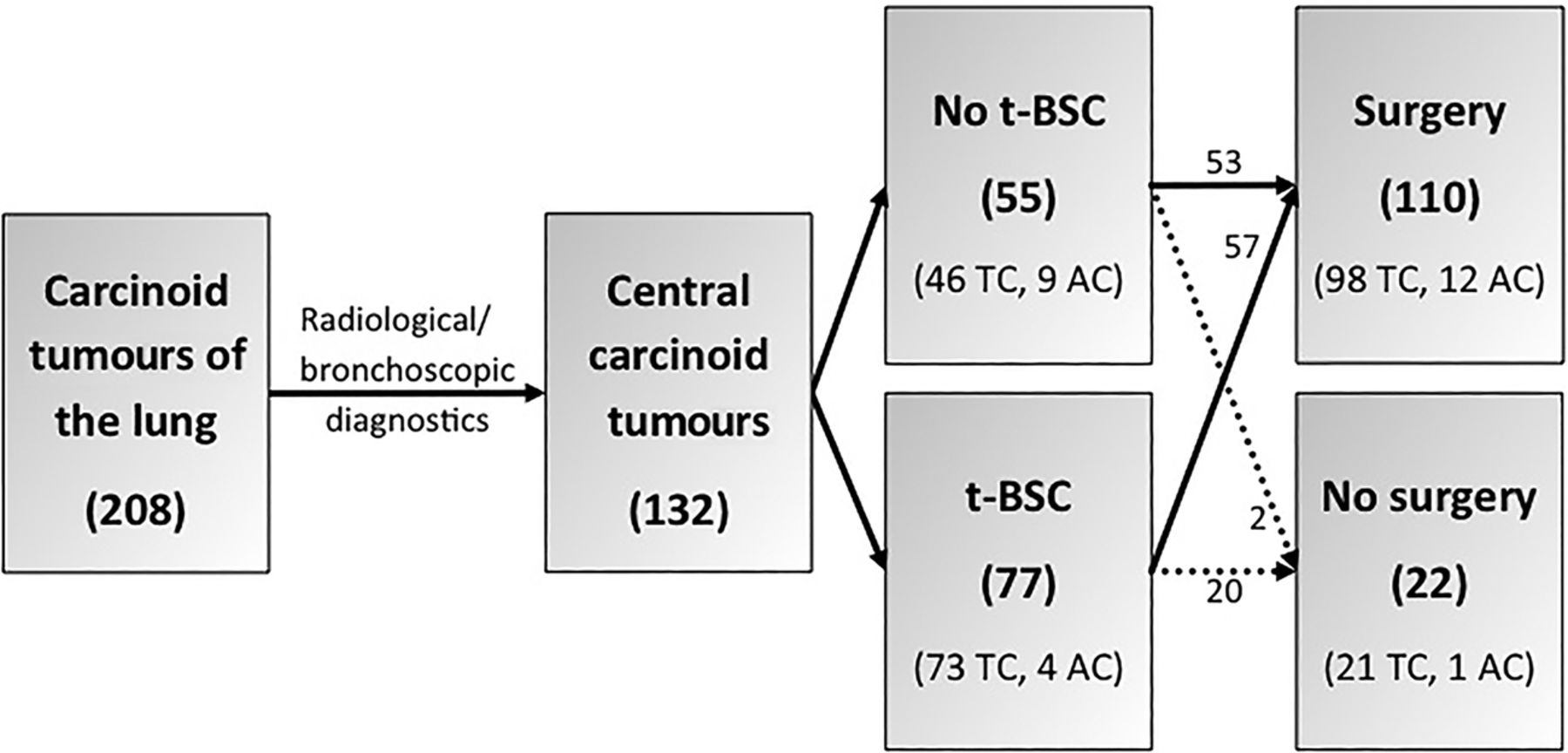
Patient regime (t-BSC, therapeutic/interventional preoperative bronchoscopy; TC, typical carcinoid; AC, atypical carcinoid). Absolute numbers of patients are shown within the groups.
Surgery
Surgery was performed in 110 patients (83.3%), who were further investigated in this study. The remaining 22 patients were either inoperable due to an independent heart disease or a second malignancy (n=7).
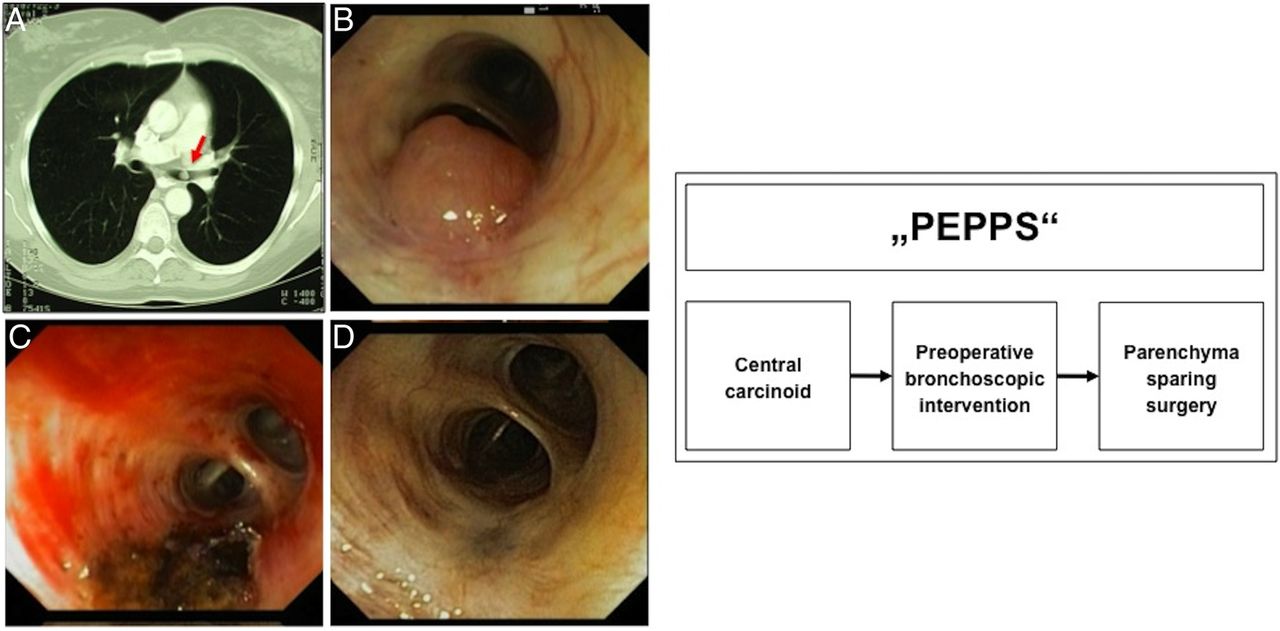
Prior to surgery, 57 of these patients (51.8%) received the preoperative bronchoscopic treatment for tumour reduction. Images from PEPPS are shown in figure 2. Surgery was initiated after a median of 20 days (range 0–270). 49 patients (44.5%) received a class 1 resection (40 lobectomies, 5 bilobectomies, 4 pneumonectomies) and 61 patients (55.5%) received a class 2 resection (25 sleeve lobectomies, 16 main bronchial sleeve resections and 20 segment resections; figure 3). No operative or postoperative mortality was seen.
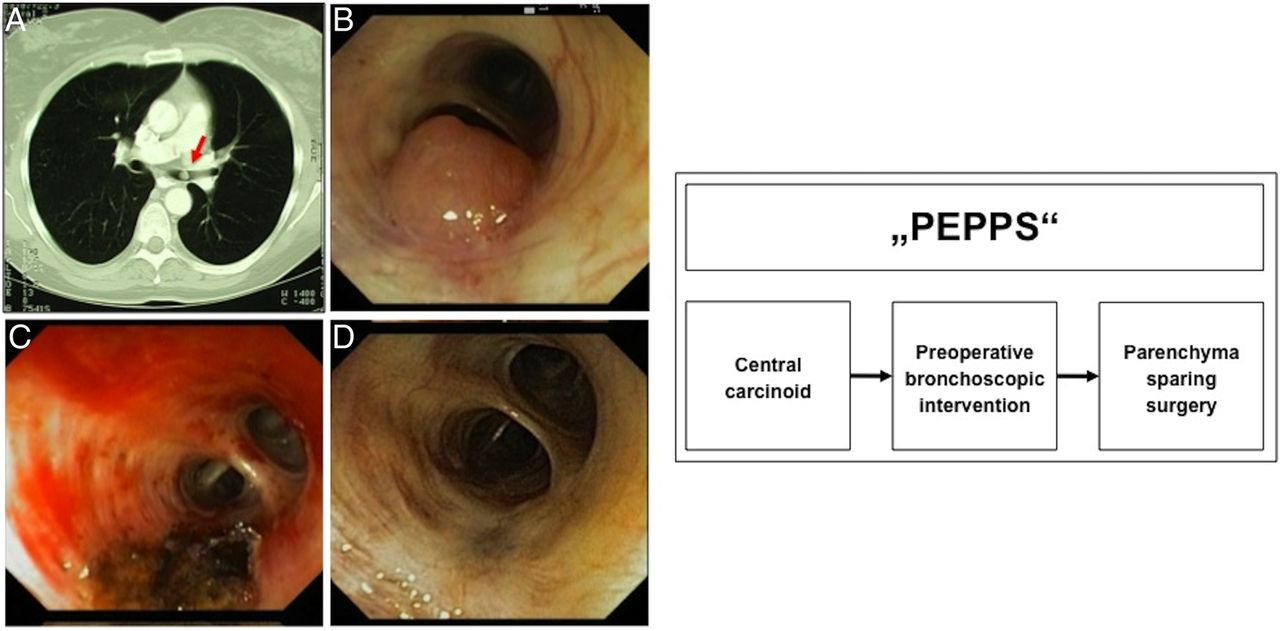
Procedure of Endobronchial Preparation for Parenchyma-sparing Surgery (“PEPPS”). (A) Centrally located, endoluminal growing carcinoid tumour, diagnosed by CT. (B) Endoscopic view of a bronchus obstructing carcinoid tumour in the medial lobe bronchus before segment 4/5. (C) Bronchial view immediately after cryoablation and laser intervention. (D) The same bronchus in a bronchoscopic control 2 months after intervention before surgery.

Sleeve resection, surgical and pathological specimen. (A) Intraoperative view of a carcinoid tumour (black arrow) in the right main bronchus in a sleeve resection. (B) Resected sleeve containing tumour.
In class 1 resections, a mean of 4.8 segments (SE±0.3; 95% CI 4.2 to 5.5; range 2–10) had to be removed whereas only 1.8 segments in class 2 resections (SE±0.2; 95% CI 1.5 to 2.2; range 0–6; p<0.001; see table 2).
Applied surgery classes and resected segments
After preoperative bronchoscopic treatment, the rate of subsequent class 2 surgical resections was higher compared with the procedure without prior interventional tumour reduction (67% vs 43%; p=0.021; table 3).
The use of parenchyma-sparing (class 2) surgery after preoperative bronchoscopic recanalisation in absolute and relative numbers
Pathology
A definitive pathological diagnosis was feasible in all 110 patients after surgery. According to the histological findings, there were 98 patients with TC tumours (89%) and 12 with AC tumours (11%). AC tumours were bigger than TC tumours (3 (2–4) vs 2 (0–5) cm; p=0.009). An exophytic growth was observed in 61% of TC and 33% of AC tissue. None of the patients who were treated by preoperative bronchoscopic intervention followed by subsequent class 2 surgery turned out to have an AC tumour. Pathological findings are shown in table 1.
Safety
Overall survival curves for the patients classified according to the pathological tumour entity are shown in figure 4A. 11 patients died during our follow-up period. The 10-year survival was 89% (TC) and 68% (AC; p=0.046). The 15-year survival was still 85% (TC) and 68% (AC). Moreover, figure 4B shows a slightly higher survival in patients who underwent PEPPS compared with patients without PEPPS, although this difference was not significant. The 15-year survival rate was 96% after PEPPS and 81% without PEPPS.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier estimates of survival between carcinoid entities (A) and procedures applied (B) (PEPPS, Procedure of Endobronchial Preparation for Parenchyma-sparing Surgery).
Metastasis and local recurrence rates did not differ considerably between the preoperative bronchoscopically treated or non-treated group (p>0.999; table 4). Furthermore, an incomplete bronchoscopic tumour ablation seemed not to increase these rates. Last, metastasis and recurrence rates did not considerably differ between the parenchyma-sparing and the more aggressive surgery groups as well as between the PEPPS-treated group and the group that did not undergo PEPPS.
Distant metastasis and local recurrence rates in dependence on interventional bronchoscopy, radicality, surgical procedure and Procedure of Endobronchial Preparation for Parenchyma-sparing Surgery (PEPPS) in relative and absolute numbers
Between the PEPPS and the non-PEPPS group, there were no relevant differences in sex (55% vs 51% females; p=0.842), median tumour size (2 (0–5) vs 3 (1–4) cm; p=0.109) and growth pattern (43% vs 57% exophytic growth; p=0.144).
Discussion
Typical and AC tumours of the lung are malignant neuroendocrine neoplasms.2 Our epidemiological data are fairly comparable to those previously reported.13 ,14 The median age was 55 years. Both genders are affected equally.15
Similar to the literature, 90% of all carcinoids turned out to be TCs; the remaining 10% were classified as ACs.4 ,16
Although the prognosis of lung carcinoids is better compared to carcinoma,17 the mainstay in most cases remains a complete surgical resection.18 Some authors recommend the implementation of parenchyma-sparing resections,6 ,19 which are reported to give more quality of life and a lower complication and morbidity rate without worsening the outcome.3 ,5 ,20
The majority of carcinoids, especially TCs, grows centrally and invades one of the bigger bronchi,5 ,7 ,16 which generally makes them bronchoscopically accessible. Our data with 63.5% of carcinoid tumours located centrally confirm these findings. Therefore, a preoperative intervention is favoured by some authors to prepare for parenchyma-sparing surgery.6 ,19 Concerning this fact, assessment of intraluminal versus extraluminal growth may be of high importance for successful bronchoscopic treatment.21
PEPPS is aimed at ablating the tumour endoluminally and recanalising the bronchus, to improve the patient's condition in case of retention pneumonia before surgery.21 It does not seem to make any difference which kind of bronchoscopic ablation technique is used.22
In 58.3% of our patients with a centrally localised carcinoid tumour, the neoplasm was ablated bronchoscopically. In the remaining patients, the tumour was either not accessible interventionally or the risk of major bleeding was judged to be too high due to a profuse visible vascularisation. Although there are a few reports of major bleeding, we had only one haemorrhage complication in the course of intervention that needed to be controlled by surgery. So we agree with the majority of reports that preoperative bronchoscopic treatment is a fairly safe procedure with only rare complications.21 ,23
Even though there are some reports on a solely curative bronchoscopic treatment with a good long-term outcome,21 ,24 we preferred the combined PEPPS because subsequent surgery is intended to function as a safety buffer to remove any remaining invasive tumour remnants, especially as carcinoids tend to grow invasively with a large extraluminal portion25 called the iceberg phenomenon.
Another important reason as to why we recommend subsequent surgery, is to confirm tumour-free resection margins by pathology26 as well as to stage regional lymph nodes,27 because there are reports of local tumour recurrence after solely intended curative bronchoscopy.21 ,28 Nevertheless, if the carcinoid tumour is locally limited, for example, to the mucosa, solely curative bronchoscopic treatment offers an option, but further studies are needed to identify the right patients and exclude patients who might not benefit from this procedure due to more invasive tumour growth.
Owing to the central growth of carcinoids, parenchyma-sparing surgery methods are feasible and recommended. Moreover, these techniques not only spare parenchyma to a highly significant extent, as shown in this study, but have lower complication rates at bronchial anastomosis and a lower morbidity and mortality as well as ‘excellent’ long-term survival rates with similar recurrence rates compared with conventional methods.5 ,20 ,29 Furthermore, they are associated with increased lung function and better quality of life compared to lobe resections.29
Nevertheless, there are some authors who recommend more aggressive resections even in well-differentiated carcinoids because of the possibility of lymph node metastasis.7 ,8
On the other hand, some authors recommend parenchyma-sparing methods even in the presence of lymph node metastasis, except for cases with distal necrosis, commonly seen with recurrent or chronic retention pneumonias.28 ,30 A preoperative bronchus recanalisation might help reduce the problems related to pneumonia.
In this study, in class 2 resections, about three times fewer segments had to be removed compared with class 1 resections. We have not found any other study that reported similar findings.
A preoperative bronchoscopy can be used to prepare for parenchyma-sparing surgery.6 ,25 Accordingly, our ability to utilise parenchyma-sparing techniques was significantly increased by performing a preoperative bronchoscopic bronchus recanalisation (67% vs 43%, p=0.021).
Compared with the literature, our study showed a slightly higher percentage (67%) of parenchyma-sparing surgery techniques overall.20 Classical lobectomies, bilobectomies and pneumonectomies were mostly applied to patients who had not been previously recanalised.
Similar to previous reports,5 we had no overall perioperative mortality. Furthermore, there was no significant difference in metastasis and recurrence rates, respectively, based on the surgery class used after up to 19 years of observation period (median life follow-up: 70 months (range 1–222)). Metastasis rates, which count for the most important negative predictive factors, were in the lower range (12.6%) in our patients compared with the literature (5–70%).4 ,31 Even our local recurrence rate of 5% falls in the lower range (5–30%).5 ,16 Moreover, overall survival was consistent with the literature with a significant worse prognostic outcome in AC patients.14 ,27 ,32 The histological subtype has been reported to be the most important risk factor for survival.5 Median survival in TC patients was 198 and 120 months in AC patients. Knowing about the different behaviours, it is very important to differentiate the histological subtypes6 ,17 which is already possible preoperatively with a high accuracy using bronchoscopic biopsies in most of the cases.6 ,21 We consider this important to further plan the right strategy and the extent of surgery.
Moreover, we found a slightly increased survival in patients who were treated with PEPPS compared with the non-PEPPS group (214 vs 176 months). Although this difference was not significant, it underlines the clinical safety of this procedure additionally. Besides our data, we did not find any other publication investigating the effect of a combination of preoperative bronchoscopic treatment and parenchyma-sparing surgery on survival. Furthermore, metastasis and recurrence rates after PEPPS treatment were lower compared with the non-PEPPS group. To compare the PEPPS and non-PEPPS groups, we showed that defined clinical and histopathological criteria were distributed almost equally in both groups, besides the patient’s age. Even metastasis and local recurrence rates behaved similar in both groups.
Based on those facts, our study strongly indicates the safety of the PEPPS when considered alongside techniques performed at other centres.
In an extra step, we tried to investigate the safety of the single components of PEPPS. Metastasis and recurrence rates did not differ considerably in patients with or without preoperative bronchoscopic treatment, highlighting the safety of the bronchoscopy part of PEPPS. Despite the absence of a similar study, there were studies that support the safety of an interventional bronchoscopy in carcinoids in general.21 ,24 ,28 Furthermore, metastasis and recurrence rates did not increase in cases with incomplete bronchoscopic tumour ablation.
As mentioned, the safety of parenchyma-sparing surgery methods has already been shown.6 ,17 ,29 Metastasis and recurrence rates in our two surgery classes support this hypothesis. Moreover, after parenchyma-sparing techniques, we observed less metastasis and tumour recurrence, although this difference was not significant.
Current classification of bronchopulmonary carcinoid tumours lacks information on the different aggressiveness of centrally versus peripherally located tumours in the surgically resected specimens on which the classification is based. Therefore, it has to be further investigated if centrally located tumours that are accessible for bronchoscopic treatment behave in a less aggressive manner than often proclaimed.
Conclusion
In conclusion, a preoperative bronchoscopic intervention seems to be a reasonable preparation for a subsequent surgical procedure in patients with centrally located TCs and ACs of the lung. The results of this study with a long-term surveillance of 227 months support our hypothesis that a parenchyma-sparing method was feasible more frequently after bronchoscopic tumour ablation. Moreover, PEPPS seems to have no negative effects on survival and oncological outcome measured by metastasis and recurrence rates. Therefore, we recommend applying PEPPS in these patients whenever technically feasible and clinically reasonable, and other treatment options like solely bronchoscopic ablation are not suitable to patients due to the so-called iceberg phenomenon, as parenchyma-sparing techniques are linked with less morbidity and a higher quality of life in the long term. Further studies are necessary to investigate the role of retention pneumonia in this procedure, and to identify patients who might benefit from a solely curative bronchoscopic treatment.
Acknowledgments
The authors acknowledge comments and corrections provided by Walter J Urba, MD, PhD, medical oncologist and director of cancer research at Providence Medical Group, Portland, Oregon, USA.
References
Footnotes
Contributors MN contributed substantially to study concept and design, data acquisition, analysis, and interpretation, drafting the manuscript, writing and approval of the final manuscript. AH contributed to statistical analysis and interpretation of the data. MS and WG contributed to data acquisition. FR contributed to study design and data interpretation. AM-H contributed to data acquisition and data interpretation. RAH contributed to study concept and data interpretation. ML contributed to study concept and design, data interpretation and approval of the final manuscript.
Competing interests None declared.
Ethics approval Local ethics committee of the university (LMU) of Munich, Germany.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.