Article Text

Abstract
Introduction Pulmonary aspergillosis has variable course of illness, severity and outcomes depending on underlying conditions. There is limited data available on the clinical manifestations and outcome of pulmonary aspergillosis from Pakistan.
Methods To determine the clinical manifestations and outcome of pulmonary aspergillosis in a tertiary care hospital a retrospective study was conducted from 2004 to 2014 in patients admitted with pulmonary aspergillosis at the Aga Khan University Hospital Karachi, Pakistan.
Results Of the 280 cases with provisional diagnosis of aspergillosis 69 met the inclusion criteria. The mean age was 45±15.7 years, 48 (69.6%) were men and 21 (30.4%) had diabetes mellitus (DM). The average length of hospital stay (LOS) was 10.61±9.08 days. Aspergillus fumigatus was the most common (42.0%), followed by Aspergillus flavus (28.9%). More than one-third of patients previously had tuberculosis (TB) (39.13%). The commonest pulmonary manifestation was chronic pulmonary aspergillosis (CPA) 47 (68.1%) followed by invasive pulmonary aspergillosis (IPA) 12 (17.4%) and subacute invasive aspergillosis (SAIA) 8 (11.6%). Surgical excision was performed in 28 patients (40.57%). Intensive care unit admission was required for 18 patients (26.08%). Case fatality rate was 14/69 (20.3%). DM, mean LOS and hypoxic respiratory failure were identified as independent risk factors of mortality on multivariate analysis.
Conclusion A. fumigatus was the most frequent species found especially in patients with prior TB. CPA was the commonest pulmonary manifestation seen as post TB sequel. Diabetes, hypoxic respiratory failure and increased LOS were independent predictors of poor outcomes. Overall patients had good outcome with CPA compared with SAIA and IPA.
- Aspergillus Lung Disease
- Respiratory Infection
- Tuberculosis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Pulmonary aspergillosis has variable clinical presentations and outcomes.
Very limited data is available from Pakistan on its different clinical presentations.
Chronic pulmonary aspergillosis (CPA) is the commonest pulmonary manifestation as post-TB sequel.
Overall patients had good outcome with CPA compared with subacute invasive pulmonary aspergillosis (SAIA) and invasive pulmonary aspergillosis (IPA).
Introduction
Aspergillosis is a spectrum of diseases cause by the Aspergillus spp. that are ubiquitous saprophytic fungi. The clinical spectrum of aspergillosis varies from the colonisation of the organism to the presence of fungus ball (aspergilloma) or an allergic response known as allergic bronchopulmonary aspergillosis (ABPA) to subacute invasive aspergillosis (SAIA) or as chronic necrotising pneumonia and invasive pulmonary aspergillosis (IPA).1 Aspergillus fumigatus has been reported to be responsible for more than 90% cases of invasive aspergillosis.2 Aspergillus flavus, Aspergillus terreus, and Aspergillus niger are responsible for the remaining invasive cases. The incidence of IPA globally is increasing due to increase in immunosuppressed patients but its true incidence is unclear in Pakistan. Aspergilloma is usually found in patients with previously formed lung cavities, whereas ABPA is a hypersensitivity reaction to Aspergillus antigens, and is usually seen in patients with atopy, asthma or cystic fibrosis.3 Pulmonary aspergillosis has a variable course of illness, severity and outcomes.
According to the WHO report in 2011, around 1.2 million people in the world have been estimated to have chronic pulmonary aspergillosis (CPA) as a sequel to tuberculosis (TB) and most cases occur in South-East Asia, Western Pacific and African regions.4 Scarce data is available on CPA as a post-TB sequel and in structural lung diseases from developing countries.
The aim of this study is to determine the clinical manifestations and outcomes of pulmonary aspergillosis in a tertiary care hospital in Karachi, Pakistan to help understand the nature of disease and to improve the clinical outcome in this part of the world.
Methods
This is a retrospective study in patients admitted with pulmonary aspergillosis at the Aga Khan University Hospital (AKUH), Karachi, Pakistan from January 2004 to December 2014. The research protocol of this study was approved by the Ethical Review Committee of the Aga Khan University. All patients admitted with a diagnosis of aspergillosis using International Classification of Disease, Ninth Revision codes (ICD-9 1173) were identified. Information was collected from Health Information Management Services (HIMS), Department of AKUH. Data on demographics, comorbid, underlying lung condition, radiographic and microbiological findings, mean length of hospital stay (LOS), requirement of invasive and non-invasive mechanical ventilation (NIMV), respiratory complications and in hospital mortality was collected on a predesigned form.
Inclusion criteria were (1) patient 18 years and above. (2) Positive sputum and/or positive bronchoalveolar lavage (BAL) (smear and/or culture) for Aspergillus and/or positive lung histopathology suggestive of aspergillosis. (3) Chest X-ray/CT scan of the chest infiltrates suggestive of aspergillosis. We excluded all patients with culture positive for Aspergillus other than respiratory specimen, and whose medical records are with incomplete information. Culture positive cases suggestive of colonisation only were also excluded. Outcomes were in-hospital mortality, mean LOS and respiratory complications.
Patients were classified further into CPA, SAIA, IPA and ABPA. CPA was defined as one or more cavities with or without a fungal ball or nodules on thoracic imaging, direct evidence of Aspergillus infection (microscopy or culture from biopsy) or an immunological response to Aspergillus spp. and exclusion of alternative diagnoses, all present for at least 3 months.5 CPA was further classified into two categories (1) single cavity with single fungal ball with no radiological progression over at least 3 months of observation is labelled as single (simple) pulmonary aspergilloma and (2) patients with one or more pulmonary cavities containing one or more aspergilloma with serological or microbiological evidence of Aspergillus spp. and significant pulmonary and/or systemic symptoms and evidence of radiographic progression (new cavities and increasing infiltrates) over at least 3 months of observation were labelled as chronic cavitary pulmonary aspergillosis (CCPA).
SAIA defined as invasive aspergillosis with mildly immunocompromised host occurred over 1–3 months with variable radiographic features and biopsy showed hyphae in invading lung tissue.5 Patients with histology and/or culture of a specimen of tissue taken from a site of disease showed evidence of Aspergillus was labelled as proven IPA. While the probable and possible invasive infections were determined by a host factor, clinical signs and symptoms, and mycological evidence that encompassed culture and microscopic analysis.6 Patients were labelled ABPA depending on the criteria as reported previously by Rosenberg et al.7
Laboratory methods
Fungal cultures were performed at the Aga Khan University Clinical Laboratory, which is one of the largest laboratories in Pakistan. This laboratory is a regional supranational laboratory for TB and regularly participates in College of American Pathologists (CAP) surveys for Mycology smear and culture. During the study period fungal smear was made using 10% potassium hydroxide (KOH). Sputum and tracheal aspirates for fungal culture were processed semiquantitatively by picking up the most purulent portion and BAL were centrifuged at 1200×g for 10 min and the sediment was used for microscopy and culture inoculation. The specimen was inoculated on two plates of Sabouraud Dextrose Agar (incubated at 28°C and 37°C), one plate of Sheep Blood Agar (incubated at 37°C), one plate of Potato Dextrose Agar (incubated at 28°C) and one plate of Mycosel Agar containing cycloheximide (incubated at 28°C). All plates were reviewed by trained laboratory technologist and consultant microbiologist daily for first week and then twice weekly for 3 weeks.
Culture plates were incubated and examined until 4 weeks before reporting them as negative. Any fungal growth was assessed by clinical microbiologist for clinical significance and to rule out contamination and only significant isolates were further processed and identified. Identification of Aspergillus spp. was made on the basis of gross appearance and microscopic morphology of the colonies.8
Statistical analysis
All analyses were conducted by using the SPSS (Release 19.0, standard version, copyright © SPSS; 1989–2002). A descriptive analysis was performed for demographic features presented as mean±SD for quantitative variable that is, age and lengths of hospital stay. Number (percentage) for qualitative variables that is, gender, mortality, smokers, associated underlying disease, presenting symptoms, radiographic findings, isolated Aspergillus spp., and respiratory complications associated with Aspergillus. Comparisons were made between the alive and dead patients and χ2 test of independence was carried out. Multivariate logistic regression analysis was performed on variables reaching significance on univariate analysis to determine factors predicting the poor outcome. All p value ≤0.05 was taken as significant.
Results
A total of 280 cases were reviewed with aspergillosis from January 2004 to December 2014 and 69 met the inclusion criteria. These cases were further classified as: CPA 47 cases (68.1%) including aspergilloma 26 cases (55.3%) and CCPA 21 cases (44.7%). IPA was found in 12 cases (17.4%), which included 2 (16.7%) proven and 10 (83.37%) probable cases. ABPA was found in two cases (2.9%) and SAIA was found in eight cases (11.6%) of which six patients (75%) had diabetes and two patients (25%) had active TB with underlying chronic obstructive pulmonary disease (COPD) (figure 1).

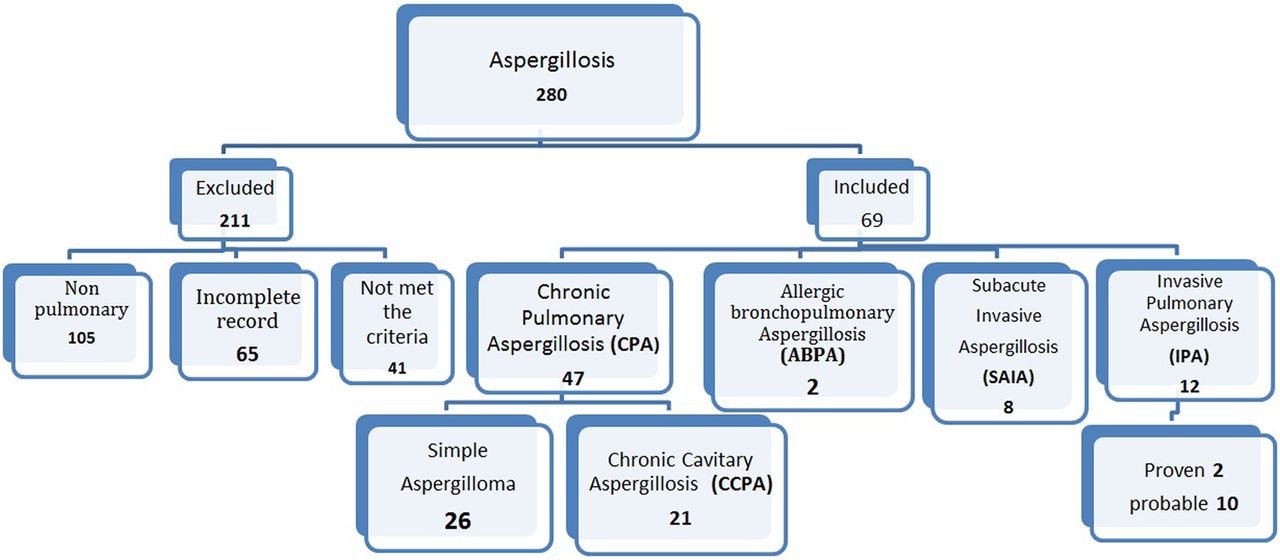{kind=link}
Showing enrolment of patients with pulmonary aspergillosis.
The mean age was 45±15.7 years, 48 patients (69.6%) were men and 43 (62.3%) were non-smokers. The most common associated systemic illness was diabetes mellitus (DM) n=21 (30.4%) followed by chronic renal failure n=16 (23.2%) and haematological malignancies n=10 (14.5%). It was noted that 21.8% patients were on systemic corticosteroids, 8.7% were neutropaenic and 7.24% were on chemotherapy. The commonest associated underlying lung disease was TB n=36 (52.2%), of which 39.1% had history of TB and 13.04% had active TB (table 1).
Characteristics of patients with pulmonary aspergillosis
Symptoms were usually non-specific, commonest symptoms being cough (n=44, 63.76%), followed by fever (n=40, 57.9%), haemoptysis (n=40, 57.9%) and weight loss (n=20, 28.9%).
On chest imaging, 29 patients (42.0%) had nodular infiltrates, 25 (36.23%) had fungal ball, 24 (34.8%) had cavitary lesions, 19 (27.58%) had consolidation, 14 (20.3%) had fibrosis/pleural thickening and 10 (14.5%) had bronchiectasis.
Sputum/BAL culture was positive for Aspergillus spp. in 46 (66.7%) patients, 31 (44.9%) had positive histopathology, 38 (55.1%) had positive culture only, 23 (33.3%) had only histopathology while both were positive in 8 (11.6%) patients. The most commonly isolated species was A. fumigatus n=29 (42.0%) followed by A. flavus n=20 (28.9%), A. niger n=7 (10.1%) and A. terreus n=5 (7.2%), 33 (47.8%) patients had single Aspergillus spp., while 13 (18.8%) patients had two or more Aspergillus spp. in culture, while in 23 (33.3%) only fungal smear was positive.
Respiratory complications developed in 28 (40.6%) patients. Hypoxic respiratory failure was the commonest complication in these patients followed by pneumothorax (table 2).
Clinical outcomes in patients with pulmonary aspergillosis
The mean LOS was 10.61±9.08 days. Intensive care unit (ICU) admission was required in 18 patients (26.1%) and mechanical ventilation in 17 (24.61%). NIMV used in eight (11.6%) patients.
Mortality was seen in 14 patients (20.3%) and was higher in ICU patients (n=13/18, 72.2%) and in IPA 7/12 (58.3%), SAIA 4/8 (50%) compared with CPA 3/47 (6.4%).
Factors associated with mortality
On univariate analysis (table 3), DM was a significant comorbidity (p value 0.05), followed by haematological malignancy (p value 0.01) and renal failure (p value 0.002). The non-survivors had a longer ICU stay (p value 0.001), more respiratory complications (p value 0.002) and greater mean LOS (p value 0.009) compared with survivors. Patients with consolidation had higher mortality (p value 0.001). Patients with fungal ball who underwent surgical excision had good outcomes (p value 0.001).
Risk factors associated with mortality in patients with pulmonary aspergillosis
DM, mean LOS and hypoxic respiratory failure were identified as independent risk factors of mortality on multivariate analysis (table 3).
Discussion
This is the first study describing clinical features and outcome of pulmonary aspergillosis from a tertiary care hospital from Pakistan. The prevalence of fungal infection has dramatically increased over recent years due to underlying risk factors.9 Culture remains a gold standard for the diagnosis of aspergillosis but has low sensitivity. Culture positivity does not always reflect infection as these organisms could also occur as colonisers or contaminants. We have reported a higher culture positivity rate (66.7%) of sputum/BAL compared with 23.3% from an Indian study.10 This high positivity rate could also reflect colonisation or contamination; however in these cases growth of Aspergillus spp. was reported only after assessing significance. In addition, the laboratory strictly monitors culture contamination rate as a quality indicator, also all specimens were processed in safety cabinet to avoid contamination within laboratory during processing. Furthermore clinical evaluation of these cases also confirmed the significance of the growth. Recent advances of diagnosis of invasive aspergillosis include antigen detection tests; galactomannan and β-D-glucan (component of cellular wall). Both these tests are approved by the US Food and Drug Administration (FDA) for the diagnosis of IPA. They help in the early diagnosis and confirmation of IPA and are also helpful in the assessment of the evolution of infection during treatment with serial levels.11 Unfortunately, the antigen detection tests were not available at our centre during the study period and the rates of aspergillosis reported could be an underestimate.
Majority of patients in this study were men and the commonest isolated species was A. fumigatus similar to the previous literature2 ,10 followed by A. flavus, A. niger and A. terreus. We found CPA as the most common pulmonary manifestation. In the literature the commonest form of CPA is CCPA.5 However, the incidence of aspergilloma was more common than CCPA in our study; this may be because ours is a tertiary care hospital and patients are referred for interventions. Patients with pulmonary insults like COPD, chronic fibrocystic healed TB, interstitial lung disease (ILD), pneumoconiosis and cystic fibrosis are well-known risk factors for CPA.12 In our study majority of patients had a history of TB as reported previously.4 ,10 ,13 ,14 One of the reason being that TB is endemic in Pakistan and majority of these patients developed CPA as a post-TB sequel. It is interesting to note that some of the patients also had active TB along with Aspergillus infection; the association of active TB with Aspergillus infection is rarely seen and reported only in few case reports.15 ,16
The commonest underlying systemic condition among our patients was DM; increased incidence of TB among patients with diabetes is well known due to impaired immunity and associated with aggressive course and outcomes.17 ,18 Previous literature has reported that patients with DM with TB had more severe clinical manifestation (cavitation), severe treatment and post treatment outcomes like failure and death, death and relapse.19 ,20 The majority of patients with SAIA also had underlying diabetes. So diabetes was identified as an important risk factor for pulmonary aspergillosis for SAIA and CPA.
DM has been rarely associated with IPA and reported only in few case reports.21 ,22 In our study the majority of cases had probable IPA but the revised definition of IPA has some limitations as it only included immunocompromised patients.6 A study in 172 critically ill patients showed that 83 had invasive disease while 60% had no risk factors for IPA.23 Critically ill patients are prone to develop disturbances in immunoregulation, which makes them vulnerable for fungal infections. Thus besides neutropaenia, haematopoietic stem cell transplant, DM, renal failure, COPD, liver failure are important risk factors in ICU.
Patients with aspergillosis usually presents with non-specific constitutional symptoms such as fever, cough, haemoptysis and weight loss or rarely may be asymptomatic in CPA.24 In this study patients mostly had non-specific symptoms. Radiographic presentation is also variable from rounded densities, pleural-based infiltrates to cavitation while pleural effusion is rarely seen. Greene25 found 94% of patients with IPA had at least one nodular lesion. In a study IPA in patients with neutropaenia who underwent stem cell transplantation had nodules 67%, ground glass 56% and consolidation 44%,26 while halo sign and air crescent sign were usually non-specific.27 In CPA, patients had pleural thickening and cavitation while fungal ball (mycetoma) can be seen in 50%.28 In our study majority of the patients had nodular infiltrates 42.2%, followed by fungal ball (mycetoma), cavitation and consolidation.
Overall mortality was 72.2% and was higher in IPA and SAIA compared with CPA. Mortality in CPA ranges from 10% to 30%, low in simple aspergilloma compared with CCPA.4 However, severity of the underlying pulmonary disease and the extent of lung destruction are important predictors of mortality and outcomes among patients with CPA. Limited data is available for SAIA while in IPA reported morality ranged from 50% to 80%.29 ,30 Majority of these patients developed hypoxic respiratory failure and had bilateral consolidations. Hypoxic respiratory failure is well known in patients with neutropaenia during the recovery phase with IPA, likely secondary to neutrophil influx.31 ,32 Interestingly, in our study only 8.69% patients were neutropaenic. This is most likely due to low feasibility of performing invasive procedures to collect appropriate samples for culture and the absence of antigen detection tests during the study period at our institute. Besides respiratory failure 14.5% developed pneumothorax. Empyema was a rare complication33 seen in 2.89% patients in this study.
The mean LOS is variable in patients with pulmonary aspergillosis and available data is also limited. As in our study population majority of the patients had CPA, therefore it is difficult to compare the results with the available data which is particularly on IPA.
Our study has added important information on pulmonary aspergillosis particularly from Pakistan but there are certain limitations of this study. (1) It is a retrospective study and we cannot standardise the diagnostic and treatment approaches in these patients. (2) It is a single centre study and study results cannot be generalised. (3) Galactomannan and β-D-glucan assays were not available during this study period and could not be used to diagnose patients in whom invasive sampling could not be performed. We recommend large multicentre prospective studies using β-D-glucan and galactomannan as an adjunctive diagnostic aid as both are now incorporated in the revised European Organisation for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) criteria for diagnosing IPA6 and recommended for CPA in BAL by European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society (ESCMID/ERS).5
Conclusion
A. fumigatus was the most frequently isolated species in our region, found especially in patients with history of TB. CPA was the commonest pulmonary manifestation as post-TB sequel. Patients with diabetes, hypoxic respiratory failure and increased LOS were independent predictors of poor outcomes. Overall patients had good outcome with CPA compared with SAIA and IPA.
References
Footnotes
Contributors NI and MI have made contributions to conception and design, interpretation of data, drafting of the manuscript and revising it critically for important intellectual content. ABSZ has made contributions to interpretation of data, and drafting of the manuscript. KJ and JAK have made contributions in drafting of the manuscript and revising it critically for important intellectual content. SA has made contributions to acquisition and interpretation of data; and in drafting of the manuscript. All authors have read and approved the final manuscript.
Competing interests None declared.
Ethics approval Ethical approval was taken from Ethical Review Committee of Aga Khan University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data set supporting the conclusions of this article is included within the article.