Article Text

Abstract
Introduction Patients with progressive idiopathic fibrotic interstitial lung disease (ILD), such as those with idiopathic pulmonary fibrosis (IPF), can have an aggressive disease course, with a median survival of only 3–5 years from diagnosis. The palliative care needs of these patients are often unmet. There are calls for new models of care, whereby the patient’s usual respiratory clinician remains central to the integration of palliative care principles and practices into their patient’s management, but the optimal model of service delivery has yet to be determined.
Methods We developed a novel, collaborative, multidisciplinary team (MDT) meeting between our palliative care, psychology and ILD teams with the principal aim of integrating specialist care to ensure the needs of persons with ILD, and their caregivers were identified and met by referral to the appropriate service. The objective of this study was to assess the effectiveness of this novel MDT meeting on the assessment of a patient’s palliative care needs.
Results Significant increases in advance care planning discussions were observed, in conjunction with increased referrals to community courses and teams, following introduction of this novel MDT.
Conclusions Our results suggest that our collaborative MDT is an effective platform to address patients’ unmet palliative care needs. Further work is required to explore the effect of our model on achieving the preferred place of death and reductions in unplanned hospital admissions.
- palliative care
- interstitial fibrosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Key messages
What is the best model of care to enable integration of specialist palliative care into management of patients with interstitial lung disease (ILD) to ensure the needs of patients and caregivers are met?
We describe a novel collaborative multidisciplinary team discussion platform, integrating psychology and specialist palliative care with respiratory and primary care, that effectively identifies the palliative care needs of our patients with ILD.
It is hoped that this initial work will form the basis of further study exploring the impact of this model on improving meaningful patient outcomes, such as achieving the preferred place of death and reducing unplanned hospital admissions.
Introduction
The interstitial lung diseases (ILD) are a group of heterogeneous lung diseases. A subset of patients with progressive idiopathic fibrotic ILD (PF-ILD), such as those with idiopathic pulmonary fibrosis (IPF), can have an aggressive disease course, with a median survival of only 3–5 years from diagnosis,1 a prognosis that is comparable with some forms of lung cancer.2
There are calls for new models of care, whereby the patient’s usual respiratory clinician remains central to the integration of palliative care principles and practices into their patient’s management,3 with early evidence suggesting that this approach may improve end-of-life care and unscheduled healthcare use.4 While the optimal model of service delivery has yet to be determined,5 it is an important priority given the increasing prevalence of this disease globally.6 7
We previously identified that patients were signposted late to specialist palliative care services within our service.8 Using quality improvement methodology, we developed and introduced a supportive care decision aid tool (SCDAT) that led to significant increases in early referral for specialist palliative care and documented discussions surrounding advance care planning (ACP).
Here we describe a novel, collaborative, multidisciplinary team (MDT) meeting between palliative care, psychology and ILD teams, which was subsequently developed to provide a platform for discussion, integrating specialist palliative care with respiratory and primary care, to ensure the care needs of patients (and caregivers) are identified and met by referral to the appropriate service.
The objective of this study was to assess the effectiveness of this novel MDT meeting on the assessment of a patient’s palliative care needs.
Methods
Description of the palliative–psychology–ILD MDT
The principal team members of the palliative–psychology–ILD MDT include a palliative care consultant and nurse, a psychologist, an ILD consultant, nurse and pharmacist, and an MDT coordinator. Hosted once every 6 weeks, its aims are to assess and provide physical (identifying symptoms needing optimisation), social (self-help, carer, rehabilitation) and psychological support to patients with ILD and their caregivers. Importantly it enables integration of secondary care and primary care services, seeking continued community support.
Any patient deemed to require further input as determined by the SCDAT can be referred by any healthcare professional to this MDT. Each case is presented with focus on key areas required by all represented disciplines, alongside electronic database documentation. An electronic report is generated and distributed to the relevant healthcare professionals, including community physicians and healthcare teams; if further input is required, dedicated palliative care and psychology consultations are organised.
Study methodology
The records of all patients discussed in the MDT meeting between January 2016 and July 2016 (post-MDT cohort) (n=46) were retrospectively analysed, alongside a comparison cohort of patients with ILD who had died 8 months prior to the introduction of the MDT meeting (pre-MDT cohort) (n=26).
Baseline patient characteristics were retrospectively recorded, including demographics (age, gender), ILD subtype, use of oxygen therapy and/or the suggestion of pulmonary hypertension/right heart strain, defined for the purposes of this study by indicative echocardiographic findings (with estimated pulmonary arterial systolic pressure >40 mm Hg or evidence of right heart dysfunction in the absence of significant left-sided heart disease) and elevated N-terminal pro b-type natriuretic peptide (NT-proBNP) >300 pg/mL. Lung physiology and 6 min walk test results were also collated, using the last available test prior to death for the pre-MDT cohort or within 6 months of the MDT for the post-MDT cohort.
We evaluated the assessment of patients’ care needs according to documented evidence of (1) recommendation to the general practitioner (GP) to highlight patient on the supportive care register; (2) recommendation for referral to community matrons (nurses who provide advanced clinical nursing care in addition to case management for those patients with high care needs); (3) recommendation for referral to palliative care courses, for example, St Peter’s Hospice fatigue and breathlessness (FAB) management course; (4) initiation of ACP, for example, end-of-life discussions; and/or (5) recommendation for specialist palliative care in hospital setting and/or community as appropriate.
Statistical analysis
Categorical variables are presented as counts, while continuous variables are presented as mean±SEM. Unpaired Student’s t-test was used for comparison of two groups, with or without Welch correction dependent on the variance of data. χ2 testing was used for comparing categorical data. For all tests p<0.05 was considered statistically significant. Data were analysed using GraphPad Prism Software V.7.0 (GraphPad Software, San Diego, California).
Results
Patient characteristics
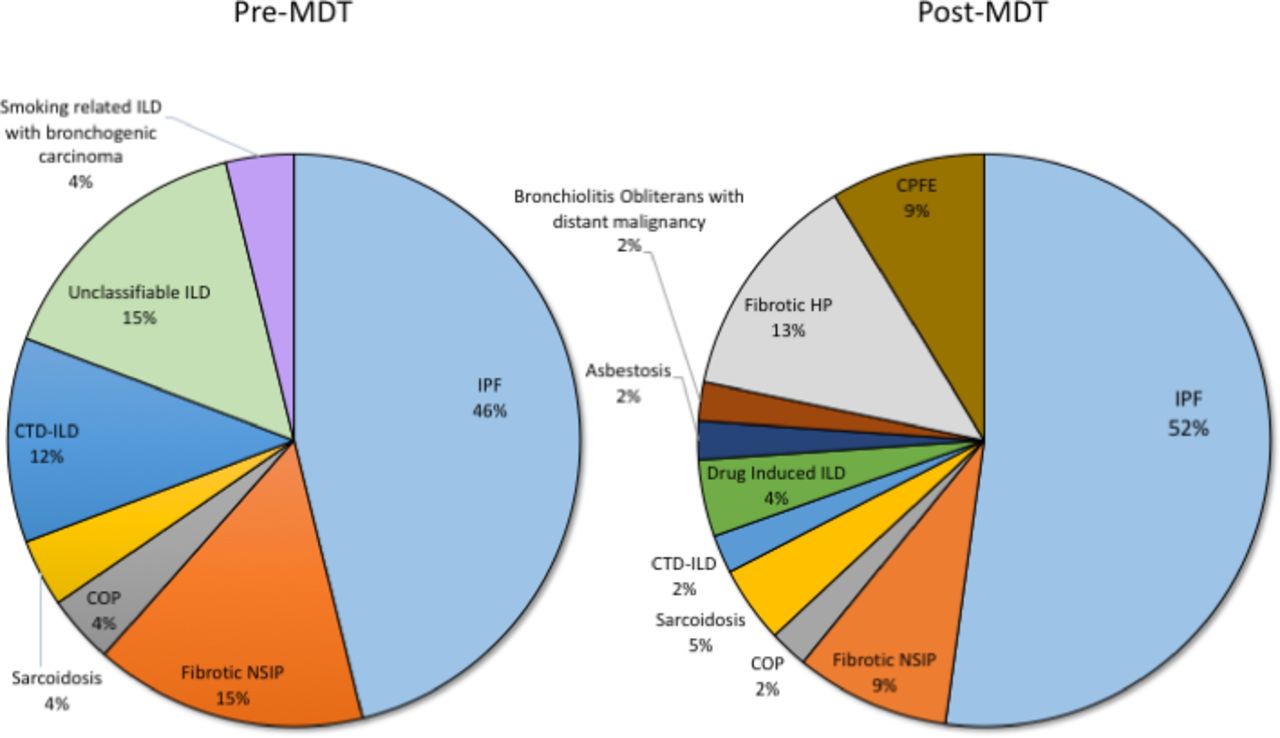
The baseline demographics of pre-MDT and post-MDT cohorts were statistically comparable (table 1). Patients had moderately severe disease as determined by their lung function and evidence of raised NT-proBNP (pre-MDT group 1283±614.2 pg/mL vs post-MDT 1223±305.9 pg/mL), with high dependency on oxygen (pre-MDT cohort 84.6% of patients, post-MDT cohort 93.5% of patients). Patients with IPF comprised the largest subgroup of patients with ILD in both the pre-MDT (46.2%, 12/26) and post-MDT (52.2%, 24/46) cohorts (figure 1).
Patient characteristics of pre-MDT and post-MDT cohorts

Subtypes of ILD in pre-MDT and post-MDT cohorts. Patients with IPF comprised the largest subgroup of patients with ILD in both the pre-MDT and post-MDT cohorts. COP, cryptogenic organising pneumonia; CPFE, combined pulmonary fibrosis and emphysema; CTD-ILD, connective tissue disease-related interstitial lung disease; HP, hypersensitivity pneumonitis; ILD, interstitial lung disease; IPF, idiopathic pulmonary fibrosis; MDT, multidisciplinary team; NSIP, non-specific interstitial pneumonitis.
Impact of the palliative care–psychology–ILD MDT
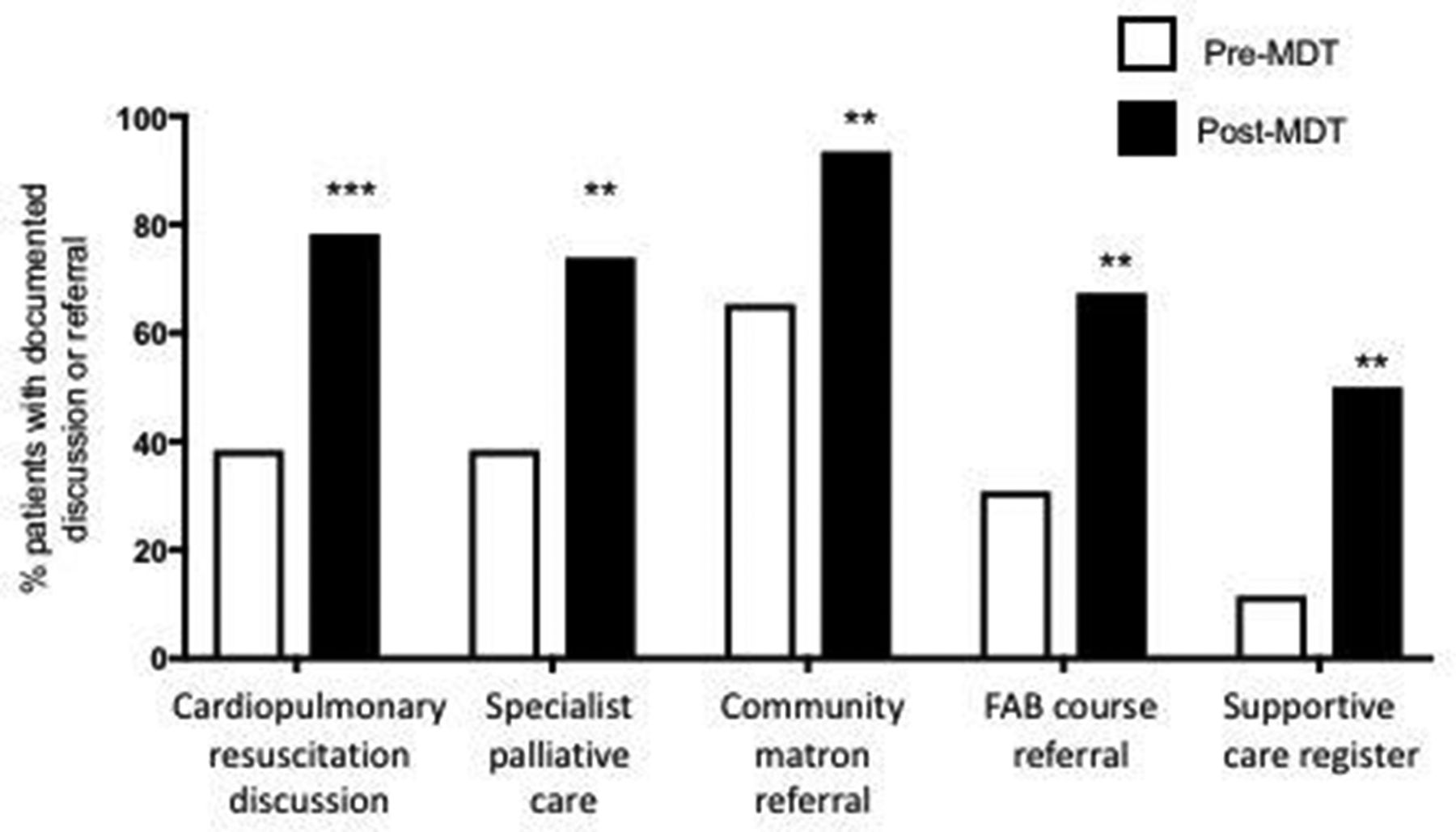
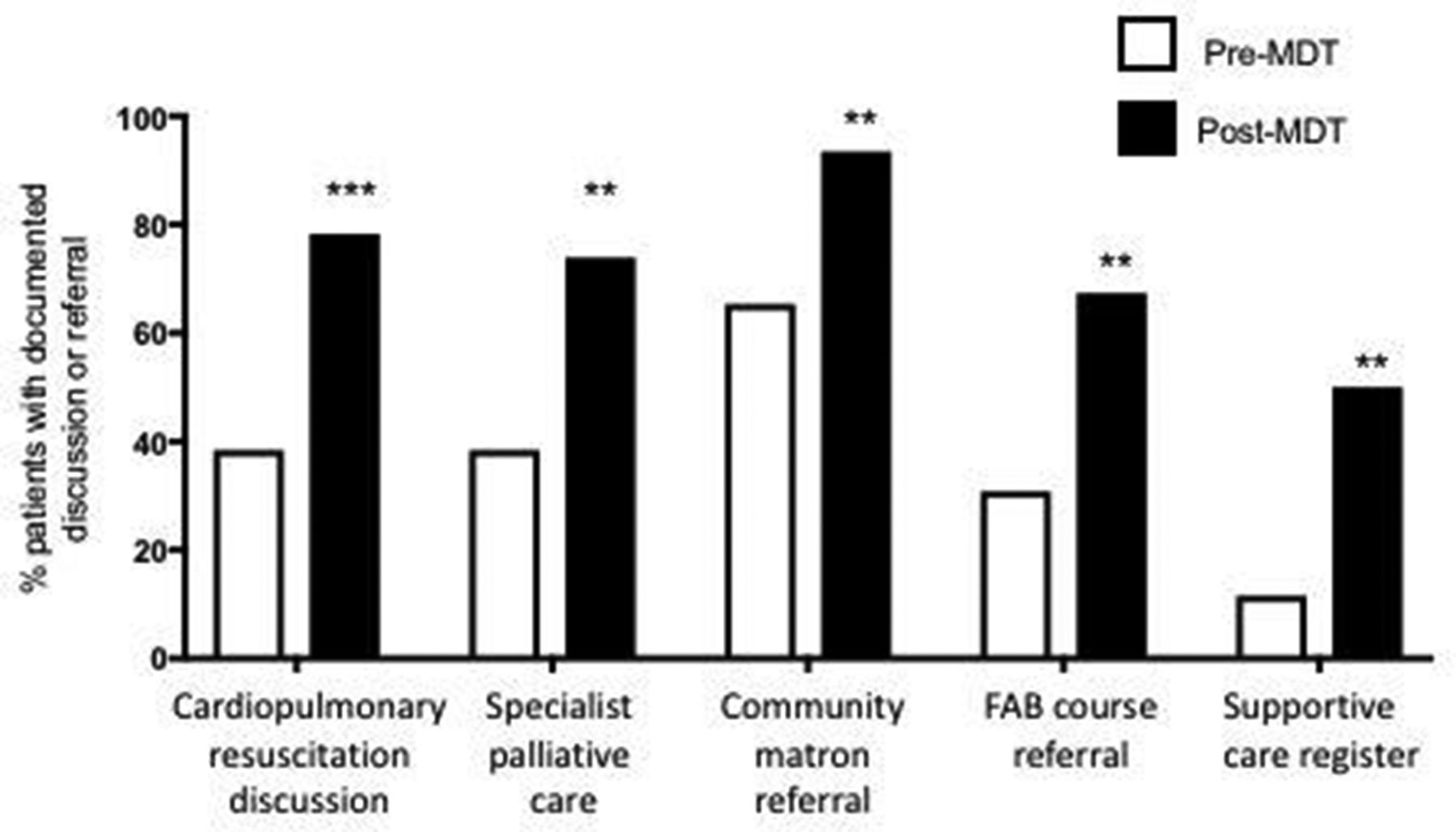
Postintroduction of the MDT, there were statistically significant increases in the documentation of cardiopulmonary resuscitation discussions (pre-MDT 38.5% vs post-MDT 78.3%), increased referrals to the hospice-delivered FAB course (pre-MDT 30.8% vs post-MDT 67.4%) and specialist palliative care services (pre-MDT 38.5% vs post-MDT 73.9%) (figure 2). Additionally, there were more recommendations to GPs to highlight the patient on their supportive care register (pre-MDT 11.5% vs post-MDT 50.0%), with increased referrals to locally available community matrons (pre-MDT 65.4% vs post-MDT 93.5%). The mean survival from discussion in the MDT to death was 159 days (95% CI 114.7 to 204.4 days).
{kind=link}
{kind=link}
Impact of MDT. Postintroduction of MDT, there were statistically significant increases in the documentation of cardiopulmonary resuscitation discussions (pre-MDT 38.5% vs post-MDT 78.3%), increased referrals to the hospice-delivered FAB course (pre-MDT 30.8% vs post-MDT 67.4%) and specialist palliative care services (pre-MDT 38.5% vs post-MDT 73.9%). Additionally, there were significantly more recommendations to GPs to highlight the patient on their supportive care register (pre-MDT 11.5% vs post-MDT 50.0%), with increased referrals to locally available community matrons (pre-MDT 65.4% vs post-MDT 93.5%). Data presented as % of patients with documented discussion or referral, ***p<0.001, **p<0.01. FAB, fatigue and breathlessness course; MDT, multidisciplinary team.
Discussion
Patients with chronic lung disease experience a higher burden of symptoms, worse quality of life, greater functional deterioration and more social isolation, compared with those with cancer,9–12 that are sustained over a longer trajectory.
While it is recognised that best supportive care should be offered to patients with IPF and other forms of PF-ILD from the point of diagnosis,13 their palliative care needs are reportedly often unmet.14 This may reflect the challenge of tailoring their needs according to disease severity and rate of progression in a condition that often has an unpredictable disease course (reflected by the broad CIs between time from discussion in MDT to death in this cohort).
We describe a novel model of care that coordinates allied health professional input to address our patients’ (and caregivers’) physical, psychological and social symptoms/needs, with the provision of a platform for high-quality discussion and subsequent communication to community teams, in keeping with the traditional aims of palliative care.15 16 Significant increases in ACP discussions were observed, in conjunction with increased referrals to community courses and teams to address unmet care needs.
Previous studies have suggested that early palliative care may have an overall survival benefit compared with standard treatment.17 The small sample size of this study prevents accurate interpretation of mortality differences as a direct consequence of this model of care, but we hope to report on this in future studies, exploring reductions in unplanned hospital admissions, achievement of preferred place of death, alongside patient and caregiver feedback.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was approved as a service evaluation project by the North Bristol NHS Trust prior to commencement.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.