Article Text

Abstract
Introduction Fifteen million people are affected by one or more long-term conditions in England. The cost of caring for this patient group increases every year. Several studies have been conducted to find out why people with those conditions choose to access Accident and Emergency (A&E) frequently. To our knowledge, there is no study that compares the three groups (patients, family members and hospital clinicians), and this approach may enhance understanding of A&E admissions in England. Therefore, an exploratory study was undertaken to identify key factors that contribute to A&E admissions as perceived by patients with chronic obstructive pulmonary disease (COPD) and heart failure (HF), their family members (or carers) and hospital clinicians.
Methods A mixed methods approach was undertaken: (1) semistructured interviews with patients and their family members (or carers) and (2) a self-developed survey with hospital clinicians. A purposive sample of 15 patients (9 COPD, 6 HF), 6 family members and carers (2 COPD, 4 HF) and 13 hospital clinicians (5 doctors, 8 nurses) participated in the study.
Results The patients’ main reason for A&E admission was severe exacerbation of their symptoms and all three parties (patients, family members or carers, hospital clinicians) agreed with this decision. Three key factors were highlighted in relation to A&E attendance: (1) patients’ health-seeking behaviour, (2) perceptions about general practitioner (GP) and A&E services by patients and (3) patients’ attitudes towards managing their own conditions.
Conclusions Improving patients’ perceptions of GP services in the management of exacerbations of HF and COPD will be important to increase patients’ trust in GP services so that patients will access primary care in a timely manner to prevent exacerbations of symptoms that require A&E admission. This may be achieved by developing a close collaboration between the patients, family members (carers) and hospital clinicians over time.
- chronic obstructive pulmonary disease
- heart failure
- long-term conditions
- emergency admission
- reason for admission
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- chronic obstructive pulmonary disease
- heart failure
- long-term conditions
- emergency admission
- reason for admission
Key messages
Why patients with chronic obstructive pulmonary disease (COPD) or heart failure (HF) use the Accident and Emergency (A&E) service and whether the perceived reasons are similar to or different from those of their family members or carers, and the hospital acute medical team.
This study showed that patients’ perceptions of A&E admissions are due to exacerbation of their conditions and the family members and acute healthcare professionals are in agreement.
This study was undertaken to comprehend the reasons for A&E admissions by patients with HF or COPD, their family members (or carers) and acute health professionals simultaneously, and identify influential factors contributing A&E admissions from all viewpoints.
Introduction
The National Health Service (NHS) faces continued financial hardship and the Department of Health has put significant pressure on Accident and Emergency (A&E) services to resolve some of the financial pressure.1 2 However, A&E attendance has increased by 4% since 2012.3 Although the number of A&E attendances is increasing, the Hospital Episode Statistics report 2012–2013 demonstrated that only 20.8% people who visited A&E were admitted to acute beds and 59% were discharged from A&E without needing further hospital treatment,3 suggesting that A&E attendance is not always appropriate.
Fifteen million people are affected by one or more long-term conditions (LTC) in England and the cost of caring for this patient group increases every year.4 LTCs take up 70% of the NHS social budget in England.5 People with LTCs are frequent users of A&E, especially patients with heart failure (HF) and chronic obstructive pulmonary disease (COPD).5–8 COPD is the second largest lung condition in the UK and 97% of all COPD hospital admissions are for emergency care.6 Both COPD and HF are ambulatory care sensitive conditions which hospital admission could have been prevented in the community,7 but the number of admissions of both conditions via A&E is reported to have increased for the last 10 years.8 Several studies have been conducted to find out why people with those conditions choose to access A&E frequently. The literature suggests that the decision to attend A&E is considered by patients and community healthcare professionals to be unavoidable due to overwhelming exacerbation symptoms.9–12 However, there is an evidence gap in understanding family members and hospital clinicians’ (doctors and nurses) views on A&E admissions. To our knowledge, there is no study which compares the three groups (patients, family members and hospital clinicians), and this approach may enhance understanding of A&E admissions in England. Therefore, an exploratory study was undertaken to identify key factors that contribute to A&E admissions as perceived by patients with HF or COPD, their family members (or carers) and hospital clinicians.
Methods
A mixed methods study was carried out from January to April 2014.
Participants’ recruitment and consents
A purposive sample, stratified by HF and COPD, gender and ethnicity, was used to reflect the diversity of the local A&E population. The patients were initially contacted by the ward staff on three acute admission wards and the researcher then approached interested participants to invite them for the interview and made arrangements for the interviews after written consent for their participation was received. Once the patient had agreed and provided written informed consent, the researcher directly approached the nominated family member or carer on the ward when available and obtained written consent prior to their interviews. The interview was conducted in a designated private room to avoid being influenced by their relatives (patients). The researcher requested the medical doctors and nurses who were allocated to the patients to complete a brief questionnaire to obtain their clinical viewpoints on each patient’s admission. The researcher provided an invitation letter and information sheet, and revisited the clinicians with a questionnaire and a consent form 24 hours later. The survey consisted of yes and no questions and space for free-text answers to obtain further insight into the patient’s admission (online supplementary appendix 1).
Supplementary file 1
Data generation
The data were generated through a mixed methods approach. (1) The researcher carried out separate face-to-face semistructured interviews13 14 with the patients and their family members (or carers) on the wards to obtain in detail their experiences and perceptions of A&E admission and their views on emergency healthcare services they received. Memos and reflexive diary notes were recorded after each interview.13 14 (2) A self-developed survey was included to attain the views of doctors and nurses to systematically study their perspectives of (A) the appropriateness of the A&E admission by the patients, (B) whether admission could have been avoided and (C) how future admissions could be prevented. Both interview and survey questions were piloted first with patients (1× COPD, 1× HF), family members (1× COPD) and hospital clinicians (×3) prior to the main study. The pilot data were included in the main study as no changes were made in the original interview questions and questionnaire.
Data analysis
Interviews were audio-recorded and transcribed verbatim by the researcher. Five initial transcripts were read by and discussed with the study team to ensure credibility and quality of the data and find agreement on initial coding. Thematic content analysis was conducted using NVIVO qualitative computer software V.10 (QSR International). This method was chosen because it allows direct information to be obtained from the participants and ensures that the findings are grounded in the actual data.15 The researcher adopted a conventional thematic content analysis (induction) to describe the phenomenon under study without an existing theoretical framework (deduction), and themes were derived from the textual data to gain new insight into a phenomenon.15 Recurrent codes were categorised and representative themes were linked to the identified categories. The research team discussed five randomly selected transcripts of patients and family members and compared codes and themes as a part of data validation, including a third coding phase to ensure all potential codes were explored. The questionnaire was descriptively analysed and stated suggestions by the hospital clinicians from the free-text questions were listed in a table to compare the accounts from patients and family/carer’s interview.
Results
A total of 15 patients (9 COPD, 6 HF), 6 family members and carers (2 COPD, 4 HF) and 13 hospital clinicians (5 doctors and 8 nurses) participated in the study. Table 1 shows the characteristics of the patients who participated in the interview. Demographic data for carers and hospital clinicians were not collected as this information was not deemed to be essential to answering the research questions.
The socio-demographic characteristics of the patients
Emergent themes
The duration of interviews ranged from 5 to 30 min. There were four interviews (one patient, three family members) which were 5 min long. Themes 1–3 were generated from the patients and family members’ qualitative data; the hospital clinicians’ survey resulted in descriptive quantitative data; all qualitative and quantitative data were compared across the participants to triangulate the further findings (figure 1).

Research aims and themes. A&E, Accident and Emergency; COPD, chronic obstructive pulmonary disease; GP, general practitioner.
Theme 1: reasons and circumstances for A&E admissions
All (15/15) patients reported that their reason for A&E admissions was an exacerbation of COPD or HF. The patients’ descriptions of their experience of exacerbation included emotional expressions such as ‘a shock’ and ‘I was going to die’, and the symptoms they experienced at the time were ‘frightening’ to them.
I suffered like rotten for 6 days and on a Sunday, I felt I was going to die. It was really bad. (COPD 3)
To be honest with you, I was frightened. I lost all the sense of power to fight anything, you know. That was it. (HF 3)
Although these alarming symptoms were described as unexpected by some patients (3/15), 12 patients experienced gradual progression of their symptoms within a couple of days and two patients within a day.
All the family members and carers spoke about how medically unwell the patients were at the time of the A&E admissions and their descriptions of the admission pathways were similar to those of the patients.
He had breathing problems and he suffered from COPD, which he had quite a number of years. I wanted him to come in to hospital but he didn’t want to come in, because he has been so many times before. But the breathing got so bad and in the end he asked me to come in [to the A&E]. (Family member of COPD 5)
Monday night she was up and down and got in and out of the balcony getting fresh air and all that. And then Tuesday morning she wasn’t looking any better, so she phoned the doctor up. The doctor came out [from GP surgery] in about 10 min, straight up [to the house] and examined her and phoned up the ambulance straight away. (Family member of HF 1)
Theme 2: pathways and key decision makers
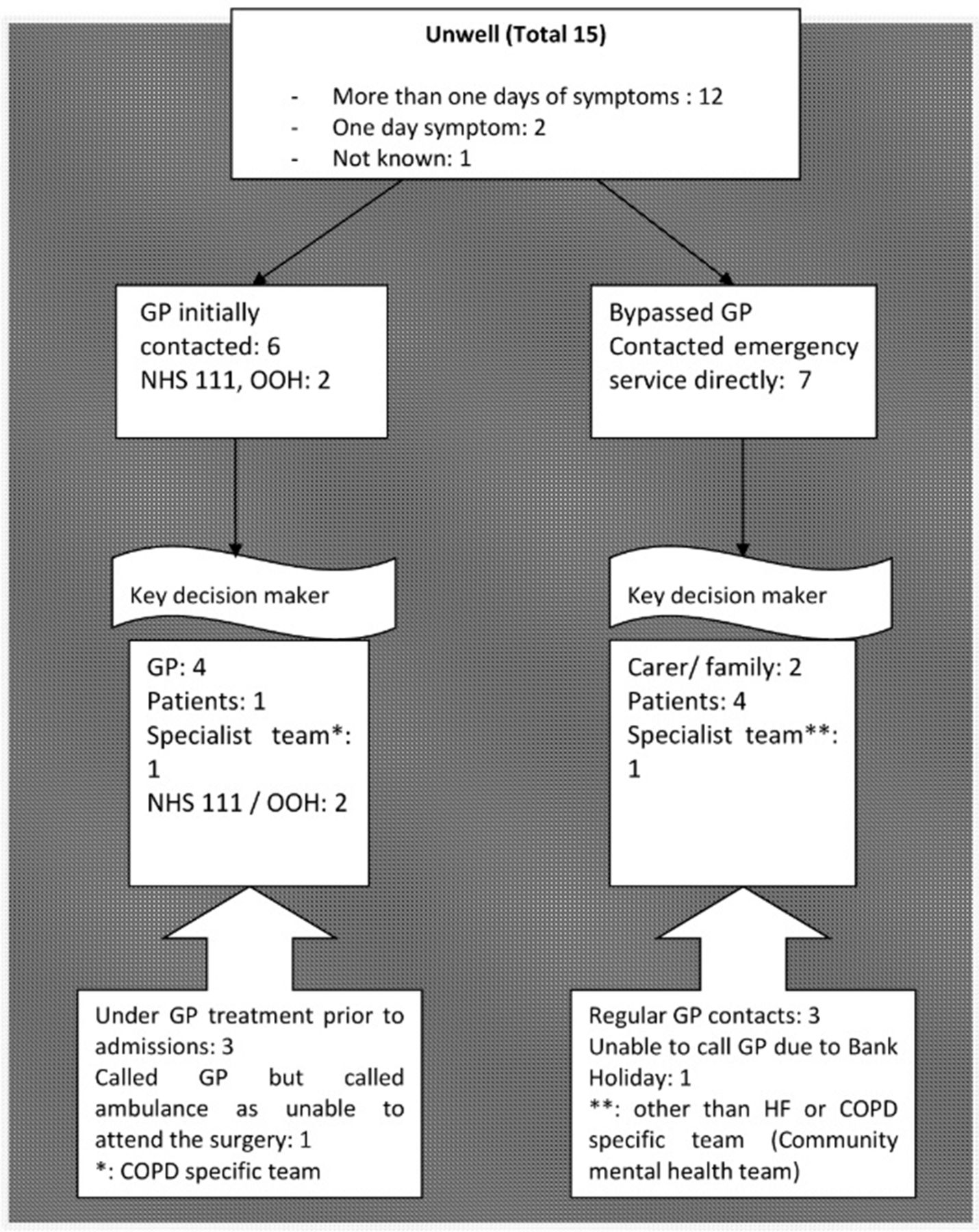
Figure 2 describes the 15 patients’ pathways to A&E and the key decision makers.

{kind=link}
{kind=link}
Patients’ pathways to Accident and Emergency (A&E). COPD, chronic obstructive pulmonary disease; GP, general practitioner; HF, heart failure; NHS, National Health Service; OOH, out-of-hours service.
When the symptoms progressed and reached a point where patients felt unable to cope, more than half of the patients (8/15) made initial contact either with their GP (5/15) or alternative GP services, for example, out-of-hours service (OOH), NHS 111 (telephone helpline) (3/15). Three out of those eight patients reported to have received treatments via their GP prior to the admission, but their exacerbation did not subside and consequently they were admitted to A&E by their GPs and/or community specialist team.
I had a chest infection, for which I had antibiotics and steroids for a week. A week after, it [chest infection] was still there, it hadn’t gone. I went back again on Friday and they [GPs] called the ambulance. (COPD 9)
The other seven (7/15) patients, who did not contact their GP, called emergency services by themselves (4/15) or by their family members (or carers) (2/15) or a healthcare professional (1/15).
Before coming today, for the last two nights I have been out of breath and couldn’t sleep, ‘cause I couldn’t lie down and I couldn’t breathe. […] This morning I just couldn’t breathe at all, so I managed to get up here [A&E by a taxi] and they [A&E staff] checked me straight in. (COPD 6)
S who is coming today, the social worker [called the ambulance]… They [community mental health team] are from the C Team, so they came [to my house for a regular visit]. I didn’t look well first. They thought I shouldn’t stay at home and I got to go to the hospital [acute hospital] so that they [acute hospital team] can see what’s wrong with me. (HF 6)
Theme 3: the perceptions of A&E versus GP services
Patients reported mixed feelings towards A&E admissions. Four patients mentioned they did not want to come to A&E and the reasons given included: (1) not wanting to disturb daily routines, (2) long waiting time in A&E, (3) hospital staff dictating them what to do and (4) uncertainty about discharge.
Another four patients, however, thought that coming to A&E was the right choice for them and their main reason was the speed of access to specialist medical assistance compared with community services. A&E was also described as having ‘the main people’, in other words, ‘experts’ in treating their LTC. This trust towards A&E service seemed to influence patients’ future decision-making, some (4/15) preferred to contact the emergency services again if similar symptoms would occur.
Oh yes, if this happens again, I will call them [emergency service] and come back up here [A&E]. I am hoping and am praying that it won’t happen again, because I have heart failure, you know… (HF 4)
In comparison to this, patients’ thoughts about their GP service were described by some (8/15) as ‘lacking in continuity’ (HF3), ‘[GP are] not too keen to visit patients [at home]’ (COPD 1), ‘no understanding of the problem [of having COPD]’ (COPD 8), ‘a drag’ (COPD 9) and ‘a waste of time’ (COPD 6).
Hospital clinicians’ perspectives on patients’ A&E admissions
A total of 13 hospital clinicians participated in the survey and provided information that related to 10 patients’ A&E admissions. Table 2 summarises the questionnaire results. All 13 hospital clinicians agreed that the patients’ admissions were due to exacerbation of HF or COPD and 11 out of 13 reported that A&E use for those patients was appropriate. Some of hospital clinicians also provided ideas to prevent future A&E admissions.
Suggestions by 13 hospital clinicians via a self-completed questionnaire
Triangulation: comparison between participant groups
The patients, family members and hospital clinicians were concordant in their view that the A&E admissions were due to exacerbation of HF or COPD. The use of A&E was regarded as appropriate by the patients and their family members (or carers), and the majority of the hospital clinicians (11/13). A difference between the parties emerged concerning how patients perceived their conditions and how all three parties considered future LTC management. Except for two patients, 13/15 patients reported that they were left to manage and cope for themselves with their LTCs.
I’ve learnt to live with it [COPD], you know. Nothing you can do about it [COPD] as such, something you caused yourself really. (COPD 8)
I’ve got it [HF] under control…I do my best to keep it controlled. (HF 1)
In contrast, the family members (5/6) and health professionals suggested future self-care management ideas such as generic and practical support. These included commencements of light exercises or change of diet, whereas hospital clinicians (7/13) recommended specific symptom management strategies or change of healthcare delivery, for example, specialist community service team input or patient education (table 2).
Discussion
Reasons for A&E admissions: participants’ views
The qualitative data of this study highlighted that the patients with COPD and HF were admitted and/or initiated admission themselves to A&E due to experiencing severe exacerbation of their symptoms. These findings support previous studies, which showed that those with LTC believed their exacerbations of symptoms were so severe and life threatening that A&E admissions were unavoidable.10 11 Family members and carers seemed to agree with this interpretation. Moreover, family members and carers either directly (eg, calling for medical expertise) or indirectly (eg, observe and monitor the patients’ symptoms) influenced the decision to seek medical help in what they decided was an emergency. In addition, most doctors and nurses also agreed that attendance at A&E was appropriate in the presented circumstances, which is in line with the findings of Drinkwater et al.12
Influences on the decision to attend A&E
Three factors emerged from the data which are important and may contribute to a reduction in emergency admission in future.
Timely seeking of medical help
The majority of patients said that their symptoms had lasted a couple of days and more than half contacted their GPs or alternative community services (NHS direct, OOH service) prior to A&E admission. These results resonated with the findings by Banger and Jones’ (2008) survey, which suggested that almost 70% of their study cohort was admitted to A&E via their GP or alternative community services.15 16 In our study, six patients were admitted via GP and three of them were actively being treated by GPs. However, most patients (12/15) experienced severe symptoms for more than a day before contacting either GPs, alternative community services or A&E, leaving the question of whether early escalated management of their symptoms could have prevented A&E admission. Patel et al11 described a ‘wait and see’ strategy adopted by patients to avoid hospital admission.11 The importance of seeking medical help in a timely manner is intensely related to what the community team (eg, GP) is able to help. Crowing and his colleagues’ study (2014) reported despite of marked increase in emergency admissions for the last 10 years in England, the number of emergency admission via GPs has decreased. Therefore, this trend highlights the gatekeeping role of GPs to contribute to the reduction of the emergency admissions.6 This role of access to specialist A&E care by GPs is achievable when the patients seek help in a timely manner.
Perceptions of GPs and A&E services
The patients who bypassed their GPs or alternative emergency services and who admitted themselves to A&E, either called emergency services, arrived via alternative transport (eg, taxi), or with family members/carers. Some of these patients reported having had regular GP contact for medical check-ups and medication review. This is an interesting finding, as with regular GP contact one would assume that early exacerbation of symptoms and signs would have been detected and a patient may use their GP to ask/request for a referral to A&E in a crisis. However, many patients reported that they regarded GPs as generalists and so, when they were acutely medically unwell, they preferred to contact A&E for specialist care. Booker et al17 examined the reasons for patients calling emergency services and they found that patients and their family members perceived the community-based services as somewhat limited.17 This is in accordance with findings from other studies9 10 and from our one study. In our study, patients reported that A&E (1) employs ‘the main people’—experts who are competent to manage their LTC, and (2) provides ‘quick access for their emergency medical situation. In comparison, GP services were perceived by some patients as a ‘waste of time’ in an emergency. Not all patients preferred to be admitted to A&E. A minority specifically stated that an A&E admission would disturb their well-established daily routines and they disliked the uncertainty of hospital discharge planning from previous experiences. However, patients’ negative perceptions of A&E admission seemed mostly to relate to the emotional distress of being away from their familiar home environment rather than questioning expert service they receive in emergency situations. Hunter et al10 argued that patients’ care-seeking behaviours are difficult to change unless they have a positive experience of community service in emergency situations. It seems therefore that patients/family members/carers’ different perceptions about different services play an important role in the decision process to attend A&E prior to contact their GPs in the event of an exacerbation of their LTC.
Attitudes towards self-management in LTCs
There were distinctive differences in how the three parties perceived LTC management. Many patients reported that their condition could be managed by carrying on ‘as usual’. This passive acceptance of how best to manage their LTC was also identified by Pinnock et al18: patients and carers accepted COPD as ‘a way of life’ and presented passive ways of seeking help for their specific long-term health needs.18 Similarly, in this study, most patients appeared to be unable to identify or articulate any additional support to manage their situation better. Instead, they seemed to yearn to return to their daily routines as soon as possible and manage their conditions independently as they had before. Additionally, passive attitudes towards their own health may also make identifying early medical help difficult.18 Family members and carers, in contrast, tended to describe a more proactive approach requesting further practical support, for example, getting a specified care package. The hospital clinicians’ feedback was mainly focused on symptom management, for example, having a community specialist team to prevent exacerbation. In a recent published document of ‘Transforming urgent and emergency care service in England NHS’,19 all patients were encouraged to take ownership of their own health and recommended to practice self-care. However, as both Pinnock et al18 and our study showed, patients may not be the expert in knowing what appropriate and effective support is available to improve their coping strategies and better self-manage their LTC. Therefore, hospital clinicians’ active involvements may be essential to support people with LTCs to manage their conditions in the community. This study also suggested that family members and carers are influential in treatment decisions, so involving them in self-management may also be an important consideration.
Strengths and limitations of study
Some of the interviews were noticeably short—5 min. Some of the interviews were short in duration due to the fact that the patient who agreed to the interview only responded with simple answers without elaborating on the subject in detail. In addition, the limited experience of the interviewer contributed to small interview length. This might have influenced the depth of the findings.
The doctors and nurses’ perceptions were obtained via a survey instead of interviews. This was a pragmatic decision due to (1) a busy hospital environment and (2) the limited time frame for the research project which was conducted as part of a master’s degree. Although the study participants were ethnically diverse, the pilot study was conducted in one geographical area, and the findings may not be representative of other areas in the UK. This project was not able to interview the patients who self-referred to A&E and discharged on the same day after a few hours receiving A&E treatment.
Conclusion and policy implications
The study findings suggest that the patients’ main reason for A&E admission was severe exacerbation of their symptoms. These interpretations were supported by the family members (or carers) and hospital clinicians. In relation to exacerbation of the symptoms, three key factors influencing A&E admission were highlighted: First, the majority of patients had suffered their exacerbation of symptoms for more than a day, prompting the question that if they had escalated the management of their symptoms earlier, could this have prevented A&E admission?
Second, there were significant differences in participants’ perceptions of GP versus A&E services in an emergency situation. Some had regular contact with their GPs but when exacerbation of their symptoms occurred, half bypassed them. A&E services were regarded as providing quick access and offering expert services to deal with their LTCs, whereas GP services were viewed as difficult to access and not competent to deal with their conditions. Improving patients’ perceptions on GP services in managing HF and COPD crises is important to increase patients’ trust in GP services so that they will be used in a more timely manner to prevent exacerbations of symptoms.
Third, some of the patients appeared to demonstrate passive attitudes towards their condition management. Patients may need to be encouraged to take ownership of their health through a close and structured collaboration over time between the patients, family members (carers) and hospital clinicians to provide and achieve optimal care for LTCs. Finally, this exploratory study suggests that there is a need for further research to investigate in GPs’ clinical reasons for patients with LTCs to admit to A&E and how patients’ perceptions of GP services could be improved. This is highly relevant in the current health climate where more than 30% of population lives with one or more of LTCs20 and there is necessity for redesigning the future service provision in primary and emergency care to meet the high demand.
Footnotes
Contributors EB, HL and VS designed the initial research idea. JSL completed the ethical approval, collected the data, carried out the data analysis, and drafted and revised the paper. EB and HL supervised the data collection and analysis and revised the paper. VS provided clinical supervision for JSL, participated in data analysis and revised the paper. All authors have seen the final version of the manuscript before submission.
Funding This research was conducted as a part of a master’s degree in Clinical Research funded by NIHR.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Research Ethics Committee approval was granted by the NRES Committee North East-Newcastle & North Tyneside 2 (REC reference: 13/NE/0364; 16 December 2013) and the local Research and Development Department (KCH 14-018; 31 January 2014).
Provenance and peer review Not commissioned; externally peer reviewed.