Article Text

Abstract
Introduction Endobronchial valve placement has potential as a treatment for patients with chronic obstructive pulmonary disease (COPD). However, a robust evidence base will be needed to convince commissioners of healthcare that it is a high-value treatment. We sought to develop the evidence base by performing an individual patient-level analysis of randomised controlled trials in people with heterogeneous emphysema and an absence of collateral ventilation.
Methods A literature search (PROSPERO register CRD42016048127) identified two trials meeting these criteria, the BelieVeR-HIFi and STELVIO studies. Anonymised individual patient data were obtained from investigators and analysed. The primary outcome measure was a comparison of change in forced expiratory volume in 1 s (FEV1) from baseline between the treatment and control groups. Secondary end points were change from baseline in 6 min walk distance (6MWD), Medical Research Council dyspnoea score and St George’s Respiratory Questionnaire (SGRQ).
Results 114 individuals were treated with 3-month to 6-month follow-up data available for 101 individuals. FEV1 improved by 23.1 (±28.3)% in patients treated with valves with a mean (95% CI) difference in response between groups of 17.8 (26.5, 9.2)% (p<0.0001). Relative to controls valve placement was associated with a fall in residual volume of 0.64 (0.43, 0.86) L (p<0.0001), a 9.5 (3.5, 15.6) unit fall in SGRQ (p=0.0022) and a 64.2 (94.0, 34.5) m increase in 6MWD. There were three deaths in the treatment arm and the pneumothorax rate was 15%.
Conclusions These data strengthen the evidence that endobronchial valve treatment can produce clinically meaningful improvements in appropriately selected COPD patients.
- bronchoscopy
- emphysema
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Can endobronchial valve placement improve health outcomes in selected patients with heterogeneous emphysema and an absence of collateral ventilation
Endobronchial valves improve lung function, exercise capacity and health status at 3–6 months after the procedure
Combining patient-level data from randomised controlled trials of bronchoscopic lung volume reduction with endobronchial valves strengthens the evidence that this therapy can improve lung function, exercise capacity and quality of life in appropriately selected patients with heterogeneous emphysema and absence of interlobar collateral ventilation.
Background
Chronic obstructive pulmonary disease (COPD) is characterised by the presence of bronchitis and emphysema. The latter process, due to breakdown of elastic alveolar tissue, leads to increased lung compliance and gas trapping. Lung hyperinflation worsens with exercise leading to breathlessness and is associated with reduced physical activity1 2 and reduced survival.3 Inhaled bronchodilator medications have only modest impacts on symptoms and do not alter the natural history of the disease. In selected patients with a heterogeneous pattern of emphysema, surgical resection can be targeted at the worst affected areas of lung tissue which contribute disproportionately to gas trapping and hyperinflation, and so improve respiratory mechanics.4 5 Lung volume reduction surgery (LVRS) improves symptoms and prolongs survival6–8 but can be associated with significant morbidity and a risk of death, with a cost per quality adjusted life year (QALY) of at least $40 000.9
A more recent approach has been to instead use endobronchial valves to occlude the airways supplying the worst affected part of the lung.10–13 This is intended to cause atelectasis in the target lobe, with a similar impact on the function of the rest of the lung as seen in LVRS. However, atelectasis will only occur in the absence of significant collateral ventilation between the target lobe and the adjacent one. Because of this, the success rate of valve placement in early studies was low, impacting on the value of endobronchial valves as a therapeutic intervention.13–15 Collateral ventilation can now be measured directly using the Chartis pressure/flow catheter system.16–18
Case series and single-centre trials have demonstrated that endobronchial valve treatment in patients with emphysema can lead to improvements in symptoms, lung function and exercise capacity,11–13 reductions in dynamic hyperinflation19 and improvements in oxygen kinetics20 and chest wall synchrony.21 Moreover, where target lobe volume loss is seen on CT, a substantial survival benefit has been observed compared with those where valve treatment has been ineffective.14 15
We wished to combine data from existing single-centre studies to address the question ‘in patients with emphysema and a target lobe with proven absence of interlobar collateral ventilation, what is the effect of endobronchial valves placed to achieve lobar occlusion, on lung function, exercise capacity and health status?’
Methods
The study was registered on the PROSPERO International prospective register of systematic reviews CRD42016048127. We searched PubMed using the terms ‘endobronchial valves (AND) emphysema’ on 22 September 2016. This identified 116 abstracts. Twelve of these were clinical trials. Review of the abstracts identified two trials where patients with emphysema were randomised to endobronchial valve placement or standard care with identification of the presence of interlobar collateral ventilation using the Chartis system (Pulmonx).11 12 Complete, anonymised, individual patient data were obtained from the investigators for analysis.
Data were checked for: missing items, internal data consistency and randomisation integrity. Summary tables were checked with the trial protocol and latest trial report or publication.
The primary outcome measure was a comparison of change in forced expiratory volume in 1 s (FEV1) between the endobronchial valve treatment and control groups. Secondary end points were change from baseline to 3 months (BeLieVeR-HIFi) or to 6 months (STELVIO) in 6 min walk distance (6MWD), Medical Research Council (MRC) dyspnoea score and St George’s Respiratory Questionnaire (SGRQ). The different time points in the two trials were merged as a measure of the effectiveness of the intervention because the impactof the intervention was expected to be much greater than spontaneous decline over a short period of time. Statistical analysis was carried out using StatView 5. Changes were compared between treatment and control groups using unpaired t-tests. Analysis of covariance using baseline values as a covariate together with treatment allocation and which study individuals were in was used to establish whether responses differed by study. Collateral ventilaion (CV)-positive patients (n=4) treated in the BeLieVeR-HIFi were excluded.
No ethical approval for this reanalysis of anonymised data was obtained.
Results
Literature search identified two studies. The UK-based BeLieVeR-HIFi trial (ISRCTN04761234) was a double-blind study which randomised 50 patients on a one-to-one basis to endobronchial valve placement, intended to achieve lobar occlusion11 or to bronchoscopy with a sham-bronchoscopy procedure. Patients were selected on the basis of hyperinflation, heterogeneous emphysema and interlobar fissure adjacent to the target lobe which appeared to be at least 90% intact. Allocation was by predetermined block randomisation, obtained by telephone link from the bronchoscopy suite after the patient had been sedated. Collateral ventilation was measured but patients were treated even if CV positive (n=4). For the purpose of the present analysis, the CV-positive patients were excluded, as they fall outside the hypothesis being addressed. Outcome measures were assessed at 3 months post procedure by investigators blind to study allocation. There were two deaths in the treatment arm, one because of complications of a valve removal procedure and one from cor pulmonale. One control patient was too unwell to attend for follow-up, so follow-up data were available for 24 control patients and 19 treated patients.
A second Dutch study (STELVIO trial—Netherlands Trial Register number, NTR2876) randomised 68 hyperinflated COPD patients, with a target lobe based on visual inspection of the CT, on a one-to-one basis to endobronchial valve placement or usual care.12 Allocation was performed using a randomisation list that had been computer-generated in blocks of four. The generated codes were placed in opaque-sealed envelopes, which were numbered sequentially. The assigned envelope was opened before bronchoscopy in the presence of the patient and bronchoscopist. Bronchoscopy was then performed. Eighty-four patients entered the study, but patients with collateral ventilation (n=13) or airways unsuitable for endobronchial valve placement (n=3) were excluded. Pulmonary function tests were assessed 6 months following the procedure by blinded assessors. One control patient withdrew. One treated patient died due to end-stage COPD with respiratory failure 58 days after treatment and one was withdrawn from the study by the investigators because of a prolonged admission to the critical care unit due to COPD exacerbation caused by a viral infection. Seven patients discontinued the study because their valves had been removed—two at patient request because of perceived lack of efficacy, two because of bronchial torsion, two because of recurrent pneumothorax and one because of pneumonia distal to valve. Follow-up data for this study were therefore available for 25 treated patients and 33 controls.
The BeLieVeR-HIFi trial was funded by the Efficacy and Mechanism Evaluation Programme, funded by the MRC and managed by the National Institute for Health Research (NIHR) on behalf of the MRC-NIHR partnership (EME 10/90/10). The valves used in the trial were provided free of charge by the device company, Pulmonx. The STELVIO trial was supported by a grant (171101008, to the University Medical Centre Groningen) from the Netherlands Organisation for Health Research and Development (ZonMw) and by innovation funding from the University Medical Centre Groningen. Valves were obtained commercially from Pulmonx (all catheters at regular market prices and all valves at 50% of the market list price).
Baseline data for 114 patients were available, 55% female, aged mean (SD) 60.2 (8.6) years, with a mean (SD) FEV1 30.6 (8.9)% predicted, with follow-up data available for 101 (treatment n=44 and control n=57). The groups were well matched for spirometry, gas transfer, symptoms, exercise capacity and BODE (BMI, obstruction, dyspnoea, exercise capacity) score, but the control group were more hyperinflated (table 1).
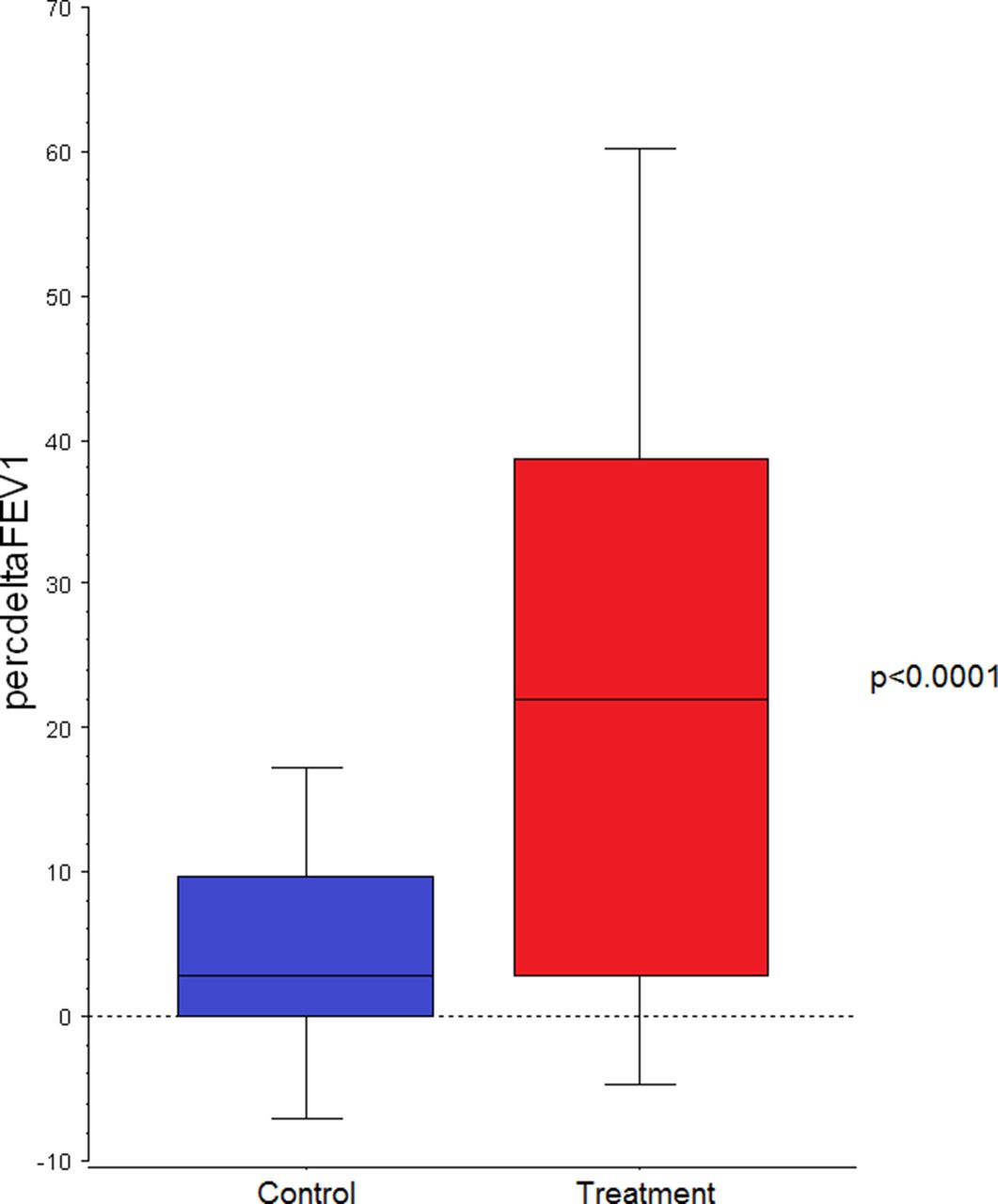
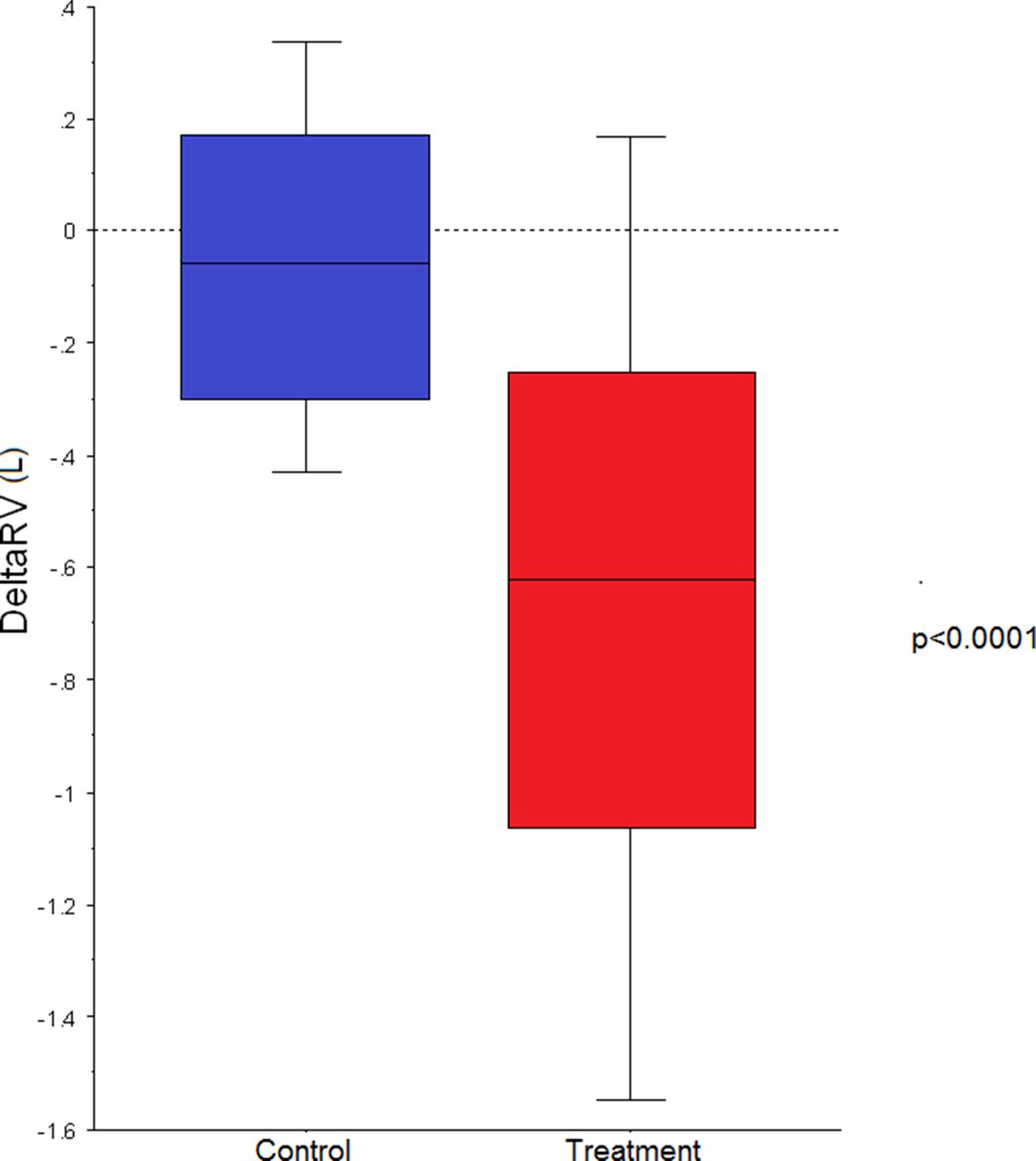
FEV1 improved by 23.1 (±28.3)% in patients treated with valves with a mean (95% CI) difference in response between groups of 17.8 (26.5, 9.2)% (P<0.0001) (figure 1, table 2). Valve placement was associated with statistically and clinically significant improvements in lung volumes (figure 2), exercise capacity (figure 3) and quality of life (figure 4). Outcomes did not differ significantly between the two trials for change in FEV1, residual volume 6MWD or SGRQ (P=0.79, 0.28, 0.16 and 0.21, respectively) although MRC dyspnoea score improved to a greater extent in the STELVIO study (P=0.002)
Baseline characteristics
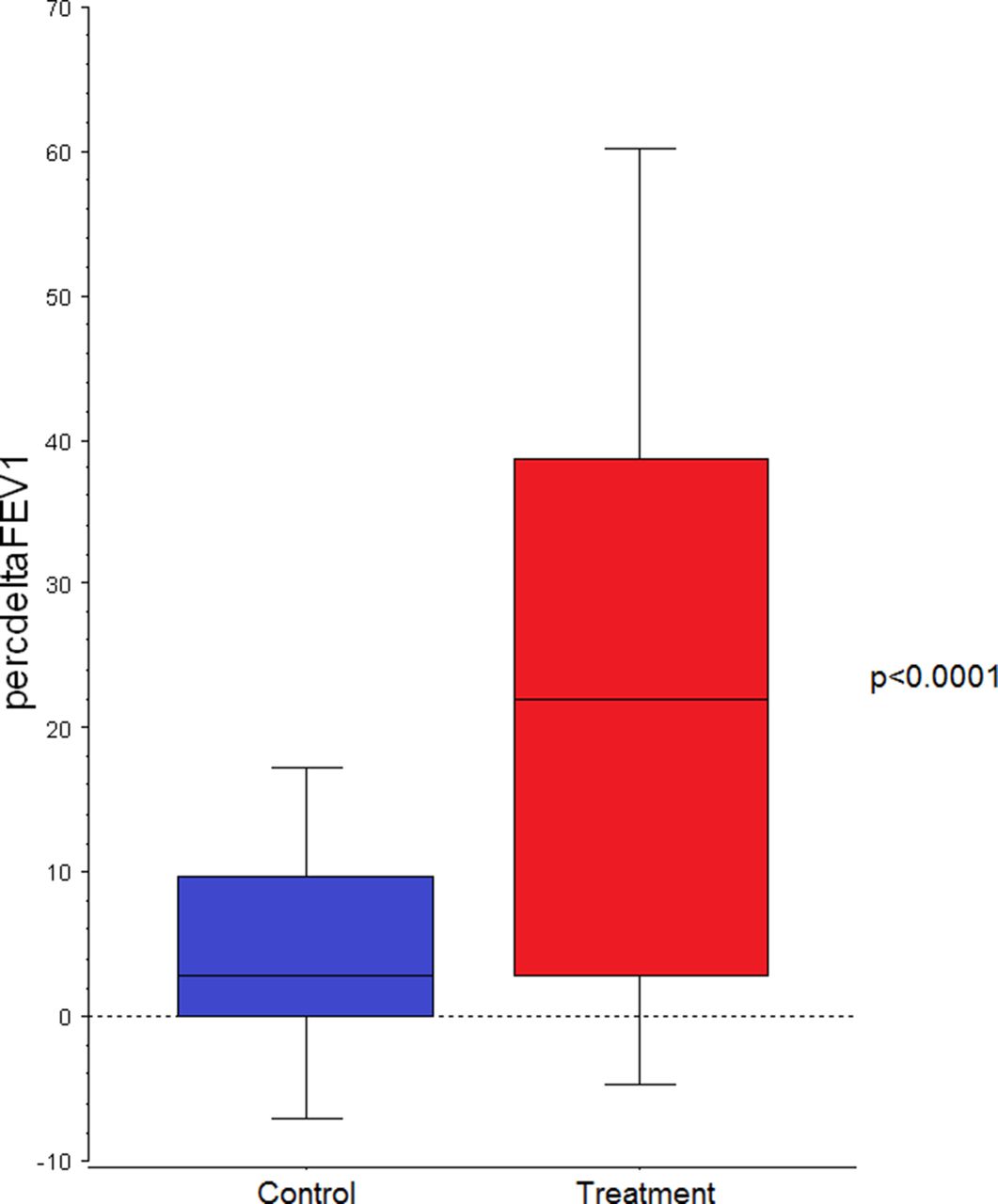
Percentage change in forced expiratory volume in 1 s (FEV1) in patients treated with endobronchial valves and control subjects. Boxes represent 25th–75th percentiles, bars 10th–90th percentiles (P<0.0001).
Response to treatment
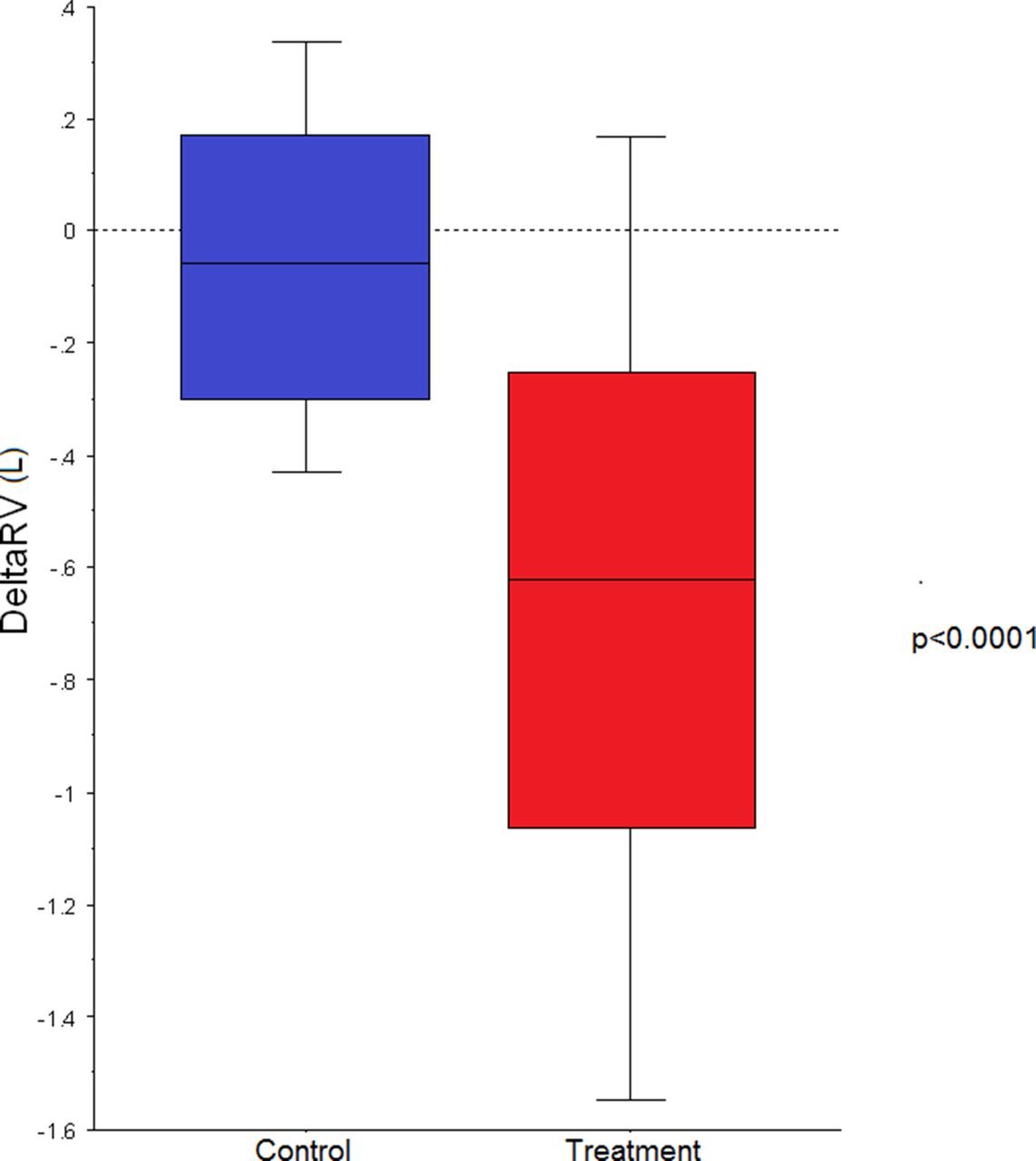
Change in residual volume (RV) in patients treated with endobronchial valves and control subjects. Boxes represent 25th–75th percentiles, bars 10th–90th percentiles (P<0.0001).

Change in 6 min walk distance (6MWD) in patients treated with endobronchial valves and control subjects. Boxes represent 25th–75th percentiles, bars 10th–90th percentiles (P<0.0001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in St George’s Respiratory Questionnaire (SGRQc) in patients treated with endobronchial valves and control subjects. Boxes represent 25th–75th percentiles, bars 10th–90th percentiles (P=0.0022).
Adverse events are described in table 3. There were a total of eight pneumothoraces in the treatment arm and one in a control subject during the follow-up period.
Serious adverse events
Discussion
The present data combine results from two randomised controlled trials which evaluated the impact of endobronchial valve placement to achieve lobar occlusion in patients with heterogeneous emphysema, where collateral ventilation had been excluded using the Chartis catheter system.11 12 They further strengthen the evidence that endobronchial valve treatment can, in appropriately selected patients, produce clinically meaningful improvements in lung function, exercise capacity and health status. The amplitudes of changes exceeded conventionally defined minimum clinically important differences (MCID)—a 15% increase for FEV1, 350 mL reduction for the residual volume,22 an increase of 26 m for the 6MWD23 and a 4-point decrease in the SGRQc.24 25 It also exceeds the more recently proposedMCID of 7 SGRQ points at 6 months for bronchoscopic interventions in advanced COPD.26
Methodological issues
We combined data from two studies which were similar in that they randomised patients with severe emphysema and a suitable target lobe to endobronchial valve placement or usual care. The trials were well conducted with study methodology including allocation and blinding clearly described with a low risk of bias. There were a number of differences between the studies, though we do not feel that they preclude combining the data as we have done. Follow-up was at 3 months in the BeLieVeR-HIFi study11 and 6 months in STELVIO,12 but the size of the response observed is significantly larger than the likely spontaneous decline over that time period. The former study included a control bronchoscopy, so participants were blind to treatment allocation whereas treatment was open label in STELVIO. This might have influenced response to questionnaires or exercise tests which are effort dependent, but in fact, improvements in these with treatment were similar between studies. Of note, the improvement in SGRQ score exceeded the 8-point threshold used in the National Emphysema Treatment Trial to allow for the lack of blinding in that study.6
Hazards of therapy
Our study extends the data available on harms associated with endobronchial valve placement. Acute exacerbation-like events are common in the early period after valve placemen. Pneumothorax remains a significant concern, occurring in 15% of individuals treated. Pneumothoraces occur because the valve placement has been effective, causing a change in the conformation of the lung which leads to tearing and air leakage. For this reason, pneumothorax was unusual in early trials,13 but the rate has increased as selection criteria for trials have become more precise.11 12 27 Most of these episodes respond to conventional treatment with an intercostal drain but they can be fatal, especially in a group of patients who already have significant ventilatory limitation. It is therefore recommended that patients should be observed for several days as an inpatient following the procedure.
Conclusion
This analysis provides further evidence for the efficacy of endobronchial valves as a therapeutic option in COPD patients with advanced emphysema. Longer-term data are becoming available suggesting that benefits, including survival benefits,14 of valve treatment are sustained and suggest that this may be a relatively high-value therapy in COPD,28 with a cost per QALY of approximately €25 000.29 Good outcomes from lung volume procedures will depend on a multidisciplinary approach and the development of effective referral pathways.7 8 28 30 Further work is needed to establish the relative long-term benefits of valve placement and LVRS. TheComparative Effectiveness of Lung volume reduction surgery for eEphysema and Bronchociopic valve placement (CELEB) trial is now underway to address this http://www.isrctn.com/ISRCTN19684749
This analysis was supported by the NIHR Respiratory Biomedical Research Unit at Royal Brompton and Harefield NHS Foundation Trust and Imperial College, London, UK.
References
Footnotes
Contributors KK, ZZ, CD, D-JS and PLS conceived the study and developed the search strategy. NSH performed the literature search, collected data, performed the analysis and wrote the first draft to which all authors contributed. All authors have approved the submitted version. NSH is the guarantor.
Funding This analysis was supported by the NIHR Respiratory Biomedical Research Unit at Royal Brompton and Harefield NHS Foundation Trust and Imperial College, London, UK.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf. NSH was principal investigator in a UK NIHR funded trial (BeLieVeR-HIFi) for which PulmonX provided endobronchial valves free of charge. PLS has been an investigator on studies funded by PulmonX, Uptake, Holaria, CSA Medical, Uptake Medical, Olympus and PneumRx/BTG and received consultancy fees from for Broncus, CSA Medical, Medtronic, Olympus, PneumRx/BTG and Pulmonx. KK received lecture fees from Pulmonx and devices for treatments, travel support, and grant support from PneumRx/BTG and Pulmonx. D-JS has been an investigator on studies funded by CSA Medical, Holaira, PulmonX and PneumRx/BTG and received consultancy fees from CSA Medical, Holaira, PneumRx/BTG and Pulmonx.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests to access the data can be made to the corresponding author.