Article Text

Abstract
Background Fever is considered as a presenting symptom of pulmonary embolism (PE). We aim to evaluate the association between PE and fever, its clinical characteristics, outcomes and role in prognosis.
Methods A retrospective chart review of patients who were hospitalised with the diagnosis of acute PE was conducted. Patients in whom underlying fever could also be attributable to an underlying infection were also excluded.
Results A total of 241 patients met the study criteria. 63 patients (25.7%) had fever within 1 week of diagnosis of PE of which four patients had fever that could be due to underlying infection and were excluded. Patients in PE with fever group were younger compared with PE without fever group (52.52 vs 58.68, p=0.012) and had higher incidence of smoking (44.1% vs 20.9%, p<0.001). Patients in PE with fever group were more likely to require intensive care admission (69.5% vs 35.7%, p<0.001), had a longer hospital length of stay (19.80 vs 12.20, p<0.001) and higher requirement of mechanical ventilation (30.5% vs 6.6%, p<0.001) compared with those without fever. PE with fever group were more likely to have massive and submassive PE (55.9% vs 36.8%, p=0.015) and had higher incidence of deep vein thrombosis (33.3% vs 17.4%, p=0.0347) compared with PE without fever. In a univariate model, there was higher likelihood of in-hospital mortality in PE with fever group compared with PE without fever (22.0% vs 10.4%, p=0.039).
Conclusion Patients with acute PE and fever have higher morbidity and clot burden.
- pulmonary embolism
- fever
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Significance of fever in patients with acute pulmonary embolism.
Fever may signify higher clot burden and poor outcomes.
How we came to this conclusion and what is the current evidence.
Introduction
Pulmonary embolism (PE) is among the leading causes of hospital-associated complications, preventable hospital deaths and healthcare costs.1 Attributable death rate in these patients ranges up to 10%–30% (if untreated) and 8% (if treated) in hospitalised population with economic burden exceeding 1.5 billion dollars in USA.2 3 According to the regional experience in several US studies, PE has an incidence of approximately 71–117 per 100 000 person-years4 with prevalence as high as 2%.5 In a community-based study by radiologists using CT angiogram, PE was diagnosed in 13% of hospitalised patients (132/981).6 To evaluate the dynamics of this menace of death, several studies have been performed and reported various aspects of diagnostic, therapeutic and prognostic strategies but data remain limited regarding the symptomatic accuracy of the disease.7 8 Although cough, pleuritic chest pain and dyspnoea have been mentioned as the most common symptoms of PE, fever has been considered a surrogate symptom and sought with interest as a cause of physician’s apprehension, unnecessary use of antibiotics and diagnostic evaluation.9
Roughly half of all patients with PE and deep vein thrombosis (DVT) are noted to have fever ranging from 38°C to 38.5°C.10 ,11 In the landmark PIOPED study,12 fever (temperature at or above 37.8°C) was observed in 14% patients with no identifiable cause. Similarly, PISAPED study13 demonstrated fever above 38°C in 6 out of 440 patients with PE. Murray et al noted temperature of ≥38°C (≥100.4°F) in 64% and 6% with temperature of ≥39.5°C (≥103.1°F) in patients with PE.14 Israel and Goldstein indicated low-grade fever in 78.9% of patients despite the use of antibiotics.15 On contrary, in a prediction model for the probability of PE proposed by Miniati et al, fever was not considered a major predictor of PE, but the study did not receive appropriate external validity.16 Later, in a study by Kokturk et al, 33% patients with PE developed fever, of which 12% (5/39) subjects had temperature over 39°C.17
Despite all efforts exercised to identify role of fever as a diagnostic predictor of PE, less is known about its prognostic role and importance in management algorithm.18 We intend to identify the association between PE and fever, clinical characteristics of patients with PE presenting with fever and its prognostic implications, if any.
Methods and material
Study design
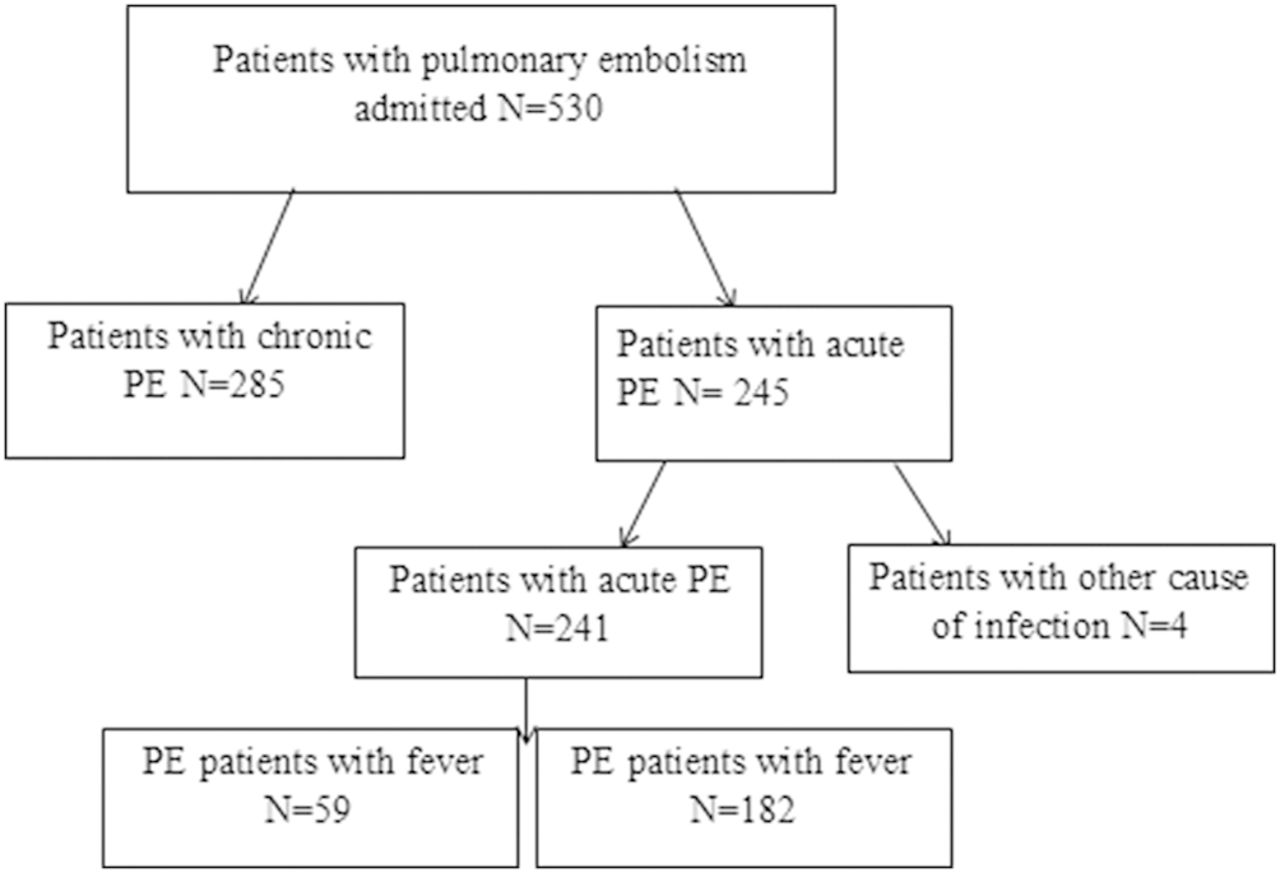
A retrospective chart review of patients with newly diagnosed acute PE admitted from 1 January 2008 to 31 January 2018 to BronxCare Health System was conducted. A total of 530 patients were identified, of which 285 histories of previously diagnosed acute PE were excluded. A total of 245 patients had acute PE diagnosed during the hospital stay of which 63 patients (25.7%) had fever within 1 week of diagnosis of PE. Of these 63 patients, 4 had fever that may have been due to an underlying infection and therefore were excluded. A total of 241 patients were included in final analysis (figure 1). We classified our patients into two groups, namely PE with fever and PE without fever. We collected data regarding patient’s baseline demographics, comorbid conditions, vital signs, laboratory parameters and severity of PE. Cultures and radiographic data within 1 week of fever were also collected to assess for infection as underlying source of fever. We further gathered data regarding use of anticoagulation, antibiotics and tissue plasminogen activator. Primary outcome in our study was mortality difference between the two groups. Secondary outcomes were severity of PE, length of stay (LOS) in hospital, need for intensive care unit (ICU) admission, need for mechanical ventilation.

{kind=link}
Schematic picture of study design. PE, pulmonary embolism.
Study was approved by the institutional review board (IRB#01111803).
Definitions
Following definitions were used in our study:
Fever was defined as temperature of ≥100.4°F within 1 week of diagnosis of PE. All cultures and radiographic data were reviewed and patients with evidence of an active infection or those in whom an underlying infection could not be excluded with certainty were removed from the final analysis. We excluded four such patients of which two died during the hospital stay. Furthermore, there were four patients with positive cultures who were included in the study as those cultures were deemed colonisers.
Massive PE was defined as PE with sustained hypotension (systolic blood pressure <90 mm Hg).12
Submassive PE was defined patients with systolic blood pressure >90 mm Hg but evidence of right ventricular dysfunction on echocardiograms or on the CT pulmonary angiograms or evidence of myocardial damage as reflected by increase in cardiac biomarkers.12 14
Statistical analysis
Demographic information and clinical outcomes were stratified by fever status. Means and SD were reported for continuous variables. Frequencies and percentages were reported for categorical variables. ANOVA tests were used to assess the association between continuous variables and fever status. χ² tests were used to assess the association between categorical variables and fever status. For the relationship between ventilation usage and mortality, subgroup analyses were conducted by antibiotic usage status. Frequencies and percentages were reported. χ² tests were used to assess the association between the outcome variables and fever status. Separate multivariable logistic regressions were used to assess the association between fever status and if the patient is expired or not, need for mechanical ventilation, need for ICU admission, controlling age, pulmonary infarction, heart rate, systolic blood pressure, leucocyte count, congestive heart failure (CHF), smoking history and if the patient had simple or submassive and massive PE. Multivariable linear regression was used to assess the association between fever status and LOS controlling age, pulmonary infarction, heart rate, systolic blood pressure, leucocyte count, CHF, smoking history and if the patient had simple or submassive and massive PE.
Results
Table 1 indicates demographic and clinical information stratified by fever status. There were 241 patients in the study. Patients in PE with fever group were younger compared with those without fever (52.52 vs 58.68, p=0.012), had higher heart rate (101.14, vs 90.20, p<0.001), had lower mean systolic blood pressure (115.93 vs 123.72, p=0.013) and higher mean leucocyte count (10.98 vs 9.80, p=0.006). Among patients with fever, the percentage of antibiotic users were higher than the percentage of non-antibiotic users (62.7% vs 26.9%, p<0.001). During evaluation of underlying comorbid conditions, we found that patients with fever and PE compared with those without fever had higher incidence of smoking (44.1% vs 20.9%, p<0.001) and lower incidence of CHF (1.7% vs 12.6%, p=0.029).
Demographic and clinical variables
Table 2 indicates the outcomes stratified by fever status. The percentage of patients who died, need for mechanical ventilation and ICU admission were higher for patients with fever compared with patients without fever (mortality: 22.0% vs 10.4%, p=0.039; need for mechanical ventilation: 30.5% vs 6.6%, p<0.001; ICU admission: 69.5% vs 35.7%, p<0.001). The LOS was higher for patients with fever compared with patients without fever (19.80 vs 12.20, p<0.001).
Outcome data
Table 3 indicates results from regression analyses. After controlling confounders, the OR for requiring mechanical ventilation was 4.6 (CI 1.71 to 12.88). The OR of needing ICU was 5.74 (CI 2.73 to 12.57). Having fever was associated with 6.62 (CI 2.11 to 11.14) days longer LOS in the hospital.
Multivariable logistic regression results
Discussion
In this 10-year single-centre study of all hospitalised patients with newly diagnosed acute PE, we showed that presence of fever was associated with higher likelihood of underlying massive and submassive and DVT. The need for mechanical ventilation, hospital LOS and ICU admission was also higher in patients with acute PE and fever. Patients with acute PE and fever also had a higher mortality in a univariate analysis. To the extent of our knowledge, our study is probably the first to extensively study this clinical and prognostic correlation of PE and fever while accounting for underlying infections.
Fever has been reported as one of the key symptoms of PE along with cough, chest pain and dyspnoea with majority of the data emphasising its association with low grade fever.12 18 Presence of high-grade fever in the setting of thromboembolism is not supported by evidence and identification of another source has been suggested.18 In the recent data, low-grade fever in PE is detected in the range of 6%–33% and high-grade fever is reported variably from 3% to 14%.12–14 In our study, 24.5% population manifested fever with average peak temperature observed was 38.6°C (101.5°F) within 1 week of PE diagnosis. Comparably in a study by Murray et al, 18 out of 19 subjects with PE were afebrile after 1 week of diagnosis.14 The most common accompanying symptom, besides fever, manifested in our PE population was chest pain and shortness of breath which is a similar finding observed by Korkturk et al in a study of 39 patients with PE and fever.17 Identical description of symptoms including dyspnoea and restlessness was reported by Hodgosn et al in patients with PE and pulmonary infarction secondary to large or recurrent small emboli causing obstruction of pulmonary circulation.19
Fever that persisted beyond 1 week of initiation of anticoagulation was not attributed to PE itself and thus other causes should be evaluated.18 19 Several aetiologies have been proposed for persistent fever after 1 week of PE diagnosis including pulmonary infarct, superimposed infection, drug fever and Dressler like phenomenon.20–22 Stein et al 20 noted fever in 39 out of 267 patients with pulmonary infarction and haemorrhage and found more evidence of DVT in patients with PE and otherwise unexplained fever which was also observed in our study. Further, several patterns of PE-related fever were described based on duration including intermittent, sustained or hectic type,20–22 though intermittent and sustained type were noted more in our study group. In one of the studies on complicated PE,21 fever was observed in 26% of heparin and urokinase-treated patients (41 out of 158). In our study, we identified that fever was more likely in patients with massive and submassive PE compared with those with simple PE (55.9% vs 36.8%) and we did not find any statistical difference in terms of pulmonary infarcts between the two groups.
The pathophysiology of fever in PE has not been clearly understood.19 23 24 Several models for its mechanism have been mentioned in literature but none is supported by the evidence.25–27 The pyrogenic model described the production of inflammation cascade associated with tissue necrosis, vascular irritation and atelectasis that leads to rise in body temperature.15 16 This results in an elevated leucocyte count in the early part of disease course which was also observed in our study.17 Another mechanism explained by Jerjes and his colleagues22 is Dressler-like syndrome, caused by immune reactivity of serosa (pleura and pericardium) secondary to vascular remodelling, reported in 4% of patients with PE. This mechanism can result in pleural effusion, fever, anaemia and leucocytosis. Our study highlighted a noteworthy association of fever and higher incidence of massive/submassive PE and DVT in patients with acute PE.
In majority of the studies performed to identify the relationship of PE and fever, exclusion of other causes of fever was not well illustrated and thus its association with PE remained debatable.25–27 Our study is noteworthy in a way that we included microbiological data and clinical decision making to identify individuals in whom fever could be attributed to PE with more certainty and excluded those where we could not establish this relation with certainty. The antibiotic use was higher in patients with PE and fever. The common reasons recognised in the literature for initiation of antibiotics in patients with PE are leucocytosis, infiltrates on X-ray imaging or clinical symptoms that may suggest underlying pneumonia which are probably also true for our study cohort.17–19
The data regarding outcome of individuals with PE and fever are very limited. 25 26 28–33 Our study is striking in this regard that we investigated the morbidity and mortality data for this subset of population. Watanakunakorn25 reported that nearly half of the patients with PE with high-grade fever in his study died. This study was a series of seven patients with limited microbiological data evaluation. Additionally, outcome and patient characteristics were not well elaborated. Calvo-Romero et al 26 reported in hospital mortality of 7% in patients with PE and fever. Although the study included majority of the patients with PE diagnosed by various imaging modalities; however, it is limited by the fact that investigators favoured pneumonia as the cause of fever and had not considered other sources of infection into account. Furthermore, outcome data in this study including morbidity and mortality were similar in all groups. In a 4-year prospective study on predictive factors of PE, Bahloul et al 33 studied outcome data in patients with PE irrespective of occurrence of fever in patients who were critically ill. They reported mean length of hospital stay (LOS) of 25 days, mean ICU stay of 20.2 days and the in-hospital mortality rate of 52.9%. Even though the study included clinical characteristics, risk factors and outcomes in acute patients with PE, the authors did not signify association of fever in such patients and its clinical impact on patient outcomes. In our study, mean LOS for PE and fever was 14 days, with higher likelihood of ICU admission in fever group (69.5% vs 24.7%). We also found higher mortality in patients with PE and fever (22% vs 10.4%) along with higher need for mechanical ventilation (30% vs 6.6%).
There are several limitations of our study. First, we used a retrospective design where we were limited to the information obtained by the medical records and not direct patient contact. Second, we included patients from a single centre, which cares for an inner-city population with specific demographic characteristics. Third, our study group is relatively small compared with some large PE study which can affect study power. However, we believe that even with small patient population, our study was able to answer some interesting clinical questions. Fourth, we retrospectively reviewed all septic workup data in patients admitted with acute PE and fever and excluded all those patients with underlying infections. This could introduce selection bias. To address that bias, two study investigators (MS and MA) independently reviewed the patient charts and excluded patients where underlying cause of fever may be attributed to non-PE source. Fifth, we did not include any patients who had fever more than 1 week from diagnosis of PE. This was done in view of prior data that stated that fever beyond 1 week is less likely to be associated with PE.11 12 14 16 Sixth, since it is a 10-year study, advancement in medical practice might be a confounding factor which may have affected the study results. Finally, we did not include ICU severity scoring system (APACHE or SOFA scores) to estimate its contribution to mortality and LOS. Despite the limitations, our study highlights the potential association of fever with clot burden in acute PE that has both clinical and prognostic implications in care of these patients.
Conclusion
Fever in patients with acute PE is associated with distinct clinical and prognostic parameters. Patients with acute PE and fever are more likely to have massive or submassive PE and DVT. Presence of fever was also associated with higher need mechanical ventilation, ICU admission and longer hospital LOS. Larger prospective studies are needed to validate our findings.
References
Footnotes
Contributors MS, MA and AZ wrote the first draft of the manuscript and reviewed the data for its integrity. DHS, AA, NM, MS and MA did the data collection. AZ performed the statistical analysis for the study. All authors reviewed, edited and approved the final draft of this manuscript. MA is guarantor of this paper and take full responsibility for the integrity of the work as a whole, from inception to publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval BronxCare Hospital Center, IRB#01111803.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data available upon request