Article Text

Abstract
Introduction The coexistence of chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVD) is frequent and might be inter-related through inflammation-related processes reflected by specific markers. Here, we studied angiopoietin-like protein 4 (ANGPTL4), an upcoming cardiovascular marker, in stable COPD, and its relationship to cardiovascular function with respect to well-known CVD risk factors.
Methods In a prospective COPD cohort study, we investigated serum ANGPTL4 levels, vascular status (ankle–brachial index (ABI)) and cardiac function (N-terminal pro-B-type natriuretic peptide (NT-proBNP)) as well as airflow limitation, objectively measured physical activity, the metabolic syndrome, high-sensitive C reactive protein (hs-CRP) and other CVD risk factors at 2 time points. We initially studied 74 stable COPD patients and 18 controls. For internal validation, we additionally studied 160 COPD patients of a former visit.
Results ANGPTL4 was significantly elevated in COPD patients compared with controls (p=0.026). After correction for traditional CVD risk factors, including hs-CRP, higher levels of ANGPTL4 were independently associated with lower ABI (p=0.023) and higher NT-proBNP (p<0.001). These findings were confirmed in the internal validation analysis, which included echocardiographic assessments.
Conclusions Serum ANGPTL4 is independently associated with cardiovascular function in COPD and might qualify as a biomarker reflecting a pathogenic link between COPD and CVD.
- COPD ÀÜ Mechanisms
- Systemic disease and lungs
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Angiopoietin-like 4 is elevated in stable COPD and is an independent predictor of atherosclerosis and cardiac function in COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a highly prevalent and complex disease characterised by airflow limitation, a varying degree of systemic inflammation and frequent comorbidities.1 The coexistence of cardiovascular disease (CVD) is a leading cause of morbidity and mortality in COPD, specifically in mild-to-moderate patients.2–4 However, the mechanisms that explain the relationship between COPD and CVD remain elusive.5
Systemic inflammation is a hallmark of CVD6 and likely represents a key link between COPD and CVD independently of common risk factors, such as cigarette smoking.7–10 Dyslipidaemia is another risk factor for CVD and represents an important criterion for the diagnosis of the metabolic syndrome,11 which is also prevalent among COPD patients.12 Angiopoietin-like protein 4 (ANGPTL4) is an acute phase protein involved in inflammatory processes and an inhibitor of the enzyme lipoprotein lipase that hydrolyses triglycerides and phospholipids.13 ,14 Therefore, ANGPTL4 is strongly associated with atherosclerosis.13–17 Recently, three large studies highlighted the association between inactivating mutations in ANGPTL4 and decreased risk of coronary artery disease (CAD).15–17 On the other hand, one preliminary study suggested that circulating ANGPTL4 levels are elevated in COPD patients when compared with healthy controls.18 So far, however, the role of ANGPTL4 for cardiovascular function in COPD is unclear.
We, therefore, aimed to analyse levels of serum ANGPTL4 in stable COPD patients and controls without any lung disease, and to investigate the relationship of ANGPTL4 levels with vascular status (determined by the ankle–brachial index (ABI)) and cardiac function (determined by N-terminal pro-B-type natriuretic peptide (NT-proBNP)) in a COPD cohort. We further wanted to confirm this latter aim by the use of an internal validation cohort, which also included echocardiographic assessments.
Methods
Study population
This study is nested within a prospective COPD cohort study performed at the Pulmonary Research Institute at the LungClinic Grosshansdorf (Germany). Here, we included 160 stable outpatients with mild to very severe COPD, who were studied at the baseline visit (T0) and after 3 years of follow-up (T1), and 18 non-smoking controls, who were only enrolled at T1. Details of the COPD population and methodology have been published elsewhere.12 ,19–21 Briefly, the COPD patients had to have an exacerbation-free interval longer than 2 months previous to the study entry and no clinical signs of heart failure. The controls were never-smokers or ex-smokers with <5 packyears in the past, without any lung disease. We initially analysed serum levels of ANGPTL4 in 74 COPD patients and 18 controls at T1. The validation analysis was based on 160 COPD patients of T0, including 86 independent COPD patients. The study was approved by the Ethics Committee of the Medical Association of Schleswig-Holstein, Bad Segeberg, Germany (III/EK 116/05(I); 185/08(I)), and all participants gave written informed consent.
Measurement of serum ANGPTL4 levels and cardiovascular function
We analysed serum samples for ANGPTL4 protein levels using DuoSet ELISA kit (R&D systems). The detection limit for ANGPTL4 was 1.25 ng/mL. Interassay precision was <10%. We determined global cardiac function by serum levels of NT-proBNP via an Elecsys proBNP Immunoassay (Roche, Mannheim, Germany) according to the manufacturer's instructions. Higher levels of NT-proBNP are an established indicator for heart failure or increased cardiac load in general.22 For patients not presenting in an acute setting, values below 125 pg/mL virtually exclude significant cardiac dysfunction.22
To assess the vascular status, we measured the ABI by Doppler sonography using a handheld 8 MHz probe (SonoMate 100, DEGO, Nagold, Germany) as previously described.20 ,23 The ABI is the ratio of the systolic blood pressure at the ankle divided by the systolic pressure at the arms. For this report, we calculated the ABI of each leg by dividing the higher pressure of the posterior tibial or the dorsalis pedis artery by the higher pressure of the right or left brachial artery and we used the lower ABI of both legs as a CVD marker according to the current statement of the American Heart Association.24 Normal ABI values range from 1.11 to 1.40 and a low ABI (most commonly used threshold ≤0.90) is an established indicator of peripheral artery disease. In addition, the ABI is an indicator for systemic atherosclerosis and can serve as a prognostic marker for cardiovascular events.24 For a study population without abnormally high ABI values (ie, ABI >1.40), there is a graded inverse association of CVD risk and ABI.24
In addition to NT-proBNP and ABI, the cardiac function was also assessed by transthoracic echocardiography at T0 (Vivid 3, GE Healthcare, Chalfont St Giles, England). We measured systolic left heart function (left ventricular ejection fraction), diastolic left heart function (ratio of the peak velocity of the early E-wave to atrial A-wave (E-wave/A-wave), deceleration time of the early transmitral flow and left atrium area), left ventricular mass and global right ventricular function (Tei index, which is the sum of isovolumetric contraction time and isovolumetric relaxation time divided by the ejection time). Left ventricular mass was calculated using the linear method and is reported indexed to body surface area.25 Detailed methods on the measurement of the other parameters are described elsewhere.19 ,26 Indicators of systolic and diastolic left ventricular function served as additional cardiovascular markers for the validation analyses, as well as the left ventricular mass, which is a strong predictor of cardiovascular events in general.25
Measurement of established cardiovascular risk factors as covariates
We also determined a panel of established CVD risk factors as possible confounders for the association between ANGPTL4 and cardiovascular function. This included the presence of the metabolic syndrome (based on triglyceride levels, HDL cholesterol, waist circumference and blood pressure), LDL cholesterol, hs-CRP, smoking status, history of CAD, physical activity and postbronchodilator spirometry. Physical activity was measured by a multisensory armband (SenseWear Pro 2, Pittsburgh, USA) over a period of 1 week as previously described.19 The presence of metabolic syndrome was assessed according to the criteria of the International Diabetes Federation.11 ,12
Statistical analyses
Univariate differences between the study groups were evaluated using the t-test or Mann-Whitney U test for continuous variables (depending on distribution and homogeneity of variances) or χ2 tests for dichotomous variables. Skewed variables were also log-transformed to obtain a normal distribution for further analyses. Bivariate associations were analysed by the Pearson correlation coefficient.
The second research question was studied by means of multivariate linear regression analyses. For the analyses of ABI and NT-proBNP as the dependent variables, we first assessed the effect of ANGPTL4 alone and next with adjustments for age, sex, smoking status and body mass index (BMI). Next, we employed two models including a broad spectrum of specific established risk factors (ie, for vascular and cardiac risk-adjusted models). These models included age, sex, BMI, smoking status, the metabolic syndrome, LDL cholesterol FEV1 and hs-CRP, respectively, as well as physical activity level for the atherosclerosis model and history of CAD for the cardiac dysfunction model.
Results
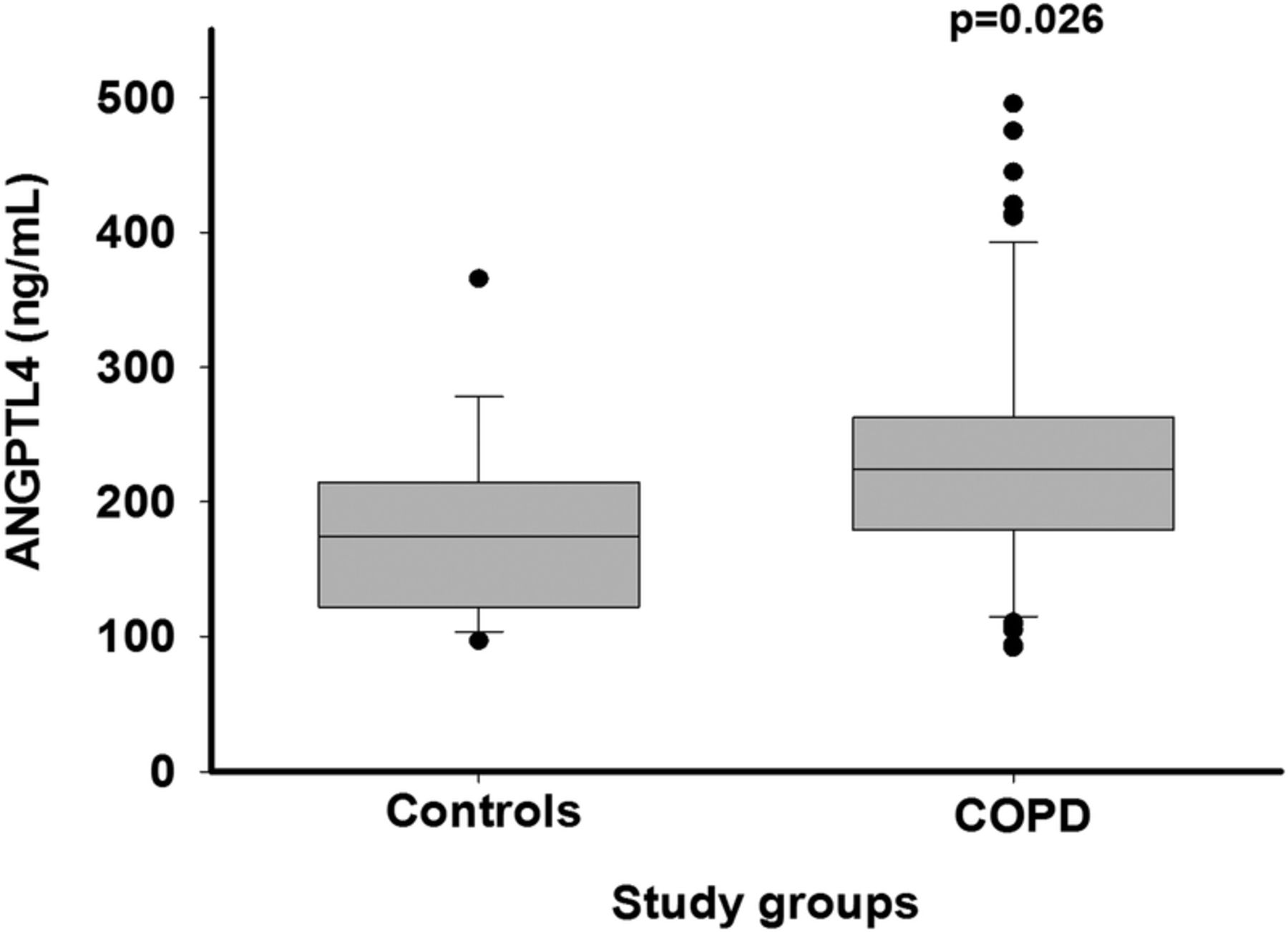
Patient characteristics are described in table 1. COPD patients and controls were well matched for age, gender and BMI. Smoking status, lung function, physical activity, ABI, frequency of CAD and hsCRP levels differed significantly between both groups, while there were no differences in the frequency of hypertension, elevated NT-proBNP levels and the metabolic syndrome, including each separate criterion (table 1). Serum ANGPTL4 was significantly higher in patients with COPD compared with controls (p=0.026; figure 1), even after excluding patients with a history of CAD (p=0.030). Within patients with COPD, there was no significant difference between ex-smokers and active smokers (p=0.84).
Patient characteristics according to chronic obstructive pulmonary disease patients and controls without any lung disease

Serum levels of angiopoietin-like protein 4 (ANGPTL4) according to patients with chronic obstructive pulmonary disease and controls without any lung disease. After adjustment for smoking status and history of coronary artery disease, levels of ANGPTL4 still differed significantly (p=0.039). Lines within the box–whisker plot represent the median and the boxes represent the IQR.
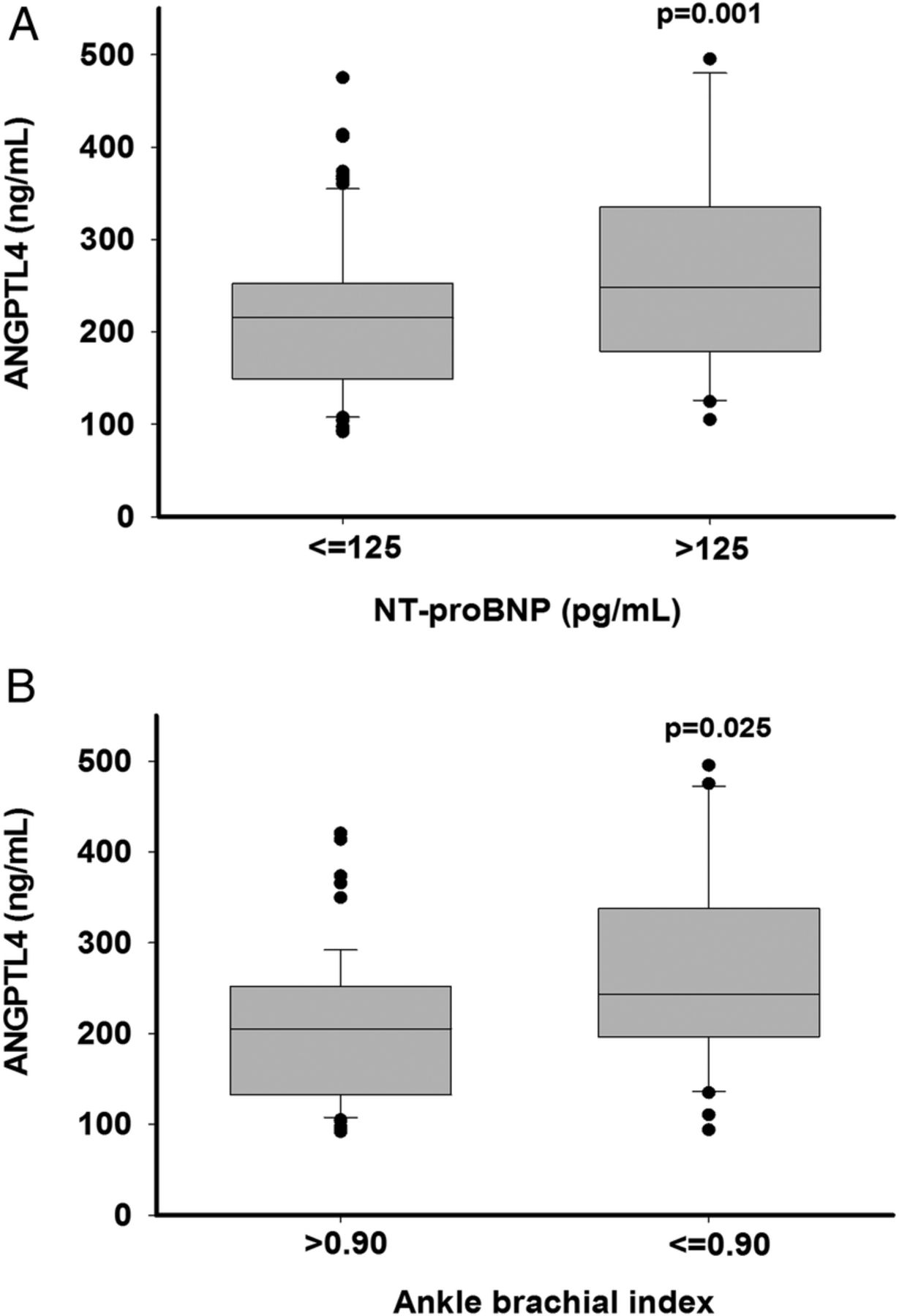
Figure 2A, B stratifies ANGPTL4 values according to established cut-off values of NT-proBNP (p=0.001) and ABI (p=0.025). In patients with COPD, ANGPTL4 also correlated significantly with the linear forms of log NT-proBNP (r=0.57, p<0.001) and ABI (r=−0.31, p=0.008). In multivariate regression analyses adjusting for a broad panel of established CVD risk factors, ANGPTL4 was an independent predictor for the ABI and NT-proBNP levels (table 2). In the final model for ABI, which included adjustments for smoking, the metabolic syndrome plus LDL, FEV1, hs-CRP and physical activity, ANGPTL4 was still an independent predictor (table 2). In the final model for NT-proBNP, which included adjustments for the metabolic syndrome plus LDL, FEV1, hs-CRP and history of CAD, ANGPTL4 also remained as a strong predictor (p<0.001; table 2).
ANGPTL4 as independent predictor for indicators of atherosclerosis and cardiac function in patients with chronic obstructive pulmonary disease

{kind=link}
{kind=link}
Serum levels of angiopoietin-like protein 4 according to (A) cardiac dysfunction (ie, abnormal N-terminal pro-B-type natriuretic peptide level) and (B) atherosclerosis (ie, ankle–brachial index ≤0.90). Lines within the box–whisker plot represent the median and the boxes represent the IQR.
In the internal validation cohort, ANGPTL4 levels also differed significantly according to established cut-off values of NT-proBNP and ABI (p<0.001 and p=0.022, respectively). Using the same multivariate regression models, ANGPTL4 was confirmed as an independent predictor for the ABI and NT-proBNP (p=0.014 and p<0.001, respectively; table 3). In addition, we also observed significant associations of ANGPTL4 with some functional and morphological echocardiographic parameters, with left ventricular mass as best correlate (r=0.30, p<0.001). Using the multivariate regression model for cardiac dysfunction, ANGPTL4 remained an independent predictor for left ventricular mass (p<0.001; table 4).
Validation analyses for ANGPTL4 as independent predictor of atherosclerosis and cardiac function in chronic obstructive pulmonary disease
Validation analyses for ANGPTL4 as independent predictor of left ventricular mass in chronic obstructive pulmonary disease
Discussion
The main findings in our cohort study are that serum ANGPTL4 levels are elevated in patients with stable COPD and, irrespective of established cardiovascular risk factors, ANGPTL4 is associated with indicators of atherosclerosis and cardiac dysfunction.
ANGPTL4 is a multifunctional protein expressed in the liver, heart, muscle and adipose tissue.13 ANGPTL4 is an inhibitor of the lipoprotein lipase, an enzyme hydrolysing triglycerides from the apolipoprotein B-containing lipoproteins, chylomicrons and VLDL.13 ,14 ,27 Therefore, ANGPTL4 suppresses the release of non-esterified fatty acids and their subsequent uptake by adipose tissue, skeletal and cardiac muscle. Increased levels of ANGPTL4 are in general associated with hypertriglyceridaemia28 and atherosclerosis.29 A large cohort study revealed that plasma ANGPTL4 levels significantly predict cardiovascular events in coronary patients.30 Furthermore, inactivating variants in human ANGPTL4 gene were linked to low plasma triglycerides and elevated HDL cholesterol, and were clearly associated with a reduced risk of coronary heart disease.15–17 ,31 In our study, we show that levels of ANGPTL4 are elevated in stable COPD patients compared with controls without any lung disease. In addition, we found that higher serum levels of ANGPTL4 are independently associated with two indicators of cardiovascular dysfunction in COPD, namely the ABI and levels of NT-proBNP. The ABI is not only an established marker for peripheral artery disease, but also an indicator of generalised atherosclerosis. Therefore, a reduced ABI improves the risk prediction for cardiovascular events beyond traditional risk factors23 ,32 and is associated with higher mortality rates in COPD.20 We found a significant association between higher levels of ANGPTL4 and lower levels of ABI, independent from a broad number of established cardiovascular risk factors, including hs-CRP. NT-proBNP is released in response to increased atrial pressure and it is an established marker of non-specific cardiac dysfunction. NT-proBNP is commonly used as a diagnostic tool for the diagnosis of heart failure,22 which in turn is frequent in COPD. Our data show a strong positive association between levels of ANGPTL4 and NT-proBNP, independent from established cardiovascular risk factors. Overall, our findings are in line with the current theory that inflammatory markers may describe a link between COPD and comorbidities, such as CVD.
This study has a few limitations. First, the results were obtained from cross-sectional analyses. Therefore, we cannot prove a causal relation or directionality of our results, which also could represent a bystander effect rather than an underlying mechanism. Nevertheless, ours is the first study analysing ANGPTL4 in a well-characterised COPD cohort. Importantly, we were able to reproduce the independent association of ANGPTL4 with markers of CVD (extended by echocardiographic parameters) in a larger subset of our cohort. Clearly, further prospective studies are needed to confirm the relationship and effects of ANGPTL4 in COPD.
Second, we do not meet all of the criteria, which have been proposed for developing novel biomarkers in COPD.33 As this study is not a randomised controlled trial, we cannot prove if our biomarker is modifiable and how changes affect clinical outcomes. However, we have indicated that ANGPTL4 has a plausible role in the pathogenesis of COPD and CVD. We have also shown a clear association with COPD and clinical outcomes. Thus, our study identified a potential biomarker candidate rather than confirmed a biomarker ready for clinical use.
In conclusion, we provide evidence that ANGPTL4 is a meaningful predictor of atherosclerosis and cardiac dysfunction in COPD independently of established risk factors, such as hsCRP. Furthermore, we show that serum levels of ANGPTL4 are elevated in patients with COPD. Altogether, our findings allow us to speculate that ANGPTL4 may describe a link between COPD and CVD. Clearly, further longitudinal studies are warranted.
Acknowledgments
The authors thank Petra Timm for her laboratory assistance and Dr Miriam Schaper and Dr Anna-Lena Sack for their help collecting patients' data. This study was supported by the German Center for Lung Research (DZL).
References
Footnotes
Contributors BW, HW and HM conceived and designed the cohort study, SJ and TW conceived analyses on ANGPTL4. BW, AMK, OH, RL, HW and SJ collected data. BW, TM and SJ contributed to analyses. BW, TM, KFR, HM, TW, HW and SJ interpreted the data. BW wrote the first draft. SJ and HW edited the first draft. All authors reviewed, edited and approved the final draft prior to submission.
Funding German Center for Lungresearch (DZL).
Competing interests None declared.
Ethics approval Ethics Committee of the Medical Association of Schleswig-Holstein, Bad Segeberg, Germany (III/EK 116/05(I); 185/08(I)).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.