Article Text

Abstract
Introduction There is a continuous debate concerning the superiority of endotracheal intubation on bag-valve-mask (BVM) ventilation in patients with cardiac arrest. In this manikin-based observational study, we evaluate and compare the performance of manual ventilation through a facemask (BVM) and an endotracheal tube (ETT).
Methods One hundred and forty healthcare providers were instructed to manually ventilate a manikin as they would do for a 75 kg adult patient in respiratory arrest. Each one was ventilating both through a facemask and an ETT for a 5 min period in a random order. Ventilatory parameters were measured by the ASL 5000 lung simulator and ventilation performance was analysed using a sliding window method published in a previous study to assess accurately ventilation efficiency.
Results The mean ventilation rate was high whatever the technique used (24 bpm). A weak relationship between manual ventilation performance and the type of interface used was observed (p=0.0484). The overall rate of adequate ventilation was low even if we noticed a slight improvement when ventilating through an ETT (13.21% vs 7.5% of adequate ventilation). However, the rate of hyperventilation did not differ between mask and tube (79% vs 77%). A significant relationship is observed between professional category, the size of the hand squeezing the bag and manual ventilation performance (p<0.05).
Conclusion Whatever the interface used, healthcare professionals are still struggling to perform manual ventilation efficiently according to international guidelines. Ventilation with an ETT does not prove to be significantly more efficient than with a facemask. It would be therefore important to recentre the debate on controlling ventilatory parameters with current devices. Focusing on training may maximise manual ventilation efficiency and minimise the loss of time during cardiopulmonary resuscitation.
- non-invasive ventilation
- equipment evaluations
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Whatever the interface used, healthcare professionals are still struggling to perform manual ventilation efficiently according to international guidelines.
It would be therefore important to re-centre the debate on controlling ventilatory parameters with current devices and on training.
Introduction
Manual ventilation with facemask or endotracheal tube (ETT) interface (also called bag-valve ventilation) is frequently needed in many prehospital and in-hospital sceneries (during induction of general anaesthesia, after intubation while mechanical ventilation is being prepared, or when mechanical ventilation fails to achieve better patient oxygenation).1–3 However, these basic and advanced airway management procedures (bag-valve-mask (BVM) with a facemask or endotracheal intubation (ETI) with an ETT) may have adverse events that can disturb patient haemodynamics and consequently impair survival.4 5
BVM is the most common method of ventilation used by emergency medical technicians. The challenge of this technique is to maintain patent airways and reduce leaks.6 7 Several research studies have shown that healthcare professionals have trouble in ventilating adequately patients in accordance with international guidelines. This irregular and inadequate ventilation leads to either excessive airway pressure, gastric insufflation, and subsequent regurgitation and pulmonary aspiration or to hypercapnia and hypoxaemia.4 6–12
In opposition, ETI requires advanced skills in airway management and is only practised by experienced and highly trained healthcare professionals (mainly emergency physicians or anaesthetists).5 6 13 However, this procedure might require time to perform and potentially lead to harmful events such as oesophageal and bronchial trauma, but also can sometimes be prolonged and delay the oxygenation of the patient or even completely fail.14 15 Furthermore, it is important to minimise chest compression interruption during cardiopulmonary resuscitation in order to increase survival with good neurological performances.16 Thereby, while it is considered the ‘gold standard technique’ for advanced airway management, international guidelines recommend the use of laryngeal mask airway or BVM as alternatives for adults.13
There is a continuous debate regarding the superiority of ETI on BVM and their ability to provide adequate oxygenation to patients.17 Indeed it remains important to know that, even if ETI is correctly performed, the main challenges of manual ventilation are to keep adequate and constant tidal volume and ventilation rate to prevent hyperinflation or hypoventilation. Therefore, we designed this prospective randomised bench study to compare the performance of manual ventilation with ETT and facemask, and assess the variability of the provided ventilation.
Materials and methods
Study design
In this study, we used the same protocol on BVM ventilation that we published in 201518 to compare the performance of BVM and ETI manual ventilation. This protocol was submitted for ethical approval but it was waived by the local ethics committee (CPP Est II). This manikin-based observational study was conducted in the Department of Emergency Medicine and Critical Care of Besançon. Briefly, 140 healthcare professionals, trained in basic life support during their initial training, were enrolled. They were still in service, aged over 18 years and coming from different independent structures (University Hospital of Besançon, Doubs Fire Department and Jussieu Ambulance Services). They were instructed to ventilate a manikin with two adult bag valves (Ambu and Laerdal bags) selected randomly in sealed envelopes, as they would do for a 75 kg adult patient in respiratory arrest. However, they were blinded regarding their ventilation performance transcribed on a computer. Ventilation was performed in protected airways with an ETT (8.0 mm ID). The size and the grip strength of the hand squeezing the bag were determined by using a tape measure and a Takei dynamometer, respectively. We define the level of professional experience based on their seniority at the moment of the trial enrolment. Thus, data of operator characteristics (professional category, grip strength of the hand keeping the bag and hand size) and ventilatory parameters (tidal volume (VT), ventilation frequency (VR), inspiratory and expiratory times (Itime and Etime)) were collected.
The manikin, a Laerdal Airway Management Trainer (Laerdal Medical, Stavanger, Norway), was connected to an ASL 5000 lung simulator (IngMar Medical, Pittsburgh, PA, USA) which simulated an apnoeic patient with a compliance of 70 mL/cmH2O and an airway resistance of 3.5 cmH2O/L/s. Ventilatory parameters (tidal volume, ventilation frequency, inspiratory and expiratory times) were measured by the lung simulator using the ASL SW V.3.3.106 software.
The manual ventilation performance was assessed using a new analysis method developed and published recently.18 The algorithm of this method evaluates the performance of a 1 min window depending on tidal volume (VT) and ventilation rate (VR). It consists of segmenting every ventilation test into sliding windows of 1 min length each with a shift of three ventilation cycles each time. This will enable us to consider intraindividual, interindividual and time variability of ventilatory parameters. Regarding our simulated patient model (75 kg ideal body weight (IBW) with no respiratory pathology), we considered tidal volume from 300 to 600 mL and a ventilation rate between 8 and 15 bpm to be adequate. Thus, three situations were distinguished to assess the performance of a sliding window according to tidal volume (VT) and ventilation rate (VR) measurements during the 1 min period:
Hyperventilation: VR >15 bpm and/or mean VT >600 mL.
Adequate ventilation: VR ≤15 bpm, mean VT ≤600 mL with at least eight adequate ventilation cycles (with a VT between 300 and 600 mL).
Hypoventilation: VR ≤15 bpm, mean VT ≤600 mL and the number of adequate ventilation cycles <8.
Data analysis
Continuous data are expressed as mean±SD and as percentages for nominal variables. The comparison between professional categories and hand size and the different performance levels was done using a Χ2test or Fisher exact test. OR, estimated by logistic regression, was used to analyse performance level for the multivariate model. A p<0.05 was considered statistically significant and SAS V.9.3 (SAS Institute) was used for statistical analysis and randomisation.
Results
Five hundred and sixty ventilation tests (280 for ventilation using appropriate facemask provided with each type of bag18 and 280 for ventilation through an ETT) were performed by 140 healthcare professionals (45 physicians, 45 nurses and 50 rescuers) with a mean age of 37 (9) years. Among them, 45% (63/140) had a high level of professional experience and one-third were women. This study population is presented in table 1.
Characteristics of study population (n=140)
Results show that the mean ventilation rate was high (24 bpm) and similar when healthcare professionals ventilated through a facemask or an ETT. The mean tidal volume obtained with the ETT interface was greater than that obtained during manual ventilation with the facemask interface (462 vs 334 mL for ETT and facemask interfaces, respectively) (table 2).
Ventilation parameter values measured during all the 5 min ventilation tests (n=280 tests for each ventilation technique)
The ventilation performance of healthcare professionals was also analysed and results show that manual ventilation performance was slightly influenced by the type of interface used (p=0.0484). The overall rate of adequate ventilation was low even if we noticed a minimal improvement when ventilating through an ETT (13.21% vs 7.5% adequate ventilation tests). The rate of hyperventilation did not differ (79% vs 77%) (table 3).
Ventilation performance analysis during the 5 min ventilation tests (n=280 tests for each ventilation technique)
We also evaluated some operator characteristics that may have an impact on ventilation performance. Multivariate analysis shows that manual ventilation performance was only impacted by the professional category (p=0.0002 and p=0.0286 for ETT and facemask ventilations, respectively). The size of the hand squeezing the bag had a significant impact only on ETT ventilation performance (p=0.0175 and p=0.5982 for ETT and facemask, respectively). The other factors like grip strength, bag type (Ambu or Laerdal bag) and professional experience had no effect on ventilation performance (p>0.05).
Figure 1 depicts more in detail the ventilation performance of the different professional categories and shows that physicians and nurses were more efficient than first-aid workers when ventilation was performed with an ETT (20%, 13% and 7%, respectively). This difference disappears when ventilation was performed with a facemask (9%, 6.67% and 7%, respectively, for physicians, nurses and first-aid workers). We observed also that all healthcare professionals hyperventilated whatever the interface used (>70%).

Percentage of hyperventilation (black), adequate ventilation (grey) and hypoventilation (light grey) for professional categories (n=280 tests for each ventilation technique). ETT, endotracheal tube.
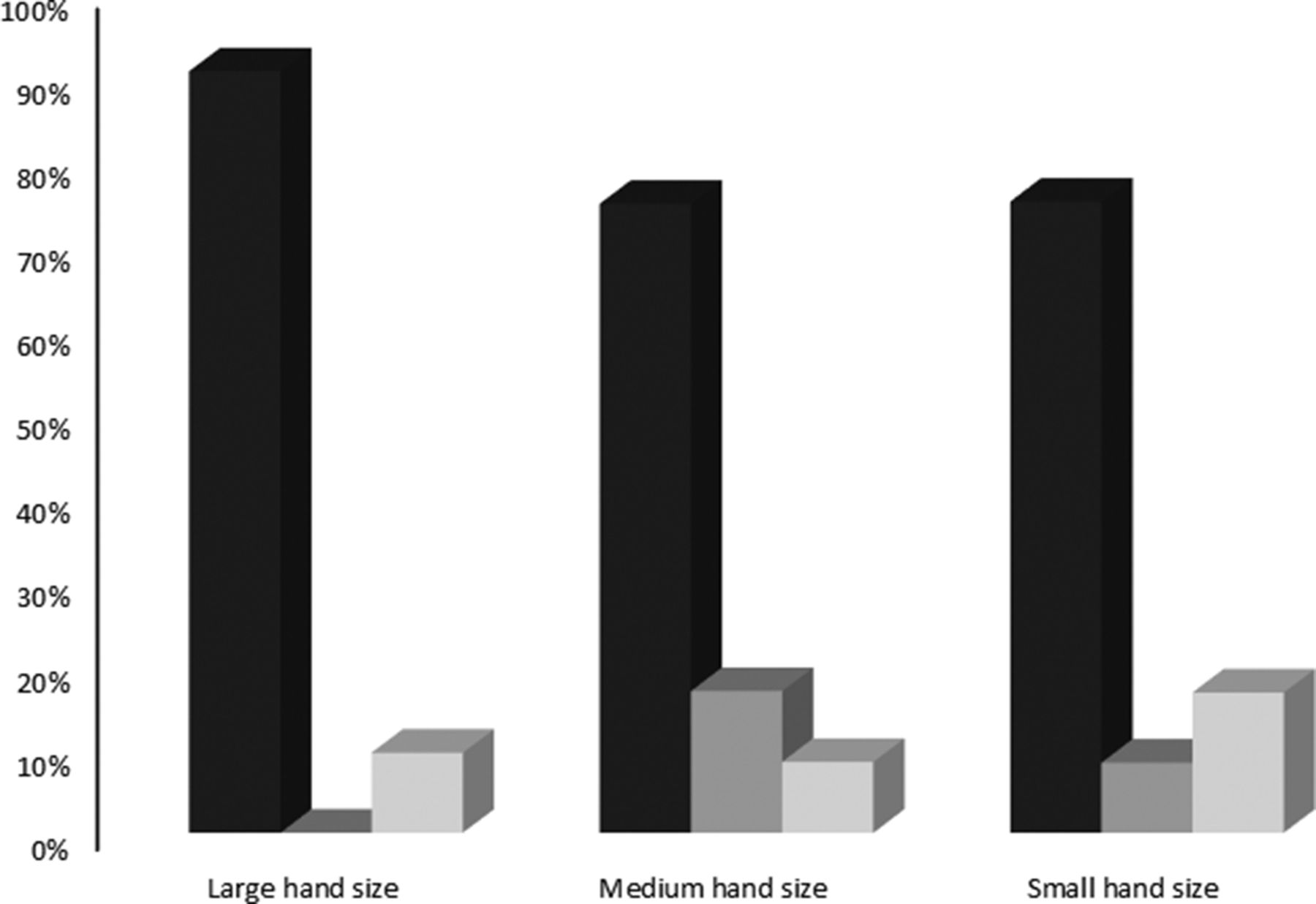
The impact of the hand size on ventilation performance is presented in figure 2. It shows that the larger the hand squeezing the bag was, the more excessive the ventilation was (90% vs 75% for large and medium hand size, respectively). When the hand was small, there were more hypoventilation tests compared with medium hand size results (16.67% vs 8.42%).
{kind=link}
{kind=link}
Percentage of hyperventilation (black), adequate ventilation (grey) and hypoventilation (light grey) for hand size categories of the hand squeezing the bag (n=280 tests with an endotracheal tube (ETT)). Large hand size (≥23 cm), medium hand size (19≤n<23 cm) and small hand size (15≤n< 19 cm).
The intraindividual and interindividual variability of the two ventilation interface techniques is also analysed. There was not any intraindividual variability between facemask and ETT ventilations concerning ventilation rate (p>0.05) while the variability of tidal volume was doubled with facemask compared with ETT ventilation (p<0.01). However, a statistically significant difference was observed for the interindividual variability of tidal volumes between ETT and facemask interfaces (154 vs 132 mL, p=0.00001) with a maximum mean tidal volume of 877 and 1004 mL and a minimum mean tidal volume of 47 and 142 mL, respectively, for facemask and ETT ventilation tests.
Discussion
Ventilation is important for patient survival in cardiac arrest and/or respiratory distress. It is usually performed manually through a facemask or an ETT. These two ventilation techniques, mostly used by healthcare professionals in hospital and prehospital settings, have some problematic aspects.
ETI is considered to be the ‘gold standard’ because it maintains airway patency and avoids leaks, but we were interested to know whether, after the intubation, healthcare professionals ventilated adequately the patient in accordance with international guidelines. Indeed, inadequate ventilation is associated with impaired haemodynamics and increases morbidity and mortality. So we have evaluated and compared the performance of these two techniques and the factors involved, and the intraindividual and interindividual variability of the provided ventilation.
Healthcare professionals have performed 560 ventilation tests with an ETT (280) and a facemask (280). Among them, only 58 (10.4%) were adequate ventilation tests while the remaining 502 (89.6%) were inadequate ventilation tests (438 (78.2%) hyperventilation tests and 64 (11.4%) hypoventilation tests). This inadequate ventilation could increase the morbidity and the mortality of patients. Indeed, hyperventilation decreases the PaCO2, leading to central nervous system vasoconstriction, lower cerebral blood flow and secondary neurologic tissue injury, and can create free radicals and irreversible cellular damage.19–21 Furthermore, the mean ventilation frequency was twice more than the adequate ventilation rate recommended by international guidelines.22 23 It was shown that hyperventilation is mostly caused by high ventilation rates rather than excessive volumes.24 However, we observed a slight improvement in ventilation performance with the ETT than with the facemask (13% vs 7.5%), which was due to a reduction of hypoventilation sequences. This could be explained by the lack of leaks during ventilation with an ETT, leaks that remain difficult to control during ventilation with a facemask. Nonetheless, this rate of adequate ventilation stayed very low and proves that healthcare professionals are still struggling to perform manual ventilation efficiently and are hyperventilating in over 75% of cases whatever the interface used (79.3% vs 77.1%, respectively, for facemask and ETT ventilation tests).
In order to understand which factors may impact manual ventilation performance, we studied operator characteristics and showed that only the professional category and the size of the hand squeezing the bag affect manual ventilation performance. First-aid workers seem to have more difficulties to ventilate adequately in protected airway with 7% of adequate ventilation tests while 20% of physicians and 13% of nurses provided adequate ventilation. These results could be explained by the fact that first-aid workers, first on scene before advanced paramedics, are more accustomed to ventilate patients in unprotected airway. In these conditions, leaks could attenuate excessive ventilation volume provided to the patient. However, we observed that they also hyperventilated either with a facemask or with an ETT. This suggests that they tend to ventilate with an ETT as they use to do with a facemask (93% of inadequate ventilation tests for each technique). Only experienced and highly trained healthcare professionals such as advanced paramedics, physicians and nurses are authorised to secure the patient airways with an ETT and they are used to ventilate intubated patients, hence the high rate of efficient ventilation compared with first-aid workers (20% vs 7% and 13% vs 7% for physicians and nurses, respectively, vs first-aid workers). Conversely, physicians and nurses who performed efficient ventilation with ETT hypoventilated the lung with facemask interface. These results underline that it would be necessary for healthcare professionals to adapt the appropriate approach to ventilate the patient when they use a facemask or an ETT interface and to take into account presence or absence of leaks.
Concerning the size of the hand squeezing the bag, it only has an influence when using an ETT. We observed that the participants with larger hand size (>23 cm) have major tendency to hyperventilate the patient, with 0% of adequate ventilation tests observed. When the hand size was medium (between 19 and 23 cm), there was a reduction of approximately 16% of hyperventilation. However, when the hand size is small, that is, under 19 cm, the percentage of hypoventilation increased by 8%. It might be helpful to raise awareness of healthcare professionals regarding the influence of these factors to adapt ventilation practices in order to optimise the ventilation efficiency (eg, healthcare professionals with large hands should squeeze the bag gently to avoid excessive ventilation). This may also explain why the interindividual variability between participants was so important. Indeed, we recorded mean tidal volumes varying from 47 to 877 mL with facemask and from 142 to 1004 mL with ETT. The same heterogeneous performances were observed on ventilation frequencies with mean VR ranging from 8 to 53 bpm and from 8 to 48 bpm with facemask and ETT interfaces, respectively.
Although the debate continues in favour of tracheal intubation to secure the airway and maintain patency despite a lack of clear evidence,16 25 intubating the patient may lead to several complications both at the time, during and after intubation, and even result in loss of effectiveness of resuscitation.26–28 A study of Hanif et al has shown that this technique was associated with decreased survival to hospital discharge of adult non-traumatic patients compared with ventilation with a facemask.29 So, if ventilation with an ETT does not prove to be significantly more efficient than with a facemask, as we showed in this study, it would be important to refocus the debate on controlling ventilatory parameters and developing high-performance medical tools that can maximise ventilation efficiency and minimise the loss of time during cardiopulmonary resuscitation. Indeed, immediate and early cardiopulmonary resuscitation with a short interruption of chest compressions is vital to increase patient survival. These medical tools can be real-time feedback devices that would instantly indicate to the healthcare professionals what they actually do during manual ventilation.
This study presents some limits as it is a manikin study and we still cannot confirm that the ventilation performance described herein is a reliable representation of what could be obtained in clinical trials. In real clinical situations, especially in intubated patients, measuring ETCO2 by capnography can help the healthcare professional to better ventilate. However, most of studies dealing with ventilation performance in the literature are manikin-based studies.30 Leaks in manikin ventilation (BVM) are more common than in real use on patients. Only few masks work effectively with a manikin, and are usually not supplied with the bags. But leaks induce users to ventilate faster hoping to ensure adequate ventilation. In addition, we decided to evaluate ventilation performance and not the difficulty related to intubation technique. This latter issue has been well documented in the literature and therefore was not considered in this study. Thus, the manikin was intubated before the 280 ventilation tests were performed. Furthermore, we still cannot confirm that the BVM ventilation performance described in this study and obtained with a new analysis method is a reliable representation of what could be obtained in clinical trials and in other centres.
In summary, the high failure rate of manual ventilation observed in this study shows that ‘to intubate or not to intubate the patient’ is not really the question, especially when its benefits are still being debated. ETI is certainly considered the ‘gold standard technique’ but unfortunately, ventilation is still poorly performed afterwards inducing other complications in addition to those associated with intubation. New devices as the Fastrach or laryngeal mask may be good alternative to increase the rate of adequate ventilation. We think we should focus more on how to improve manual ventilation efficiency with current devices and minimise these complications. We should also consider how to teach healthcare professionals to adapt their ventilation practices according to the airway management technique used.
Acknowledgments
We thank all the staff of the Departments of Emergency Medicine and of Anaesthesia and Critical Care of Besançon University Hospital, the staff of the Doubs Fire Department and Besançon Jussieu Ambulances teams who voluntarily participated in this research project and made it possible.
References
Footnotes
Contributors FSS carried out the bibliography, drafted the protocol and the manuscript. ADL defined the new analysis method and realised bench tests. AP performed the statistical analysis and drafted the statistical section. LP participated in the conception and design of the study. GC guided the work and corrected the manuscript. AK supervised the work and corrected the manuscript. All authors approved the final manuscript.
Funding This work is supported by an unrestricted grant from the European Commission (FEDER) in Franche-Comté, Bpi France, the Greater Besançon Urban Area Community (CAGB), the Regional Council of Franche-Comté and the General Council of Doubs Department.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.