Article Text

Abstract
Introduction Complete foreign body airway obstruction is a life-threatening emergency, but there are limited data on its epidemiology.
Methods We conducted a retrospective analysis of data collected routinely from London Ambulance Service calls coded as being for choking was undertaken for the calendar year of 2016.
Results There were 1916 choking episodes of significant severity to call for emergency assessment in London during 2016, 0.2% of total calls requiring an ambulance response, an average of 5.2 per day. The incidence increased at the extremes of age. Calls coded as choking occurred at times consistent with lunch and dinner and less frequently at breakfast. Peak incidence occurred at Sunday lunchtimes and on Wednesday evenings.
Conclusions Choking is a substantial health problem for Londoners to seek emergency assistance. Choking is more frequent at the extremes of age with a higher incidence at lunch and dinner time. Greater public awareness of choking and its management could help to prevent avoidable deaths.
- clinical epidemiology
- respiratory muscles
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Choking is a substantial health problem.
Choking is more frequent at extremes of age.
Choking has a higher incidence at lunch and dinner time. Greater public awareness of choking and its management could help to prevent avoidable deaths.
Introduction
Complete foreign body airway obstruction (FBAO) is a life-threatening emergency, but there are limited data on its epidemiology. In 1982, Mittleman et al 1 found the incidence of choking in the USA to be 0.66 per 100 000 per year. Vilke et al 2 reported that of emergency department (ED) attendances related to choking in San Diego, USA, 50% were in children aged less than 5 years. In adults, the incidence of choking appears to increase with age.3 The National Safety Council, USA, reports that FBAO is the fourth leading cause of ‘unintentional injury death’ with 5051 reported deaths in 2015 with 56% (2848 people) being over the age of 74.4 Establishing the true incidence of significant choking due to FBAO is difficult because many cases of choking may be managed without the assistance of the emergency services. The Office for National Statistics reports that there were 34 avoidable deaths in the UK related to choking in 20155 which is likely to be an underestimate.
Recognition of FBAO is key to early intervention. Choking normally occurs while the victim is eating or drinking and can be associated with muscle, neurological or cerebral impairment. The most common signs and symptoms of choking are cough, struggling to breathe or talk, cyanotic appearance and grasping or reaching for the throat.6 7 In addition to choking caused by a food bolus entering the trachea, causes include inhaling foreign bodies, particularly in children and aspirating vomit when consciousness is obtunded.
The abdominal thrust manoeuvre, commonly known as the ‘Heimlich manoeuvre’ is an effective technique for expelling an obstructing foreign body from the airway. As originally described by Heimlich, the rescuer places their hands around the victim’s waist, above the umbilicus and below the rib cage, from behind, and delivers a sharp inward and upward thrust to the abdomen below the rib cage.6 The UK Resuscitation Council’s basic life support guidelines, National Health Service choices8 9 and European Resuscitation Council7 state that the management of FBOA is a combination of back blows and abdominal thrusts.
We sought to understand the incidence of choking by analysing calls to the London Ambulance Service (LAS) coded as being for choking.
Methods
LAS choking data
We obtained routinely collected retrospective data from the LAS (patient report form) records for the calendar year 2016, giving the time of day, gender, age and outcome for calls identified using the search term ‘choking’. The data comprise LAS codes for ‘choking with cardiac arrest’ where a prealert or ‘blue call’ was required (ie, when the ED is contacted prior to patient arrival) and LAS codes related to ‘choking only’. Numbers of calls per estimated age band were adjusted for population numbers using data from the Office for National Statistics10 (www.ons.gov.uk). Patient outcome and data on the location from which the call had come were not available from the LAS patient report forms.
Analysis
LAS choking
In 2016, the total number of calls to the LAS requiring an ambulance response was 1 114 965. Of these, 1916 (0.2%) were coded as due to choking, an average of 5.2 per day. Forty-nine per cent were male, 50% were female and 1% unknown. Peaks in incidence for weekdays occur at lunch time from 12:00 to 14:00 and dinner time from 16:00 to 20:00. Choking occurred less frequently at breakfast time (figure 1). Notably, there was a spike in incidence on Sunday at 13:00.

Spider diagram showing choking incident count by day of week and hour of day. Vertical axis showing number of events. Circumferential axis showing time in 24 hours clock. Coloured lines relate to designated days of the week. There is a peak incidence of choking events on weekdays at 12:00 to 14:00 and 16:00 to 20:00, with a spike in incidence on Sunday at 13:00 (pink).
Eight hundred and eleven of the calls to LAS were for children aged 0–4 years (incidence of 1.3 per 1000 population) (figure 2). The incidence of choking rose steeply in older people. Although there is a known association between alcohol consumption and choking,11 only 1.3% of episodes were coded as having been related to alcohol consumption.
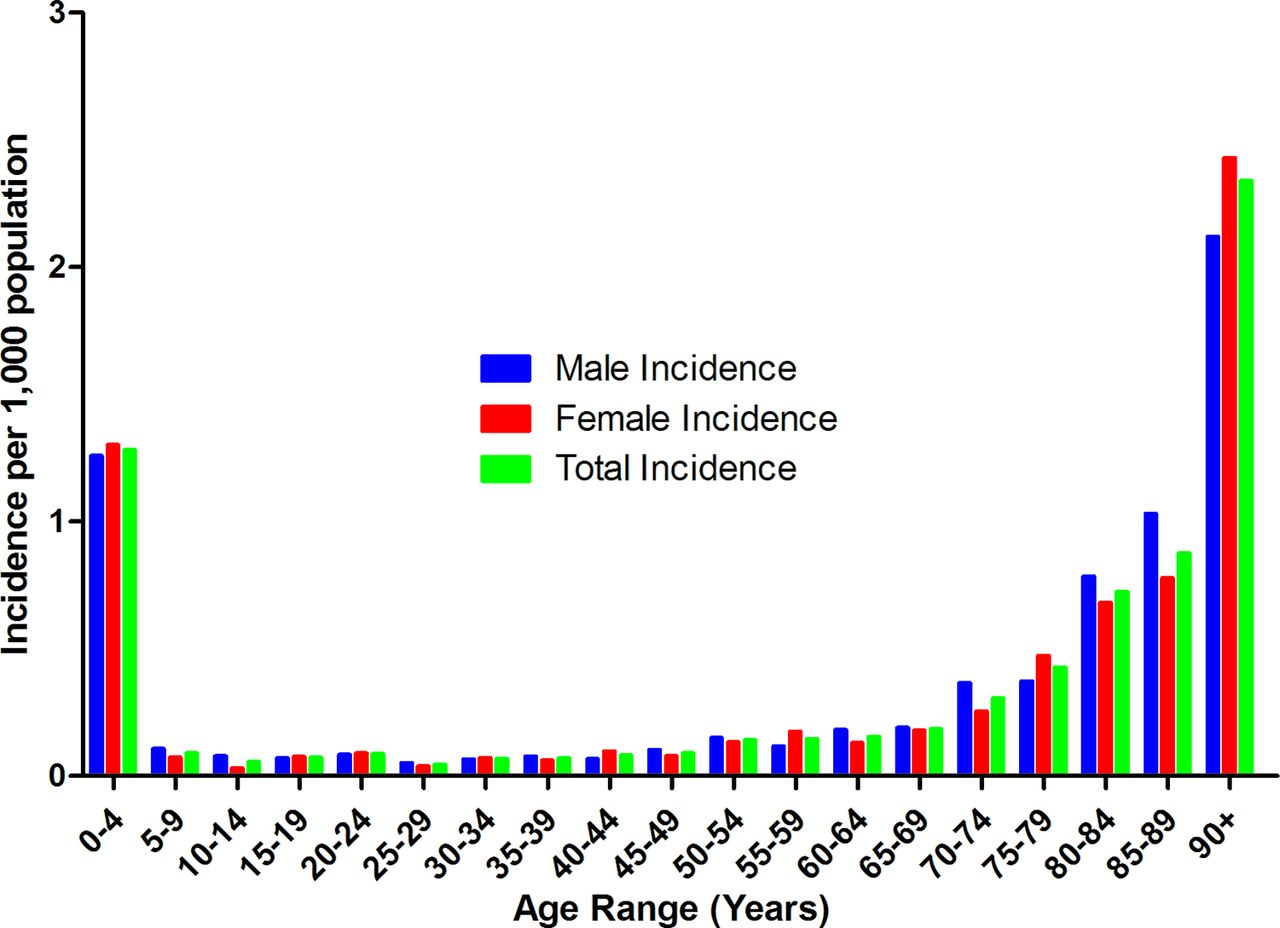
Incidence of choking in London, UK, by gender per 1000 population by age group. Incidence of choking per estimated age band adjusted for population numbers using data from the Office of National Statistics10 (www.ons.gov.uk). Total incidence of choking in the 90+ age group is higher than that of the individual genders because 35% of the total choking events for this group the gender was not documented.
Of calls to the LAS, 118 152 were coded as a prealert or ‘blue-call’; this is where a prealert call is placed to the receiving unit and urgent transfer with the ambulance using blue lights is undertaken. Of the calls coded as choking, 224 were coded as a prealert or blue call representing 0.2% of total ‘blue calls’.
One thousand three hundred and sixty-four (71.2%) LAS calls coded as choking required transfer to an ED and of these 224 (16.4%) were coded as a prealert or ‘blue call’. Thirty-two of 1364 (2.3%) of ED transfers were coded as having a cardiac arrest event related to choking with a prealert call.
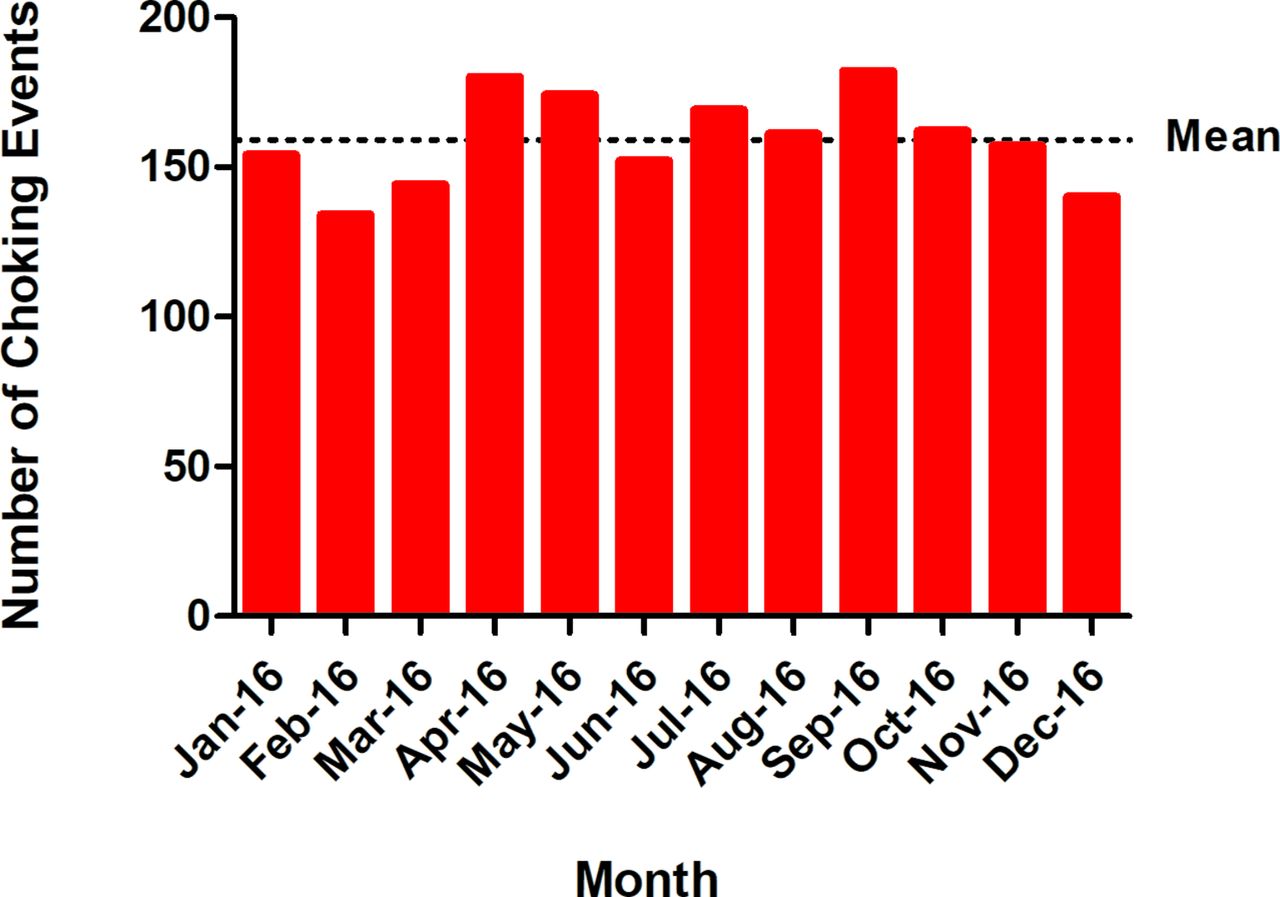
There was no apparent seasonal variation in ‘choking’ events (figure 3). The average number of choking events per month was 159.
{kind=link}
{kind=link}
{kind=link}
Number of choking events in London, UK, by month for the calendar year of January 2016–January 2017. The mean number of choking events per month was 159.
Discussion
We report data showing the incidence of choking in a large European city. The incidence was highest in the very young and very old (0–4 years and 90+ age group) (figure 2). These results are consistent with the National Safety Council, USA report4 (where 56% of choking occurred in people aged over 74 years and the data of Vilke et al’s2 study (in which 50% of hospital attendances for choking in the under 5-year-old group).
Choking is related to the consumption of food and this explains the higher incidence at mealtimes, particularly lunch and dinner, with a lower incidence during breakfast time and overnight. It may be that people are more alert at breakfast (which is often a smaller volume meal) or that lunch and dinner includes foods which the diner is more likely to choke on. The National Food Survey 1970 British Cohort study12 found that in 2016 there was a higher proportion of people eating meat-based ready meals and that meals are eaten faster at lunch and dinner. Alcohol intoxication was associated with 1.3% of calls to the LAS. However, there may well have been choking incidents where some alcohol had been consumed but not identified as a contributing factor to the choking event. There is a spike in the incidence of choking on Sundays at 13:00 which may be related to the traditional British Sunday lunch, though unexpectedly the highest single time point is 19:00 on Wednesday.
Concerns have been raised regarding the implementation of the abdominal thrust manoeuvre citing life-threatening complications including abdominal rupture,13 oesophageal rupture,3 pneumomediastinum14 and rib fracture.15 This has led to the Australian and New Zealand Resuscitation Councils recommending the use of back blows and chest thrusts in its place.16 However, in a recent physiological study, we17 assessed the effectiveness of the abdominal thrust manoeuvre to increase thoracic pressure and found that the angle at which thrusts were performed did not affect the magnitude of intrathoracic pressures achieved. It seems likely that most complications come from compressing the lower ribs and even fracturing them. We concluded that if the manoeuvre is performed on the fleshy part of the abdomen over the umbilicus with thrusts inwards rather over the upper abdomen with thrusts inwards and upwards (as traditionally recommended), then rib compression should be avoided. The risk of rib injury also seems likely to be higher with chest thrusts than with abdominal ones. Another important observation was that the self-administered Heimlich manoeuvre produced similar intrathoracic pressures to those produced by a first-aider and that the highest pressure produced in that study was by subjects compressing their own abdomen against a chair back.
Increased public awareness of the recognition and management of choking would help prevent avoidable deaths. In the state of New York, USA, the New York State Department of Health18 (www.health.ny.gov) have made available to restauranters, posters displaying the signs and management of choking. There have been a number of media campaigns highlighting choking and its management including St Johns Ambulance19 ‘the chokeable advert: save a choking baby’ and an interactive video from the Resuscitation Council, UK.20
Methodological issues
Strengths of this study are that it is based on a comprehensive dataset of all LAS calls in the calendar year 2016. However, our conclusions rely on events having been accurately coded and unfortunately no event outcome or location data were available. In addition, there must be a degree of under-reporting (the magnitude of which is unknown) since self-resolving choking events may have been managed without the requirement of LAS attendance. There may also be an under-representation due to misdiagnosis, for example, a death caused by choking being misdiagnosed as a myocardial infarction (the misdiagnosed ‘Café coronary’).11
Conclusion
Choking is a substantial health problem with 5.2 calls per day by Londoners seeking emergency assistance. Choking is more frequent in at the extremes of age and appears to have a higher incidence at lunch and dinner time.
We would recommend greater public awareness of choking and its management with signs in restaurants being a possible way to achieve this.
References
Footnotes
Contributors NSH and MG conceived the study. MJP, JN, MG and NSH wrote the survey. JN collected the LAS data. MJP and LLS analysed the results and produced the first draft of the paper. JN, MDH, MIP, MG and NHS contributed and approved the final version of the paper.
Disclaimer Dr NS Hopkinson affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.