Article Text

Abstract
Introduction Pulmonary arteriovenous malformations (PAVMs) may not be amenable to treatment by embolisation or surgical resection, and many patients are left with significant hypoxaemia. Lung transplantation has been undertaken. There is no guidance on selection criteria.
Methods To guide transplantation listing assessments, the outcomes of the six patients who had been considered for transplantation were compared with a similarly hypoxaemic patient group recruited prospectively between 2005 and 2016 at the same UK institution.
Results Six patients had been formally considered for lung transplantation purely for PAVMs. One underwent a single lung transplantation for diffuse PAVMs and died within 4 weeks of surgery. The other five were not transplanted, in four cases at the patients’ request. Their current survival ranges from 16 to 27 (median 21) years post-transplant assessment.
Of 444 consecutive patients with PAVMs recruited between 2005 and 2016, 42 were similarly hypoxaemic to the ‘transplant-considered’ cohort (SaO2 <86.5%). Hypoxaemic cohorts maintained arterial oxygen content (CaO2) through secondary erythrocytosis and higher haemoglobin. The ‘transplant-considered’ cohort had similar CaO2 to the hypoxaemic comparator group, but higher Medical Research Council (MRC) dyspnoea scores (p=0.023), higher rates of cerebral abscesses (p=0.0043) and higher rates of venous thromboemboli (p=0.0009) that were evident before and after the decision to list for transplantation.
Conclusions The non-transplanted patients demonstrated marked longevity. Symptoms and comorbidities were better predictors of health than oxygen measurements. While a case-by-case decision, weighing survival estimates and quality of life will help patients in their decision making, the data suggest a very strong case must be made before lung transplantation is considered.
- Lung Transplantation
- Ambulatory Oxygen Therapy
- Thoracic Surgery
- Systemic disease and lungs
- Rare lung diseases
- Paediatric Lung Disaese
- Imaging/CT MRI etc
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Lung Transplantation
- Ambulatory Oxygen Therapy
- Thoracic Surgery
- Systemic disease and lungs
- Rare lung diseases
- Paediatric Lung Disaese
- Imaging/CT MRI etc
Introduction
Pulmonary arteriovenous malformations (PAVMs) are abnormal vessels that provide direct communications between pulmonary arteries and veins, and an anatomic right-to-left shunt.1 There are extensive references within early surgical literature detailing the structural characteristics,2–8 natural history in large series,4 8 9 surgical models,10 successful responses to surgical resection and limitations of surgery when disease was widespread. With the advent of embolisation treatment,11–13 treatment modalities evolved and the majority of patients are now treated by endovascular embolisation14–19 Surgical resection is undertaken in selected cases, particularly in emergency settings for haemoptysis if embolisation facilities are not available, or where pulmonary embolisation therapy is difficult or unsuccessful for patients experiencing PAVM complications.20–24 Unfortunately, PAVMs are often technically too small and/or numerous for curative embolisation or surgical procedures, and many treated patients are left with residual right-to-left shunts.
Population-wide CT screening programmes (undertaken for lung cancer screening) suggest as many as 1 in 2600 individuals will have a PAVM.25 The vast majority have no respiratory symptoms, usually because the PAVM(s) are small. In addition, for those with hypoxaemia secondary to their right-to-left shunting, as for high altitude adaptation,26 compensation occurs through polycythaemia and haemodynamic responses.27–31 A small proportion of patients experience haemoptysis, although this is infrequent except in the settings of pregnancy (1.0% of PAVM pregnancies result in life-threatening pulmonary haemorrhage32); pulmonary hypertension33 or if there is a systemic arterial supply to the PAVM sac: systemic arterial supply may arise de novo, or as a consequence of previous embolisation,34–36 surgical treatments20 or intercurrent lung parenchymal conditions.37 38 Haemoptysis may also occur due to endobronchial or nasopharyngeal telangiectasia39 if PAVMs are associated with hereditary haemorrhagic telangiectasia (HHT).40 HHT is a multisystemic inherited vascular dysplasia which also leads to arteriovenous malformations in visceral vascular beds, and iron deficiency anaemia as a result of recurrent bleeds from nasal and gastrointestinal telangiectasia.41
Independent of HHT pathology and anaemia, there is a subgroup of patients who have significant dyspnoea attributable to their PAVMs. Other respiratory symptoms are less frequent: chest pain is not considered a feature of untreated PAVMs, and major haemoptysis is rare. Usually, the most important risks from PAVMs relate to the loss of pulmonary capillary bed filtration of particulate material resulting in paradoxical embolic strokes,42–44 cerebral abscess42 43 45 46 and migraines.47 For reported cases presenting prior to 1999, >30% experienced paradoxical strokes or cerebral abscess.42 While some progress has been made identifying which patients are at greater risk of these neurological complications,43–47 there has been little improvement in overall complication rates,46 since the majority of patients with PAVMs are undiagnosed prior to their first cerebral abscess or ischaemic stroke.43–46
Lung transplantation has been performed if PAVMs were not amenable to treatment by embolisation or surgical resection.48–52 Reported follow-up periods for patients with PAVM receiving lung transplantation were short, but included at least one operative death.52 At the same time, the survival of cases in whom lung transplantation had been considered but not performed, was being recognised, and at many institutions, once these exceeded lung transplantation survival figures, the option of lung transplantation was rarely, if ever considered.34 52–55
Morbidity in severely affected individuals within the non-transplanted cohort, and the limited appreciation of how patients with PAVMs differ to other hypoxaemic patients27–31 56 prompted the more detailed evaluation reported in this manuscript. The aim of this study was to explore evidence in support of transplantation listing by evaluating long-term outcomes of patients considered for transplantation and comparing with a similarly hypoxaemic patient group.
Methods
Study population and assessments
The study subjects were cohorts of patients with radiologically diagnosed PAVMs, prospectively recruited at a single UK institution.
All evaluations, including pulmonary function, red cell and iron measurements, were performed as part of routine clinical care. Oxygen saturation (SaO2) was measured by pulse oximetry in the erect posture for 10 min, with the mean value of 7–10 min recorded for serial evaluations, since this better reflects right-to-left shunt size than SaO2 in other postures.27 57 58 Contrast echocardiograms were not performed routinely, as serial SaO2 provide a more discriminatory index of right-to-left shunt severity for patients with CT-evident PAVMs.1 44 45 Where indicated, PAVM embolisation was performed as described elsewhere with pulmonary artery pressure measured prior to contrast injection.16 Patients were followed-up locally and/or at our institution as described.27 43 44
In keeping with the Curaçao criteria,59 HHT was diagnosed in the presence at least three criteria from epistaxis, characteristic telangiectasia, visceral involvement and an affected first-degree family member. Reported exercise tolerance was assigned to the MRC dyspnoea scale60 using a modification employed by us to distinguish athletic from other normal individuals.27 61 Thus, grade 1 (normal, only breathless on strenuous exertion) was subdivided into grade 1a (performing intense sporting activity at least three times a week), or grade 1b (other individuals only breathless on strenuous exertion).27 61 As in the original MRC dyspnoea scale,60 grade 2 represented breathless on a slight hill, grade 3 breathless/having to stop after a mile; grade 4 breathless after walking a few minutes (about 100 m) and grade 5 breathless at rest or minimal effort.
Arterial oxygen content (CaO2) breathing room air was calculated by SaO2 × haemoglobin × 1.34/100, where SaO2 was expressed as a per cent and 1.34mL is the empirically determined amount of oxygen carried per gram of haemoglobin.62
Study cohorts
Cohort origins are illustrated in figure 1.
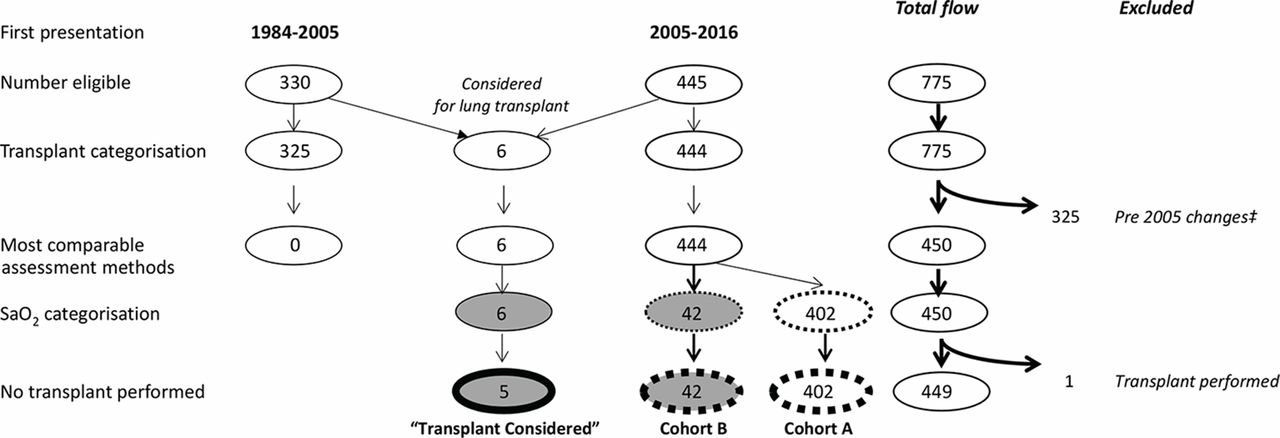
Study flow chart. The cohort of 330 patients who first presented to our institution between 1984 and 2005 included five individuals considered for lung transplantation, compared with only one from the cohort of 445 who were first assessed between 2005 and 2016. ‡It was not possible to compare the presentation values of the 1984–2005 cohort to the final lung transplant-considered group due to the changes in clinic assessments over the period. In particular, routine dyspnoea and iron (ferritin) assessments changed in 2005, as described in references 27 and 44. Cohorts A and B were categorised by SaO2: cohort A had resting SaO2 on air of ≥86.5%, cohort B <86.5%.
Consecutive patients who had been considered for lung transplantation at any time between 1984 and 2016 were studied. Consideration for transplantation was made on a case-by-case basis, primarily based on symptoms and perceived life expectancy. Clinical details at the time of their assessment for lung transplantation, and at latest follow-up in 2016/2017, or prior to their recorded death, were evaluated. The patients who did not receive a lung transplant are referred to as the ‘transplant-considered’, that is, ‘transplant-considered (but not performed)’ cohort.
The full comparator population were the 445 patients with PAVMs reviewed for the first time at our institution between June 2005 and December 2016. Full details of this population and susceptibility to cerebral abscess are reported elsewhere.46 One individual had been referred for a lung transplant prior to review, leaving 444 patients who were/had not been considered for transplant, and were categorised by their presentation SaO2. Cohort A had resting SaO2 on air of ≥86.5%. Cohort B (the transplant-comparator cohort) had SaO2 <86.5%. The category boundary was selected because all SaO2 values in the transplant-considered group were ≤86%.
Statistical analyses
STATA IC 13.1 (StataCorp, College Station, Texas, USA) was used to generate descriptive statistics, to compare data sets and to perform Kaplan-Meier survival analyses. Two group comparisons were performed by Mann-Whitney U test, three group comparisons by Kruskal-Wallis test. In Kaplan-Meier analyses, T=0 represented the start of follow-up after consideration for transplant at median age 21.5 years (transplant-considered cohort), or for cohorts A and B, the age of 22 to reduce bias (note PAVMs are usually fully developed by the end of puberty).1 28 GraphPad Prism 5.04 (GraphPad Software, San Diego, California, USA) was used to generate additional graphs.
Results
Demographics of transplantation cohort
Of 755 individuals with PAVMs assessed and treated at our institution,43 46 63–65 6 (0.8%) patients were formally considered for lung transplantation.
Four had undergone transplantation assessments as adults, and two as children. Ages ranged from 2 to 47 (median 22) years. Four were from the UK (including three referred from our institution between 1988 and 1993), and two had been assessed in the non-UK countries. All had a clinical diagnosis of HHT 59 with at least three Curaçao criteria (see online supplementary table 1).
All had disease that could be classified as ‘diffuse’ with multilobe involvement remaining after maximal embolisation. At the time of consideration for lung transplantation, the adults had undergone maximal embolisation of PAVMs and had PAVMs too extensive to be considered for surgical resection (one had previously undergone surgical resection as a child). The children were considered to have untreatable disease. SaO2 ranged from 73% to 86% (median 79%) on air. Two of the six had suffered a cerebral abscess due to their PAVMs, and two were venesected regularly for polycythaemia (see online supplementary table 1).
Transplantation assessment outcomes
One of the six underwent lung transplantation. The other five were not transplanted, in four cases at the patients’ request. Stated reasons included young family (n=3), potential interactions of immunosuppression drugs with anti-epileptic therapy (n=1) and in all cases, a strong preference for their existing health state.
The patient who was transplanted died within 4 weeks of surgery, a different PAVM lung transplantation death to the one reported by Pierucci et al.34 The cause of death was multiorgan failure precipitated by a series of postoperative complications: severe epistaxis and anaemia, a transient ischaemic attack and renal failure with anasarca, although no overt infection. At the time of death, the function of the transplanted lung was good with SaO2 92% compared with 74% preprocedure.
Currently, the survival of the five patients who were not transplanted ranges from 16 to 29 (median 21) years, with three of the five still alive (figure 1). One of the ‘transplant-considered’ cohort survived three successful pregnancies. Survival is therefore significantly higher than the International Society for Heart Lung Transplantation 2016 median survival figures across all pathologies of 5.7 years for adults, 5.4 years for children67](p<0.01) and 10-year survival rates (48%) reported at one UK transplant centre68 (p<0.01).
Morbidity after assessment for lung transplantation
While all five received further embolisation over the subsequent two to three decades, all were left with residual, severe right-to-left shunting. At the time of the most recent or final assessment, SaO2 on room air ranged from 73% to 86% (median 83.5%). Four of the five required long-term oxygen supplementation, and exhibited marked reduction in exercise tolerance but the fifth, one of the two children referred, has had a more indolent course and is able to exercise and work normally. Thus, MRC dyspnoea grades vary from 1 to 5 (median 3). Only one experienced low-grade haemoptysis. Two experienced long-term disabling pain and were diagnosed with hypertrophic pulmonary osteoarthropathy. It was not known whether PAVM-induced hypoxaemia or paradoxical emboli may have contributed to epilepsy and/or significant mental health issues considered to be the cause of a self-inflicted death.
One had a first cerebral abscess during follow-up, and another a second cerebral abscess which was fatal. Three of the five (60%) also developed a venous thromboembolus (VTE-deep vein thrombosis or pulmonary embolus) in the follow-up period. Although VTE is a common consequence of PAVM-induced cerebral abscess,43 46 none of these three events were related temporally to a cerebral abscess: all intervals exceeded 5 years, and one VTE preceded an abscess by 10 years. Two of the five patients tolerated short-term anticoagulation, while a third was anticoagulated for 15 years after the insertion of a caval filter to prevent further pulmonary emboli. Due to very high haemoglobins, one is assessed regularly for hyperviscosity symptoms that would precipitate further venesection.69
Comparison between ‘similarly hypoxaemic’ and less hypoxaemic 2005–2016 cohorts
The cohort prospectively recruited between 2005 and 2016 who were comparably hypoxaemic (SaO2 <86.5%) to the transplant-considered cohort were older than the less hypoxaemic cohort A (median ages 61 vs 47 years, p=0.0082). Both groups had similar proportions of females (59.5%, 60.2%), and underlying HHT (92.3%, 95.8%, online supplementary table 2).
Despite the non-overlapping oxygenation parameters (median SaO2 82.9% and 95%, p<0.0001), CaO2 was no lower in the more hypoxaemic cohort (median 173 and 174 mls of oxygen/L, p=0.38, table 2). supplementary table 2). As for the transplant-considered cohort, this was achieved through higher red cell number, and was not attributable to iron-deficient indices in less hypoxaemic patients (table 1, online supplementary table 2).
Comparison of comparator PAVM cohorts
Notably, the hypoxaemic cohort were more likely to have the right-to-left shunt complication of cerebral abscess, with no clear difference in ischaemic stroke rates (table 1).
Comparison between ‘transplant-considered’ and ‘similarly hypoxaemic’ cohorts
Compared with the similarly hypoxaemic cohort B, the transplant-considered cohort were significantly more dyspnoeic (figure 2A). This was despite very similar SaO2 (figure 2B), and a trend to higher arterial oxygen content (CaO2) in the transplant-considered cohort (figure 2C). Our previous studies have hinted that higher pulmonary artery pressures or airflow obstruction may impede compensations,27 61 but this was not evident for the transplant-considered cohort (table 2).However, all three adults with grade 3 or more dyspnoea demonstrated highly abnormal lung function. One patient with a previous lobectomy and hemiparesis had a restrictive ventilatory defect (vital capacity ≤64% predicted, online supplementary table 3). Two further cases displayed low gas transfer (TLCO and TLCO/VA <60% predicted, online supplementary table 3), potentially attributable to PAVMs, although one had biopsy-proven pulmonary fibrosis, and the other displayed additional symptoms of hypoxaemia (online supplementary table 4), and was at risk of further pulmonary emboli.

Dyspnoea and oxygenation parameters. The five cases considered for transplant, as assessed at their most recent follow-up, compared with 29 similarly hypoxaemic cases who were a subgroup of cohort B in whom presentation clinic assessments were rigorously evaluated between 2005 and 2010 (to generate blinded MRC dyspnoea scores as described in references 27and 61). (A) Modified MRC dyspnoea scale. (B) SaO2 and (C) CaO2. Box plots indicate median (line) and IQR, error bars represent two SD. Note that the comparator population were able to benefit from subsequent treatments. p Values were calculated by Mann-Whitney U test.
Comparative demographics between transplant-considered and similarly hypoxaemic PAVM cohort.
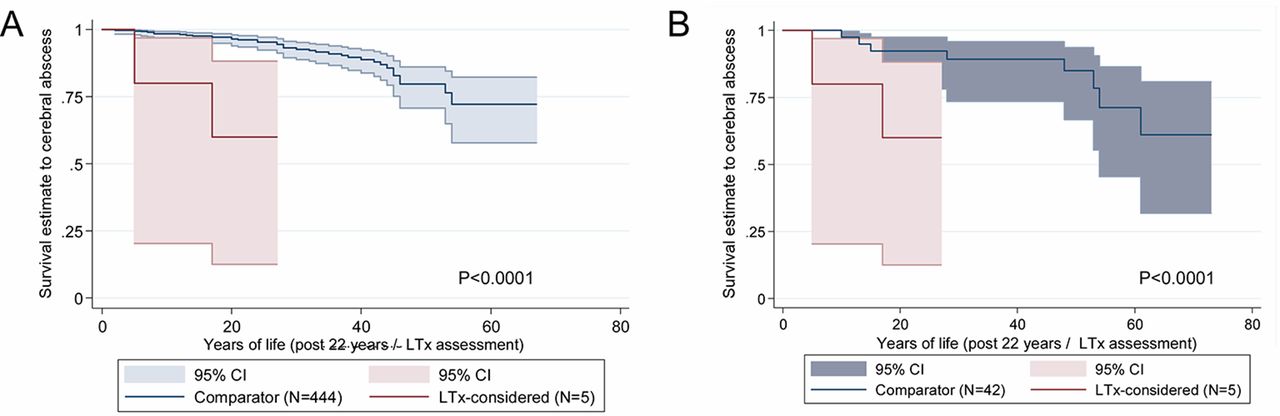
Compared with the similarly hypoxaemic cohort B, the transplant-considered cohort also had a greater burden from PAVM complications (cerebral abscess, ischaemic stroke) and VTE (table 2). To exclude prior events that may have increased the likelihood of transplant referral, comparisons were made from the time of transplant consideration, comparing the transplant-considered cohort to the other patients from an equivalent age (median 22 years). Calculated in this manner, cerebral abscess-free survival was significantly lower in the transplant-considered cohort than for all 444 individuals in the 2005–2016 cohort not considered for lung transplantation (p=0.0001, figure 3A). Surprisingly, the transplant-considered cohort were more likely to develop a cerebral abscess in follow-up post-assessment than similarly aged (from 22 years), similarly hypoxaemic (SaO2 <86.5%) patients in the period prior to their treatment (p<0.0001, figure 3B).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier comparisons of cerebral abscess risks. (A) The five cases considered for transplant (LTx-considered), compared with the full comparator cohort of 444 patients (cohorts A+B). T=0 represents the start of the follow-up after consideration for transplant (LTx-considered, at median age 21.5 years) or 22 years for the comparator cohort of 444 patients. (B) The same five cases considered for transplant (LTx-considered), compared with the comparably hypoxaemic comparator cohort of 42 patients (cohort B). Again, T=0 represents the start of follow-up after consideration for transplant (LTx-considered, at median age 21.5 years) or 22 years for the comparator cohort of 42 patients.
Patient perspective
For the four patients declining transplantation, all confirmed their decision to decline lung transplantation on multiple occasions, including at their most recent follow-up assessment. All reiterated a strong preference for their existing health state, despite the additional complications since their transplantation evaluations. One noted that they had outlived all of their original cohort at the lung transplant clinic.
Discussion
This is the largest series of PAVM cases categorised by severity of hypoxaemia, permitting a rigorous examination of parameters that may be judged as indicators for lung transplantation. This is important in a rare disease field where the literature is dominated by single case reports of short-term outcomes post lung transplantation.48–52 The manuscript provides evidence to help guide management of the more severely affected individuals with PAVMs in whom embolisation and surgical resection are unable to substantially reduce right-to-left shunting and restore near-normal oxygenation parameters. Arterial oxygen content was maintained, and the transplant-considered cohort who did not receive a lung transplant, displayed very long-term stability. However, the hypoxaemic PAVM cohorts experienced substantial morbidity.
Generally for patients with PAVM, information is becoming more reassuring. The hypoxaemic patients provide a powerful reminder of haematological compensations that are successfully employed to maintain arterial oxygen content (CaO2). There is greater evidence of benefits from PAVM treatments, and there are more options for supportive management. Overall clinical awareness is also increasing, as indicated by the shorter time to obtain a diagnosis of PAVMs in more recent series.46 Nevertheless, for anatomical reasons, some PAVMs are less amenable to treatment. At our institution, the survival of cases in whom lung transplantation had been considered but not performed, soon exceeded the most optimistic lung transplantation survival figures53–55 and no further cases were referred. Similar sentiments have been expressed by other groups with very extensive experience managing patients with PAVMs.34 52 Successful short-term lung transplantation outcomes are reported however,48–51 and there are good very long-term outcomes for patients with HHT receiving orthotic liver transplants for hepatic AVMs.70–73 Together with substantial morbidity experienced by many of the lung transplant-referred cohort at our institution, this prompted the more rigorous comparative evaluations reported in this manuscript.
The transplant-considered cohort were substantially more dyspnoeic than the comparator cohort of 42 patients with similarly severe right-to-left shunting through PAVMs. Patients with PAVM right-to-left shunts need to ventilate more to exhale CO2.29 This may accentuate the significance of modestly reduced ventilatory capacity,27 61 which could be important if surgery is being considered for PAVMs that will not be fully resected.
Surprisingly, thromboembolic complication rates that should be independent of ventilation were also higher in the transplant-considered cohort, assuming that years of PAVM life pretreatment can be compared with years after treatment. This assumption may not be fully valid, and given the cohort sizes, it is possible the events reflect mere coincidence, but we suggest further exploration is needed for factors rendering individuals less able to tolerate the circulatory consequences of right-to-left shunts.27–34 43–47
In our experience, it is difficult for patients to weigh risks of future individual events (such as a cerebral abscess), as opposed to a current symptomatic state. For the patient who was transplanted, her quality of life was deteriorating and despite the poor outcome, lung transplantation would still be considered her best option at the time. For the patients who declined transplantation, it is not known whether their judgements would have been influenced if there were more formal quantification of long-term neurological implications of hypoxaemia and recurrent paradoxical emboli. However, despite experiencing additional complications, this did not alter their perspective.
In conclusion, patients with PAVMs causing severe hypoxaemia demonstrate pronounced longevity with reasonable quality of life; lung transplantation, with all its risks, is rarely performed, and usually refused by the patient if it is suggested. Nevertheless, such patients remain at risk of major complications attributable to PAVMs. The current data suggest a sensitive discussion about the potential risks of residual PAVMs is needed, particularly for patients remaining symptomatic from severe right-to-left shunting following maximal standard treatments. While in highly selected symptomatic cases, exploration of lung transplantation options may be considered a reasonable approach, a very strong case, based on parameters other than oxygenation/longevity, would need be made.
Acknowledgments
The authors thank the patients, and their many colleagues at Hammersmith Hospital. The authors particularly thank Abeer Rizvi for transcribing the serial spirometric data as part of studies for reference.28
References
Footnotes
Contributors CLS assessed and treated patients (1999–to date), set up the prospective characterisation series, performed the notes evaluations, statistical evaluations, and figure generation, and wrote the manuscript. EB assessed and treated patients. DJA assessed and treated patients (1984–1999), developed interventional treatment modalities and referred one case for lung transplantation. JMBH assessed and treated patients (1988–1999), developed physiological assessment modalities and referred two cases for lung transplantation. JEJ assessed and treated patients (1985–to date) and developed interventional treatment modalities. All authors contributed to and approved the final version of this manuscript.
Funding Funding was received from patient family donations, particularly the Donald Ralph and Thomas Ralph Memorial Fund. Professor Shovlin and Dr Jackson also acknowledge support from the NIHR Imperial Biomedical Research Centre.
Competing interests None declared.
Ethics approval This study was conducted in accordance with the amended Declaration of Helsinki. The Hammersmith and Queen Charlottes Local Research Ethics Committee (LREC 2000/5764) approved the protocol.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors agree with the principles of data sharing: anonymised data will be provided on reasonable request.