Article Text

Abstract
Idiopathic pulmonary fibrosis (IPF) is a rare lung disease characterised by progressive loss of lung function, dyspnoea and cough. IPF has a variable clinical course but a poor prognosis. Nintedanib, a tyrosine kinase inhibitor, is one of two drugs approved for the treatment of IPF. In clinical trials, nintedanib slowed disease progression by reducing the rate of decline in forced vital capacity (FVC) in patients with IPF and mild or moderate lung function impairment. The effect of nintedanib was consistent across patient subgroups defined by baseline characteristics including FVC % predicted, diffusion capacity of the lung for carbon monoxide % predicted and the presence of emphysema. Recently, it has been shown that the rate of decline in FVC and the treatment effect of nintedanib are the same in patients with preserved lung volume (FVC >90% predicted) as in patients with greater impairment in FVC, supporting the value of early treatment of IPF. The adverse events most commonly associated with nintedanib, both in clinical trials and real-world clinical practice, are mild gastrointestinal events, particularly diarrhoea. Side effects are manageable in a majority of patients through symptomatic treatment, dose reductions and treatment interruptions, enabling most patients to stay on treatment in the long term.
- Interstitial Fibrosis
- Rare lung diseases
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Idiopathic pulmonary fibrosis (IPF) is a form of interstitial lung disease, which means that it affects the space around the alveoli inside the lungs. IPF is characterised by progressive loss of lung function, dyspnoea and cough, and substantial impairments in quality of life.1 2 IPF is the most common form of interstitial lung disease but is still a rare disease. A study of healthcare claims data in the USA from 2004 to 2010 suggested an incidence of 19.3 cases per 100 000 person-years in people aged 55–64 years.3 IPF is more common in older people, in men and in former smokers.1
The clinical course of IPF is variable, but its prognosis is poor, with historical data suggesting a median survival time after diagnosis of 2–3 years.1 Acute, clinically significant, respiratory deteriorations characterised by evidence of new, widespread alveolar abnormality are known as acute exacerbations of IPF.4 Such acute deteriorations in respiratory function, which are unpredictable and often of unknown cause, are a major cause of morbidity and mortality in patients with IPF.5
In the USA, Europe and several other countries, two drugs have been approved for the treatment of IPF: nintedanib (OFEV)6 7 and pirfenidone (Esbriet).8 9 Each of these drugs received a conditional recommendation for use in the latest international treatment guidelines for IPF, identifying their use as an appropriate course of action in the majority of patients, depending on individual patients’ values and preferences.10 In this article, we present the data supporting the efficacy and safety of nintedanib as a treatment for IPF and discuss key considerations around its use in clinical practice.
What is nintedanib and how does it work?
Nintedanib is an inhibitor of the receptor tyrosine kinases platelet-derived growth factor receptor, fibroblast growth factor receptor and vascular endothelial growth factor (VEGF) receptor and of non-receptor tyrosine kinases of the Src family.11 12 These tyrosine kinases are involved in signalling pathways that have been implicated in the development and progression of fibrosis.13
In vitro studies and investigation in animal models have shown that nintedanib inhibits pathological processes fundamental to the progression of fibrosis, including the migration of fibroblasts, their transformation into myofibroblasts and the deposition of extracellular matrix.12 14 15 Inhibition of these processes reduces the loss of parenchymal architecture and stiffening of the lungs and so reduces the decline in lung volume characteristic of the progression of IPF.15
How effective is nintedanib and in which types of patients has it been tested?
The clinical trial programme for nintedanib included an international phase II trial known as the TOMORROW trial16 and two international phase III trials known as the INPULSIS trials.17 To take part in the INPULSIS trials, patients had to be ≥40 years of age and to have IPF diagnosed in clinical practice <5 years previously. If a surgical lung biopsy was not available, patients had to have honeycombing and/or a combination of traction bronchiectasis and reticulation in the absence of atypical features of usual interstitial pneumonia (UIP) confirmed by central review of high-resolution computed tomography (RCT) taken within the previous year to be eligible to participate. According to the latest international diagnostic guidelines, a diagnosis of IPF requires the presence of a UIP pattern (subpleural basal predominance, reticular abnormality and honeycombing) on HRCT in patients not subjected to a surgical lung biopsy; in the case of possible UIP (no honeycombing), a surgical lung biopsy is required to make a definitive diagnosis.1 As such, the inclusion criteria in the INPULSIS trials differed from the diagnostic guidelines in that patients who had features of possible UIP plus traction bronchiectasis were eligible to participate without a surgical lung biopsy. Patients also needed to have a forced vital capacity (FVC) ≥50% of the predicted value, indicating mild or moderate impairment of lung function, and a diffusion capacity of the lung for carbon monoxide (DLCO) of 30%–79% of the predicted value.17 About two-thirds of patients in the INPULSIS trials were male, mean age was 67 years, mean FVC was 79% predicted, and mean DLCO was 47% predicted (table 1).
Key baseline characteristics of patients in the INPULSIS trials (reproduced with permission from ref. 18
Across the two INPULSIS trials, a total of 1061 patients were randomised and treated with nintedanib 150 mg twice daily or placebo. Dose interruption or reduction to 100 mg twice daily was allowed for the management of adverse events. Patients who prematurely discontinued study medication were asked to continue to attend study visits and undergo assessments as originally planned.
The primary endpoint in the INPULSIS trials was the annual rate of decline in FVC. Change in FVC is a relevant outcome to assess in patients with IPF because a decline in FVC reflects disease progression and is a predictor of mortality.19 20 In both INPULSIS trials, nintedanib reduced the annual rate of decline in FVC versus placebo by about 50%. Pooled data from both trials indicated that nintedanib reduced the decline in FVC by −112.4 mL/year compared with −223.3 mL/year for placebo, a difference of 109.9 mL/year (95% CI 75.9 to 144.0).17 The effect of nintedanib on slowing FVC decline was consistent across patient subgroups defined by baseline characteristics including sex, race (Asian vs white), age (<65 and ≥65 years), smoking history (current/former vs never smoker), the presence/absence of emphysema on HRCT and disease severity indicated by thresholds of FVC (≤70% vs >70% predicted; ≤90% vs >90% predicted), DLCO (>40% vs ≤40% predicted) or Gender-Age-Physiology stage (I vs II/III) (figure 1).21–26 Notably, patients who began the INPULSIS trials with well-preserved lung volume (FVC >90% predicted) (n=274) experienced the same rate of decline in FVC when treated with placebo, and received the same benefit from nintedanib, as patients with less well-preserved lung volume at baseline (n=787), suggesting that patients with ‘mild’ IPF are at risk of disease progression and arguing against a ‘watch and wait’ approach to the management of such patients.25

FVC decline across subgroups of patients in the INPULSIS trials by baseline characteristics (reproduced with permission from ref. 21).
The effect of nintedanib on slowing FVC decline was consistent in subgroups of patients with versus without honeycombing on HRCT at baseline27 and in patients with honeycombing on HRCT and/or confirmation of UIP on surgical lung biopsy (ie, with definite UIP according to current guidelines1) versus patients who had features of possible UIP and traction bronchiectasis on HRCT and no biopsy.28 This is important because honeycombing on HRCT is not a universal feature in patients with IPF29 and the risks of obtaining a surgical lung biopsy in patients with severe physiological impairment or comorbidity may outweigh the benefits of determining whether there is histopathological evidence of honeycombing.30 31
The most precise estimates of the treatment effects of nintedanib come from pooled analyses of data from the TOMORROW and INPULSIS trials, which had similar inclusion/exclusion criteria and trial designs and involved a total of 1231 patients.32 Pooled data from these three trials suggest that compared with placebo, nintedanib reduced the annual rate of decline in FVC by 110.9 mL/year (95% CI 78.5 to 143.3).32 Acute exacerbations were defined in these trials as clinically significant acute deteriorations of unknown cause that were accompanied by worsening dyspnoea and new features on HRCT.16 17 In pooled data from these three trials, nintedanib reduced the risk of an investigator-reported acute exacerbation versus placebo by 47% (HR 0.53; 95% CI 0.34 to 0.83; p=0.0047).32 Furthermore, nintedanib reduced the risks of all-cause mortality and respiratory-related mortality by 30% (HR 0.70; 95% CI 0.46 to 1.08; p=0.0954) and 38% (HR 0.62; 95% CI 0.34 to 1.13; p=0.0779), respectively, versus placebo.32
Are the benefits of nintedanib maintained in the long term?
Patients who completed an INPULSIS trial were eligible to participate in an extension study called INPULSIS-ON, in which all patients received nintedanib open label at a recommended dose of 150 mg twice daily but with treatment interruptions and dose reduction to 100 mg twice daily allowed for the management of adverse events. The latest interim analysis of data from INPULSIS-ON, conducted after patients treated with nintedanib in both INPULSIS and INPULSIS-ON had received nintedanib for a mean of approximately 3 years, suggested that the effect of nintedanib on reducing FVC was maintained over long-term treatment, with no new safety signals identified.33
Patients could enter INPULSIS-ON irrespective of their FVC. Similar absolute changes in FVC from baseline to week 48 of INPULSIS-ON were observed in patients with FVC ≤50% and>50% predicted at baseline. This suggests that nintedanib may have a similar effect on FVC decline in patients with advanced disease as in patients with less advanced disease, but these results should be interpreted with caution given the small number of patients with FVC ≤50% predicted included in the analysis (n=24).34
It is important to note that as IPF is a progressive disease, FVC will continue to decline even in patients treated with antifibrotic drugs. Thus, a decline in FVC in a patient treated with nintedanib does not necessarily indicate a treatment failure. Patients need to be informed that while antifibrotic therapy will slow the progression of their disease, it is not a cure and their lung function will continue to deteriorate.
What are the most common adverse events seen with nintedanib and how should they be managed?
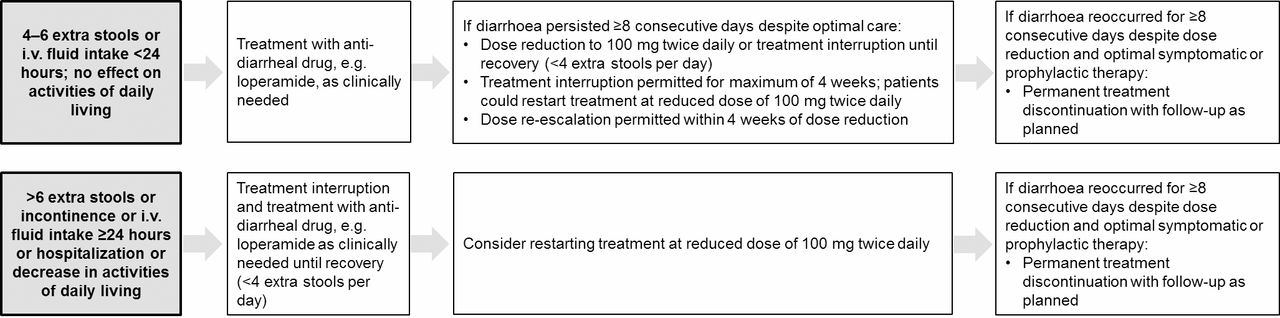
The most common adverse events associated with the use of nintedanib are gastrointestinal events, particularly diarrhoea (table 2).17 18 Diarrhoea should be managed using antidiarrhoeal drugs such as loperamide and through dose reductions and treatment interruptions (figure 2). In the INPULSIS trials, at least one diarrhoea adverse event was reported in 62.4% of patients treated with nintedanib compared with 18.4% of patients treated with placebo, but only 55% of patients treated with nintedanib who experienced diarrhoea were given antidiarrhoeal drugs.17 18 Most diarrhoea adverse events were mild in intensity and resolved without the need for dose reduction or treatment interruption; fewer than 1 in 20 patients permanently discontinued nintedanib due to diarrhoea.17 18

{kind=link}
{kind=link}
Algorithm for management of diarrhoea in the INPULSIS trials (reproduced with permission from ref. 18).
Most frequent adverse events reported in the INPULSIS trials (reproduced with permission from ref. 18)
In the INPULSIS trials, clinical laboratory testing was undertaken at screening and weeks 2, 4, 6, 12, 18, 24, 30, 36, 44 and 52. Alanine aminotransferase (ALT) and/or aspartate aminotransferase (AST) levels ≥3 × upper limit of normal (ULN) and bilirubin levels ≥1.5 × ULN were more common in patients treated with nintedanib than placebo (ALT and/or AST 5.0% vs 0.7%; bilirubin 2.4% vs 0.7%).18 Liver enzyme elevations should be managed through dose reduction and temporary or permanent treatment discontinuation.18 In the INPULSIS trials, liver enzymes had returned to the normal range by the end of treatment in the majority of patients, with no cases of Hy’s law observed in patients treated with nintedanib. In a retrospective study of 32 patients with IPF conducted at a single Japanese centre, elevations in AST/ALT >3 × ULN were reported in 34% of patients.35 The reasons behind this higher incidence remain unclear but may relate to smaller body size and to more frequent blood sampling.
Data collected in the real world through compassionate use programmes and postmarketing surveillance suggest that nintedanib has a similar safety and tolerability profile in clinical practice as has been observed in clinical trials.36–39 In 62 patients with a mean FVC of 64% predicted and a mean DLCO of 40% predicted who were treated with nintedanib for a mean of 8 months in a German compassionate use programme, diarrhoea was reported in 63% of patients and adverse events led to permanent discontinuation of nintedanib in 3% of patients.36 Elevations in AST/ALT >3 × ULN were reported in 8% of patients and resolved with dose reduction and/or treatment interruption.36 Postmarketing surveillance data from 6758 patients treated with nintedanib for a mean of 113 days in the US found that diarrhoea, nausea and hepatic disorders were reported in 42%, 22% and 3% of patients, respectively.38
What cautions need to be borne in mind when considering using nintedanib?
Due to its inhibition of the VEGF receptor, nintedanib might be associated with an increased risk of bleeding.40 Nintedanib should be used in patients with known risk of bleeding only if the anticipated benefit outweighs the potential risk.6 7 An alternative antifibrotic therapy (pirfenidone) has been approved for the treatment of IPF. Patients receiving full-dose anticoagulation or at known risk of bleeding were excluded from clinical trials of nintedanib.16 17 In the INPULSIS trials, bleeding adverse events were reported in 10.3% and 7.8% of patients treated with nintedanib and placebo, respectively, with serious bleeding events reported in 1.3% and 1.4%, respectively.18 The most common bleeding events reported in patients treated with nintedanib were epistaxis and contusion. Incidence rates (95% CI) per 100 patient-years of bleeding events in the nintedanib and placebo groups in INPULSIS were 11.82 (9.29, 15.05) and 8.34 (5.93, 11.73), respectively. However, rates of bleeding events in patients who continued or initiated nintedanib in the latest interim analysis of INPULSIS-ON (7.16 (5.52, 9.28) and 6.29 (4.47, 8.85]), respectively) were similar to the rate reported in the placebo group in the INPULSIS trials.33 In postmarketing surveillance data collected in the USA in the year following the launch of nintedanib, the rate of bleeding events was similar to the rate reported in patients treated with nintedanib in the INPULSIS trials (11.9 per 100 patient-years).38
Inhibition of VEGF has also been linked to an increased risk of gastrointestinal perforation.41 Nintedanib should be used with caution in patients with recent abdominal surgery due to this potential risk. In the INPULSIS trials, gastrointestinal perforation was reported in two patients (0.3%) treated with nintedanib and none treated with placebo.18
Nintedanib should be used with caution in patients at higher cardiovascular risk, including those with coronary artery disease.6 7 Cardiac disorder adverse events occurred in similar proportions of patients treated with nintedanib versus placebo in the INPULSIS trials (10.0% vs 10.6%, respectively).18 A higher proportion of patients treated with nintedanib than placebo had a myocardial infarction (2.7% vs 1.2%), while a lower proportion had other ischaemic heart disease events (1.7% vs 3.1%).18 The incidence rates of myocardial infarction in the nintedanib and placebo groups in INPULSIS were 1.68 and 0.48 per 100 patient–years, respectively. Incidence rates of myocardial infarction from the latest interim analysis of data in patients continuing or initiating nintedanib in INPULSIS-ON were 0.70 and 0 per 100 patient–years, respectively.33 The incidence rates of major adverse cardiovascular events in the nintedanib and placebo groups in INPULSIS were 3.92 and 2.67 per 100 patient–years, respectively, and in patients continuing or initiating nintedanib in INPULSIS-ON were 2.94 and 1.98 per 100 patient–years, respectively.33
Nintedanib is not recommended for use in patients with moderate or severe liver impairment. Patients with ALT or AST or bilirubin >1.5 ULN were excluded from the TOMORROW and INPULSIS trials.16 18 Liver function tests (ALT, AST and bilirubin) should be conducted prior to treatment with nintedanib, monthly for 3 months, every 3 months thereafter, and as clinically indicated, and liver enzyme elevations managed through dose reduction, treatment interruption and permanent treatment discontinuation.7
There are no data to support the efficacy of a combination of nintedanib and pirfenidone in patients with IPF, and there is some overlap in the adverse events associated with these medications. Trials of combination therapy with nintedanib and pirfenidone (ClinicalTrials.gov NCT02598193, NCT02579603) are ongoing and will report results soon.
What non-pharmacological therapies should I consider when treating patients with nintedanib?
Patients diagnosed with IPF understand their poor prognosis, but many have little understanding of how their disease will progress and how it will be managed.42 Patient education is crucial and should be tailored to address patients’ individual needs.43
Lung transplantation should be considered as a treatment option for patients with IPF who meet eligibility criteria. Patients with IPF should be referred for evaluation for lung transplantation as soon as possible to maximise the chance that they will be eligible.1 44 There are very few data on outcomes in patients treated with nintedanib who undergo lung transplantation and practice varies among treatment centres as to whether nintedanib may be continued until lung transplantation in patients with IPF.
Non-pharmacological therapies recommended for patients with IPF include pulmonary rehabilitation, supplemental oxygen and palliative care.1 Pulmonary rehabilitation consists of a programme of exercise training, education and patient support designed to improve patients’ physical and psychological condition.45 There is a growing body of evidence that pulmonary rehabilitation improves exercise capacity, dyspnoea and quality of life in patients with IPF, at least in the short term.46 47 International treatment guidelines for IPF recommend that patients with clinically significant resting hypoxaemia (commonly defined as a resting arterial oxygen saturation <88%) should receive long-term oxygen therapy.1 There are no recommendations regarding the use of supplemental oxygen in patients with exertional hypoxaemia.1 A systematic review of articles on the impact of oxygen therapy in patients with interstitial lung disease suggested, based on data from 12 studies, that short-term oxygen therapy had no effect on dyspnoea during exercise, although exercise capacity was increased.48
Palliative care focuses on reducing patient’s symptoms and providing comfort and should be individualised to meet the needs of patients and their caregivers.1 There is a growing consensus that patients with IPF should have access to palliative care at all stages of the disease, not just at end of life, to preserve quality of life.49
Conclusions
Nintedanib has been approved for the treatment of IPF in several countries and regions, including the USA and Europe, and received a conditional recommendation for use in the latest international treatment guidelines. Placebo-controlled trials have shown that nintedanib reduces the rate of disease progression in patients with IPF, with adverse events that are manageable in most patients through dose reduction, treatment interruption and symptomatic management of diarrhoea. Nintedanib has been shown to be effective across a wide range of subgroups of patients with IPF. Caution should be used in using nintedanib in patients with known risk of bleeding and in patients with high risk of cardiovascular disease such as those with coronary artery disease. Non-pharmacological therapies are an important part of the management of patients with IPF and should be individualised to the needs of the patient.
Acknowledgments
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). The authors received no direct compensation related to the development of the manuscript. Writing support was provided by Sorcha Wahlkvist and Wendy Morris of FleishmanHillard Fishburn, London, UK, which was contracted and funded by Boehringer Ingelheim Pharmaceuticals, Inc. Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
References
Footnotes
Contributors The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE).
Funding The authors received no direct compensation related to the development of this article. Page processing and open access charges for this article have been paid by Boehringer Ingelheim Pharmaceuticals, Inc.
Competing interests Amy Case reports personal fees from Boehringer Ingelheim outside the submitted work. Peace Johnson reports no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.