Article Text

Abstract
Introduction Widespread white matter damage and cognitive impairment have been demonstrated in chronic obstructive pulmonary disease (COPD). However, it remains unclear if brain atrophy is a global phenomenon or if specific subregions are differentially affected. The aims of this study are, first, to test a simple, validated visual analogue grading technique. Second, we hypothesised that frontal regions of the brains of patients with COPD will show greater signs of atrophy compared with control subjects. Third, any localised regions of atrophy would correlate with components of cognitive performance. Finally, the severity of cerebral atrophy would be associated with measures of respiratory disease severity.
Methods We used a simple, validated visual analogue grading technique to assess the degree of regional atrophy in multiple brain regions from cerebral MR images in patients with stable non-hypoxaemic COPD (n=25) and age-matched control subjects (n=25). We also explored correlations between regional brain atrophy with demographics, cognitive performance measures and disease severity. Measures of cognitive performance focused on executive function, working memory, verbal memory, overall memory and processing speed. Measures of disease severity include lung function, gas exchange, health status and breathlessness questionnaires.
Results The visual grading scale found that patients with COPD had significantly greater frontal atrophy than control subjects (p=0.02), independent of smoking history, comorbid depression or anxiety. Cognitive function was significantly worse in the COPD group for executive function (p<0.001), working memory (p=0.02), verbal memory (p=0.03) and processing speed (p=0.001). Group differences in atrophy did not appear to account for differences in cognitive function. We were unable to identify meaningful correlations between regional atrophy and disease severity or cognitive function.
Conclusion Further work is needed to identify causative mechanisms behind unexplained structural brain changes in COPD.
- COPD pathology
- COPD ÀÜ mechanisms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Significant brain pathology and cognitive impairment has been consistently demonstrated patients with chronic obstructive pulmonary disease (COPD), but it is not clear how best to detect and measure these brain changes. Current MR analysis requires complex data processing and expertise to interpret
A simple, easy to learn visual rating scale may be able to detect significant brain pathology in COPD.
We used a simple, validated visual analogue grading technique to assess the degree of regional atrophy in multiple brain regions from cerebral MR images in patients with COPD. It was simple to learn and repeatable and shows patients with COPD had significantly greater frontal atrophy than control subjects.
Introduction
It is well established that patients with chronic obstructive pulmonary disease (COPD) have multiple comorbidities, such as heart disease, stroke, skeletal muscle wasting and depression.1 2 These systemic effects are not explained by shared risk factors alone, such as cigarette smoking, hypertension of hypoxaemia, leading to the hypothesis of a ‘COPD-specific’ risk for comorbidity.3 The presence of comorbidities in COPD is associated with significantly worse patient outcomes such as increased hospitalisations, impaired functional capacity, decreased quality of life and mortality.3 Therefore, characterising and understanding these comorbidities is essential to optimising the management of each individual patient.
Previous studies have shown that up to 77% of patients with hypoxaemia with COPD have cognitive impairment indicative of cerebral dysfunction.4 This has also been demonstrated in non-hypoxaemic patients with COPD.5 There is also evidence that cognitive impairment in COPD is associated with reduced ability to carry out basic and instrumental activities of daily living6 7 and poor medication adherence.8 Combined, these factors are likely to contribute to increased exacerbations and hospital admissions, decreased quality of life, increased length of hospital stay9 and, possibly, increased mortality.10 The identification of COPD as a risk factor for accelerated cognitive dysfunction11 presents clinicians and researchers with a potential target for interventions to prevent or delay cognitive impairment.
People with COPD have been found to perform poorly across a wide spectrum of cognitive areas. The most frequent and severely affected cognitive domains appear to be those related to executive function, attention and memory.5 Motor function and processing speed are also likely to be negatively impacted on by COPD.12 We may therefore expect specific regions of the brain, thought to be functionally linked to these cognitive domains, to be at risk of damage in patients with COPD, for example, executive function and frontal lobes.
Previous analysis of global microstructural changes in this population of stable, non-hypoxaemic COPD MR diffusion tensor imaging showed extensive reduction in white matter integrity, but no difference in the overall volume of grey or white matter, suggesting generalised cerebral atrophy, was unlikely.13 Two small studies in patients with hypoxaemia with COPD found evidence of frontal lobe hypoperfusion with the authors concluding that anterior cerebral hypoperfusion could herald frontal-type cognitive decline with the worsening of the hypoxaemia.14 15 Hippocampal atrophy has also been identified in COPD16 in addition to localised grey matter (GM) loss.17 18 However, these studies are limited, as they require complex data processing and statistical techniques, which do not always adequately adjust for multiple comparisons.
In this study, we test a simple, validated visual MRI rating scale to analyse multiple brain regions of stable, non-hypoxaemic patients with COPD and age-matched control subjects. We aimed to identify areas of regional brain atrophy, we sought associations between regional brain atrophy and cognitive function before looking at whether any patient characteristics could account for particular regions of atrophy.
There is ongoing debate concerning the neuronal pathways and supplementary cortical and subcortical brain regions involved in cognitive functioning. We used associations more widely accepted to form our hypotheses. The relationship between executive function and the frontal lobe19 and that between memory and the hippocampus20 are examples. We aimed to test a simple, validated visual analogue grading technique in this study. We hypothesised that, first, the frontal regions of the brains of patients with COPD will show greater signs of atrophy compared with control subjects. Second, any localised regions of atrophy would correlate with components of cognitive performance. Finally, the severity of cerebral atrophy would be associated with measures of respiratory disease severity.
Methods
Subjects
This study was carried out as analysis of data collected from a prospective case–control study, titled ‘Brain structure and function in chronic obstructive pulmonary disease—a multimodal cranial magnetic resonance imaging study’.13 Twenty-five patients with stable, non-hypoxaemic COPD (n=25) were recruited from outpatient respiratory clinics of two university teaching hospitals (St George’s Hospital and Royal Brompton Hospital) between 2010 and 2011. Patients were non-hypoxaemic (PaO2>7.3 kPa)21 and had no exacerbations in the preceding 8 weeks. Recruitment of an age-matched control group (n=25) from the local community took place through local press advertisements. All subjects were required to have at least primary school education or equivalent and be competent in English in order to complete neuropsychological testing. Control subjects with significant respiratory or cognitive difficulties were excluded. Exclusion criteria were otherwise the same for both groups and included other causes of cognitive impairment (overt psychiatric illnesses, drugs known to cause sedation or cognitive impairment, diagnosis of dementia, current or past alcohol or drug abuse), breathlessness attributed to heart disease or left ventricular dysfunction, neurologic disease, active tumours, vascular complications of diabetes, diagnosis of obstructive sleep apnoea, visual and hearing disturbances and hepatic failure.
Image acquisition
Whole-brain T1-weighted MRI was performed on all patients and controls using a Philips 3T Achieva dual TX scanner (with a 32-channel head coil).
Image analysis
Technique
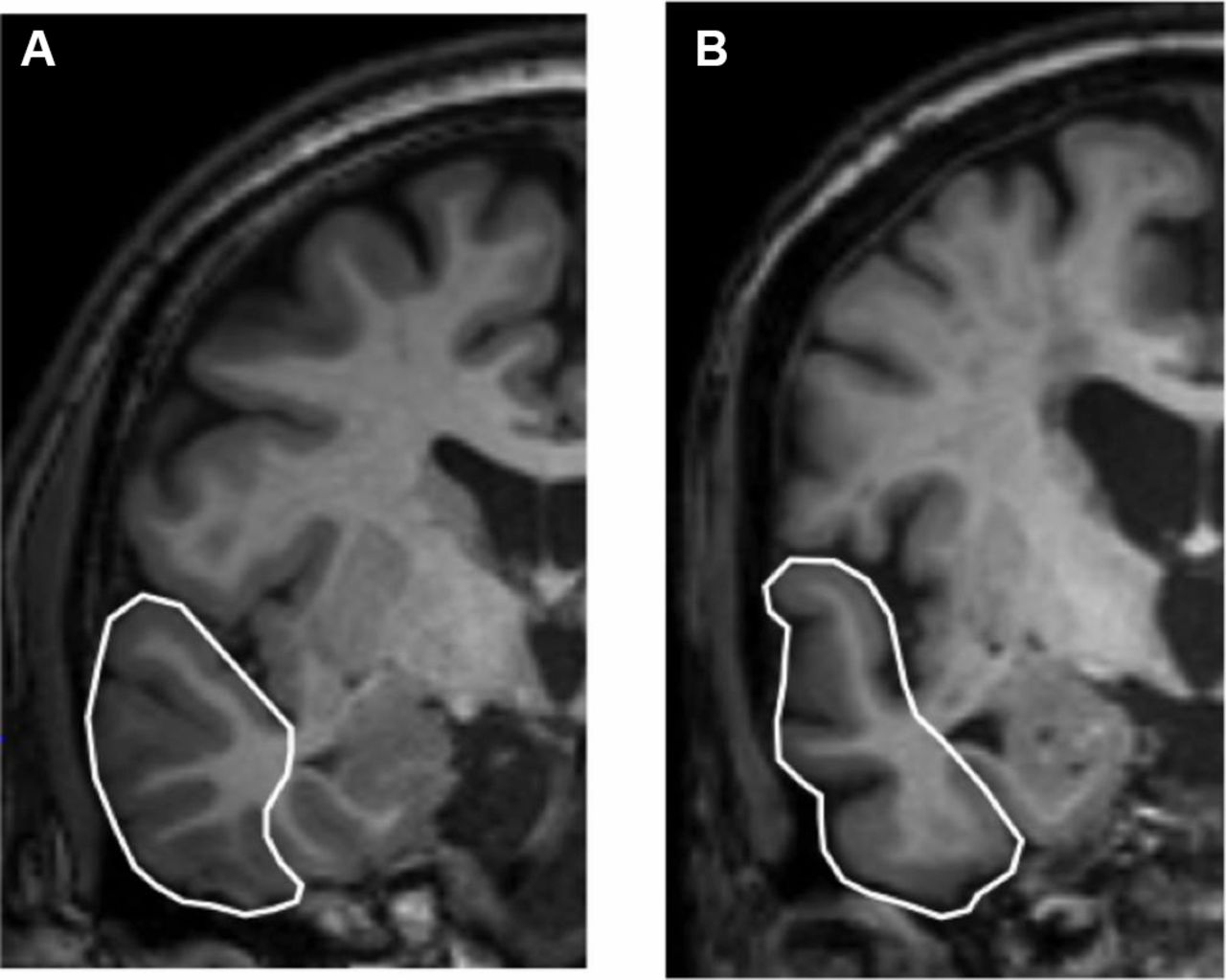
The T1-weighted MRI images were analysed in the coronal plane by a rater blinded to the clinical condition of each subject. A validated visual analogue MRI grading technique was used to assess the degree of atrophy in multiple brain regions.22 Fifteen brain regions were rated bilaterally using a 5-point Likert-type scale: 0=no atrophy; 1=borderline appearances, not necessarily abnormal; 2=definitive signs of atrophy; 3=severe atrophy, with preservation of structure to a degree; 4=very severe atrophy, GM not discernible in cortical structures. Each structure was located within one of four slices, chosen using defined landmarks (from anterior to posterior), namely: slice 1=at the level where the internal capsule can first be seen; slice 2=at the level of the intralimbic gyrus’ medial opening; slice 3=at the level of the lateral geniculate nucleus; slice 4=the level where the fornix can be seen in continuity beside the pulvinar nucleus. In slice 1, the anterior temporal lobe, basal ganglia, orbitofrontal cortex, dorsolateral frontal cortex and anterior cingulate were rated; in slice 2, the anterior hippocampus, entorhinal cortex, perirhinal cortex, anterior fusiform gyrus, lateral temporal lobe and insula; in slice 3, the mid-hippocampus and superior temporal gyrus; in slice 4, the posterior hippocampus and Brodmann area 37. Figures 1 and 2 demonstrate rating examples in slice 1 and slice 2 for different subject brains.

Slice 1 in the right hemispheres of two different subject brains. The white line highlights the dorsalfrontal lobe. This region would be rated as 0 for brain A (not atrophic) and 2 for brain B (signs of atrophy).
{kind=link}
{kind=link}
Slice 2 in the left hemispheres of two different subject brains. The white line highlights the lateral temporal lobe. This region would be rated as 0 for brain A (not atrophic) and 2 for brain B (signs of atrophy).
Rater training
The rater (CCS) was trained using a subset of the MRI scans collected for this study, alongside images provided in the original paper describing the technique. The same scan set was independently rated by an experienced rater (CP). An iterative training process was used initially, followed by rerating of 10 scans to give a measure of intrarater reliability (measured using Cohen’s kappa coefficient).
Health assessments
All participants’ demographic and medical histories were collected through interview and medical records. Age, gender, educational level (based on General Certificate of Secondary Education, A level, diploma, degree or other levels of qualification) and pack-years were recorded. The following areas were also explored:
Comorbidity: Charlson Comorbidity Index (CCI).23
Cerebrovascular risk: modified Framingham’s Stroke Risk Profile (FSRP) (ECG-defined left ventricular hypertrophy omitted).24
Mood: the Hospital Anxiety and Depression (HAD) questionnaire.25
With regard to the above three scoring methods, the higher the number obtained, the worse outcome predicted.
Additionally, the following were captured for the COPD group only, to define functionality and disease severity:
Forced expiratory volume in 1 s (FEV1).
Forced vital capacity.
PaO2 and PaCO2 using arterialised earlobe capillary blood gases (COPD subjects only).
St George’s Respiratory Questionnaire (SGRQ)—a 50-item questionnaire. A score of 100 indicates the worst possible health status and 0 indicates the best possible health status.
Medical Research Council Dyspnoea Scale was used to measure patients’ perceived respiratory disability, based on their degree of breathlessness.
Neuropsychological tests
In addition to the Mini-Mental State Examination (MMSE) cognitive screening tool,26 a comprehensive neuropsychological battery was used. Executive function was tested using verbal fluency and trail making from the Delis-Kaplan system27; working memory using letter-number sequencing and spatial span from Wechsler Adult Intelligence Scale28; visual memory using Rey Complex29 Figure-Immediate (3 min) and Delayed Recall (30 min) and Recognition; verbal memory using Word Lists-List Learning, Word Lists Delayed Recall (30 min) and recognition from Wechsler Memory Scale,30 and processing speed using the digit symbol and symbol search from Wechsler Adult Intelligence Scale. Testing was carried out in a quiet room to ensure data collection uniformity and in a fixed sequence to avoid responses to self-complete questionnaires being influenced by subsequent tests. Age-standardised scores were then calculated with reference to normative population samples.
Age-standardised cognitive scores were generated with reference to normative population samples.27–30 These scores are in the range (mean±SD) of 1–20 (10±3) for all measures. A score ≤7 indicates mild cognitive impairment.31
Statistical analysis plan
Data were analysed using IBM SPSS version 23. Histograms were plotted for each variable to visually check for normality of distribution. Data for demographic characteristics, baseline cognitive function and regional atrophy were assessed for group differences using an independent samples t-test, if normally distributed, or Pearson’s χ2 test, if non-normally distributed. Differences were deemed significant at p<0.05. Group differences in regional atrophy were also analysed after controlling for CCI, pack-years and HAD scores, using a generalised linear model multivariate analysis. A bivariate correlation was performed in the whole group (COPD and controls) and COPD group to test for associations between regional atrophy and cognitive function (Pearson’s correlation coefficient for normally distributed data and Spearman’s rank-order correlation for non-normally distributed data). As an exploratory analysis, associations between disease severity and regional atrophy were also assessed in this way.
Results
Demographics
Demographic characteristics for the control and COPD groups are displayed in table 1. The groups were well matched on age, sex, FSRP and MMSE score. As anticipated, COPD subjects had a significantly greater number of pack-years (4.16 vs 58.33), they were also significantly more anxious, depressed and with lower levels of education and a greater number of comorbidities than controls.
Demographic characteristics and cognitive function of the control group and COPD group
Visual rating assessment
Agreement analyses.
Inter-rater
The weighted kappa coefficient at the start of the training process was 0.66 (p<0.001), demonstrating significant agreement between the two raters and comparing well to the overall inter-rater kappa value of 0.71 (p<0.05) reported in the paper in which this scale was developed.22
Intrarater
From the ten rerated scans, 300 values were obtained. Raw percentage agreement was 77.7% and Cohen’s kappa coefficient was 0.66 (p<0.001). Again, this compares well to the reported intrarater kappa coefficient of 0.75 (p<0.05) from the original rating scale paper, indicating good intrarater agreement.
Regional atrophy
Table 2 shows the bilaterally summed composite scores for regional atrophy in the two groups. Grouping the scores from anatomically and functionally related regions formed the composite scores, as demonstrated in table 3. Left and right hemisphere scores were summed to give overall bilateral scores and the mean of this value was generated. As per a priori hypothesis, frontal regions of the patients with COPD were more atrophic than those of the control group (p=0.01). This difference in frontal atrophy remained significant after controlling for CCI, pack-years and HAD scores. There was, however, no difference in temporal or hippocampal atrophy between the two groups. After statistical correction, hippocampal atrophy did not meet significance.
Bilaterally summed composite scores for regional atrophy in the control and COPD groups (presented as mean±SD)
Regions included in composite groups
Cognitive function
Neuropsychological test scores significantly worse in the COPD group compared with controls for executive function (p<0.001), working memory (p=0.02), processing speed (p<0.001) and verbal memory (p=0.03), but mean scores for both groups were not in the clinically impaired range (table 1). There was no significant difference in visual memory (p=0.22) between the two groups. Overall difference in memory function (average of visual, verbal and working memory performance) did not reach statistical significance (p=0.05).
See online supplementary materials for further description of neuropsychological measures (online supplementary table 1 and online supplementary figures 1–5)
Supplemental material
Disease severity within the COPD group
Measures of disease severity for the patients with COPD (table 4) demonstrated no significant hypoxaemia or hypercapnia. The mean age was 67.8 years and 41% were female. Health status was moderately impaired (SGRQ 51.65). Airway obstruction (FEV1) was moderate (52.51% of predicted value).
Clinical, functional and symptomatic measures of the COPD group
Correlations between regional atrophy and cognitive function
Scores for regional atrophy did not significantly correlate with cognitive function in the COPD group. There was a large amount of scatter around the regression line when the association between frontal atrophy and executive function was plotted for the COPD and control groups. On exploration of the whole group (COPD group and control group together) associations between verbal memory and atrophy within the temporal (r=0.30, p=0.03) and hippocampal (r=−0.33, p=0.02) regions were found. However, after correction for multiple comparisons using Bonferroni method (p=0.002), these associations were not significant.
Disease severity and regional atrophy
No correlations between regional atrophy in the COPD group and selected measures of disease severity within this group (PaO2, FEV1 % predicted and SGRQ) were found.
Discussion
This study set out to use a simple visual MR rating scale22 in the assessment of regional cerebral atrophy in patients with COPD and age-matched control subjects. The visual rating scale was simple to learn and repeatable between raters. It demonstrated significant atrophy in the frontal regions of non-hypoxaemic patients with COPD with moderate airflow obstruction and health status impairment (p=0.01). There was no difference between the two groups in the degree of hippocampal or temporal atrophy. This population of patients with COPD had worse average cognitive function than controls but no significant correlations were found between regional atrophy and cognitive function or measures of disease severity.
The significant frontal atrophy demonstrated by visual rating in these data confirms findings from smaller single-photon emission computerised tomography (SPECT) cerebral perfusion studies in patients with hypoxaemic COPD suggesting frontal hypoperfusion.14 15 The frontal atrophy demonstrated in this study is consistent with the frontal-type cognitive decline thought to occur in patients with COPD.9
In contrast to previous studies that have demonstrated reduced hippocampal volume in patients with COPD,16 no significant hippocampal atrophy was found in this study. Our findings are also not concordant with recent evidence for a correlation between hippocampal volume and hypoxaemia.16
Limitations of this study may, in part, account for the lack of significant association between regional atrophy, cognitive function and disease measures. It is possible that the relatively small participant sample size hindered our ability to form important potential correlations. However the sample size is similar to other imaging studies designed to identify meaningful differences in brain pathology in a well-characterised population sample such as in this study. Age and education are known to predict cognition, while the COPD and controls were matched for age in this study, differences in educational attainment between COPD and control groups were controlled for statistically. This approach was adopted given the pragmatic considerations required to prospectively recruit education matched control subjects.
In addition, results obtained from analysing MRI scans without using volumetric measurement can only provide an estimate for the difference in atrophy between these two groups. Clear descriptions are provided in the paper in which the technique used in this study was devised.22 However, there is still the potential for misratings as a consequence of structural variation between brains and subjectivity of raters. Moreover, the scale suggested for use with this technique is relatively narrow, probably because it was originally developed for assessing different forms of neurodegeneration. This narrow scale makes it more difficult to distinguish subtle structural changes, which are more likely to be found in patients with COPD.
This study confirms that using a simple visual rating scale is effective for investigating atrophy in the brains of patients with COPD, advocating its use in future studies. The validated technique used in this study was chosen as it was inexpensive and specialist equipment was not required. The findings of this study have implications for our understanding of structural damage in the brains of patients with COPD, supporting a possible frontal atrophy and executive pattern cognitive impairment. Like many of the studies of brain pathology and cognitive function in COPD, consistent associations between demographic and disease severity are seldom identified. There are a number of possible explanations for this. First, the principle of ‘cognitive reserve’—the recognition that cross-sectional studies are unable to capture cognitive decline over time, in particular those of premorbidly ‘high-normal’ cognition who remain cognitively intact at time of assessment but who nevertheless may have undergone significant cognitive decline. Second, our traditional measures of disease severity have historically focused on lung physiology such as FEV1. It is now appreciated that they do not reflect the multisystem nature of COPD and are not thought to be directly involved in the pathophysiology of comorbidity in COPD. Systemic inflammation, accelerated ageing, autonomic dysfunction and genetic susceptibility have all been considered as possible mechanisms of increased comorbidity such as cognitive impairment and warrant further investigation.32
This was a preliminary study that warrants replicating in a larger sample using patients with a wider range in severity of COPD. Doing so will improve our understanding of to what extent hypoxaemia plays a role in regional atrophy and also increase the likelihood of identifying relationships between regions of atrophy and cognitive dysfunction.
Conclusions
It is possible to use simple visual rating scale to assess regional atrophy in COPD. This technique shows evidence of frontal cerebral atrophy in patients with stable, non-hypoxaemic COPD independent of comorbidity, smoking and mood. These morphological changes may contribute to the cognitive impairment displayed in this population; however, this study did not find significant correlations between the degree of brain atrophy and cognitive functioning or disease severity. Further investigations with a larger sample size are needed to explore these important potential associations. At this stage, the mechanism behind regional atrophy in the brains of patients with COPD is unclear.
References
Footnotes
Contributors JWD and CP conceived the presented idea. JWD provided data set from previous published research for the further analysis of this study. CCS performed image analysis and generation of results with CP. PHAD provided critical feedback and all authors contributed to shaping of the research. CCS wrote the manuscript with supervision from JWD, CP and PHAD.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Wandsworth and East Central London Research Ethics Committees.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.