Article Text

Abstract
Introduction The British Thoracic Society Sarcoidosis Registry allows physicians to record clinical data after gaining written consent from patients. The registry’s aim is to phenotype sarcoidosis in the UK.
Methods Between February 2013 and July 2017, demographic details for 308 patients (with complete clinical data for 205 patients) presenting to 24 UK hospitals were recorded. This data was analysed to detail methods of presentation, diagnosis and management.
Results Fatigue was a significant complaint, affecting 30% of all patients. The most prevalent CT findings were nodules (in 77% of cases) with traction bronchiectasis (11%), distortion (9%) and ground glass (5%) less prominent. Of 205 patients with complete clinical data, only 64% had a diagnostic tissue biopsy. 35% of all patients underwent endobronchial ultrasound-guided transbronchial needle aspirate (EBUS-TBNA) with 15% having a transbronchial biopsy. Use of EBUS-TBNA showed an overall increase over time, from 28% of all patients in 2013 to 43% in 2016. The most common steroid sparing treatment was methotrexate, but 42% of patients were not initiated on any pharmacological treatment at the time of inclusion.
Discussion Fatigue was common and has shown association with poor quality of life. We therefore suggest using a fatigue questionnaire as part of all new patient assessments. It may be that EBUS-TBNA should be reserved for cases of stage I or II disease where there is a reported higher yield than using transbronchial biopsy alone. Bronchoalveolar lavage was not widely used in our data, but it is generally a safe and useful adjunct and should be used more widely.
- sarcoidosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the phenotype of patients with sarcoidosis presenting to hospital clinic in the UK?
We made a number of conclusions from the data including that fatigue is a common complaint, use of endobronchial ultrasound-guided transbronchial needle aspirate is increasing over time and methotrexate is the most commonly used steroid-sparing agent.
Sarcoidosis is a complex and challenging disease to diagnose and manage. Collection of registry data such as these will help standardise clinical practice and allow research to be targeted to areas where there is a larger disparity in how patients are managed.
Introduction
Clinical data registries are useful in complex diseases where data can be collated for research purposes. To our knowledge, the British Thoracic Society (BTS) Sarcoidosis Registry is the only database in the world which allows physicians to record data after gaining written consent from patients with sarcoidosis. The aim of the registry is to record information to phenotype the disease in the UK.
European Respiratory Society (ERS)/American Thoracic Society/World Association of Sarcoidosis guidance on sarcoidosis is now almost 20 years old,1 and there is no recent international guidance on diagnosis and management of the disease. This is despite a number of more recent changes including the advent of endobronchial ultrasound-guided transbronchial needle aspirate (EBUS-TBNA) for tissue diagnosis which is not discussed in the previous ERS guidance.
A decision was therefore made by the BTS to perform an interim analysis on data collected to date with the specific aims of providing a clear interrogation of data from areas where the authors felt there was limited prior evidence for specific approaches in the diagnosis and management of sarcoidosis. As part of this process, a steering committee of the authors was formed to review all data collected to date and identify areas of greatest interest. Through this process, a number of areas were identified and these are presented here. There were three specific areas of interest to the committee: (1) the proportion of patients undergoing a tissue biopsy, (2) the type of biopsy performed in these patients and (3) the use of steroid-sparing agents in the management of sarcoidosis. The rationale for choosing these specific areas is associated with the lack of prior evidence regarding how to make a diagnosis of sarcoidosis, in which patients to perform a biopsy and in cases where medication additional to steroids are needed, which agents are used.
The data is collected over the course of a single visit but may be updated onto the web portal over a period of time (eg, up to several months later once physicians have had time to collect all relevant clinical information for that case). As such, the data record is opened using demographic data only but is not marked as ‘complete’ until all the clinical information is entered and the record is locked. This resulted in approximately 70% of patients having a complete data set for this interim analysis (as detailed in the Methods section below), but over time this number is increasing, for example, as of 23 November 2018, 75% of all entries have a complete data set. We anticipate that this percentage will rise over time as more cases are fully completed. The web tool to input data can be found at: https://registry.brit-thoracic.org.uk/ An example of the full sarcoidosis registry tool with all data collection points is given in the online supplementary appendix 1.
Supplemental material
Methods
The Registry was launched on 1 February 2013 with full ethical approval (NRES reference:12/EE/0381). Participation is open to all UK Physicians. Patients must provide written consent. Data is collected at time of presentation to the clinic and entered onto a web-based platform. The registry is associated with the Idiopathic Pulmonary Fibrosis registry and this means that clinicians may sign up for both registries together.
Between February 2013 and July 2017, demographic details for 308 patients (with complete clinical data for 205 patients) presenting to 24 UK hospitals were recorded (see online supplementary appendix 2 for full distribution by site). A steering committee was formed to review data for this interim analysis and make decisions on how to review and present the data. The manuscript was primarily written by MT and RC but all co-authors have reviewed and commented on the data presentation. The registry data is currently available for access by the BTS registry team and data is shared at international conferences.
Supplemental material
Results
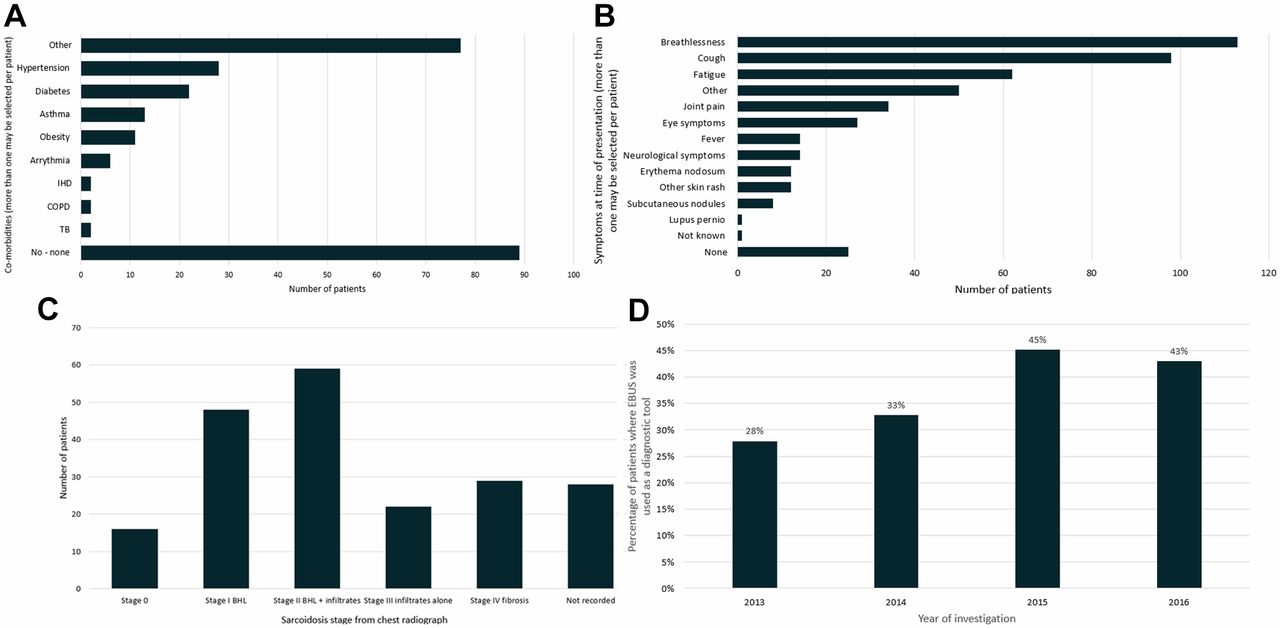
A retrospective analysis of the 308 patients showed that mean age at inclusion was 50 years. Fifty-eight per cent were male and 64% Caucasian. Most had never smoked (64%) or were ex-smokers of >3 months duration (26%). Patients (3.7%) reported at least one first-degree relative with sarcoidosis. Forty-three per cent had no significant comorbidities, while 14% had a diagnosis of essential hypertension and 11% type 2 diabetes (figure 1A). Respiratory symptoms were the predominant complaint with 55% having breathlessness and 48% cough. Fatigue was significant at 30% (figure 1B). The Medical Research Council (MRC) breathlessness score showed 48% of patients recorded as category I, 32% category II and 10% category III.
{kind=link}
(A) Comorbidities at the time of diagnosis. (B) Presenting symptoms in sarcoidosis. (C) Sarcoidosis stage from chest radiograph. (D) Use of endobronchial ultrasound-guided transbronchial needle aspirate for diagnosis over time.
With respect to Scadding classification of chest radiographs, these were recorded as stage 0 (8%), I (24%), II (29%), III (11%), IV (14%) with the remainder unrecorded (figure 1C). The most prevalent CT findings were nodules (seen in 77% of cases) with traction bronchiectasis (11%), distortion (9%) and ground glass (5%) featuring less prominently.
Pulmonary function testing revealed predicted forced vital capacity at the time of inclusion ranging from 101.2% predicted for Scadding stage 0, to 92.8% predicted for stage IV. Mean predicted forced expiratory volume in one second showed a trend with stage from stage 0 (98.1%) through to stage IV (81.4%). Mean transfer factor for carbon monoxide at inclusion was 78.2% predicted. The most common blood abnormalities (both in 49% of cases) were lymphopenia and a raised serum ACE (>55 IU/L) with a mean of 67.5 (range 3–221). Other blood abnormalities included a raised erythrocyte sedimentation rate (20%), abnormal liver function tests (17%) and raised serum calcium (10%).
Of 205 patients with complete clinical data, only 64% had a tissue biopsy, the remaining 36% had a clinic-radiological diagnosis only. When biopsies were performed, 79% were intrathoracic with extrathoracic lymph nodes (7%) and skin (6%) next most common sites. Thirty-five per cent of all patients in the registry underwent EBUS-TBNA, 15% transbronchial biopsy (TBBX), 11% endobronchial biopsy and 13% bronchoalveolar lavage (BAL). Twelve per cent of patients had a mediastinoscopy. Use of EBUS-TBNA showed an overall increase over time, from 28% of all patients in 2013 to 43% of all patients in 2016 (figure 1d).
At presentation, 39% of all patients were treated with oral corticosteroids. The second most common treatments were methotrexate and inhaled corticosteroids (8% each). Forty-two per cent of patients were not initiated on any pharmacological treatment at the time of diagnosis.
Discussion
We present data from 308 patients enrolled into the BTS Sarcoidosis Registry between 2013 and 2017. The aims of the analysis were review the entire data set and concentrate specifically on areas where the BTS committee felt there was the least amount of prior evidence. The two areas of greatest interest were regarding biopsy for diagnosis and the use of steroid sparing agents.
With regard to biopsy for sarcoidosis, until recently, there was debate about the role of EBUS-TBNA.2 However, a recent study showed that as a single modality, EBUS-TBNA had the highest diagnostic yield at 74.5%, and addition of TBBX increased this to 91%.3 The choice and combination of diagnostic modalities is still unclear, but in our data EBUS-TBNA is more commonly used than TBBX. It may be that EBUS-TBNA should be reserved for cases of stage I or II disease where there is a reported higher yield than using TBBX alone.4 BAL was not widely used in our data. However, CD4:CD8 >3.5, in the absence of an increased proportion of other inflammatory cell types, may help support a diagnosis of possible sarcoidosis.5 BAL is generally a safe and useful adjunct and we argue that it should be used more widely in sarcoidosis, especially in cases where a transbronchial lung biopsy confers greater risk of bleeding or pneumothorax or in cases where extensive fibrosis means that a lung biopsy may have a low accuracy for diagnosis of sarcoidosis.
Identification of the both the proportion of registry patients who had a biopsy and in those who had a biopsy the type of procedure performed is an important finding from this data set. However, a further analysis will be needed to distinguish differing factors between the patients who had a biopsy and those who did not, as well as between the types of biopsy, for example, whether the extent of radiological changes influenced the type of bronchoscopic procedure performed.
The second main aim for this data analysis regarded the use of non-steroid agents in the pharmacological management of sarcoidosis and in this respect we feel our findings are important. Inhaled corticosteroids were used in 8% of registry patients and while there is evidence that an obstructive lung defect is present in almost a quarter of UK patients with sarcoidosis,6 studies have shown conflicting evidence with some showing improvement in lung function7 and others showing no benefit.8 One study with fluticasone showed no benefit against placebo but an improvement in cough.9 There are arguably no convincing studies to support the evidence of one steroid-sparing drug over another and the choice of agent used is often influenced by local specialist experience. However, as with previous Delphi studies, methotrexate was our commonly used second-line drug.10
Two additional important findings from our analysis involve patients with a family history sarcoidosis and the symptoms recorded at time of presentation. In our data set, 3.7% of all patients reported a family history of sarcoidosis. The only previous UK study to report familial associations received questionnaires from 268 patients and found similar results in that 5.2% had at least one first-degree, second-degree or third-degree relative with sarcoidosis.11
With regard to symptoms, fatigue was common (30%) and has shown association with poor quality of life.12 The aetiology is multifactorial including granuloma formation, depression, altered sleep patterns13 and use of corticosteroids.14 Fatigue is difficult to quantify, but the Fatigue Assessment Scale can differentiate between sarcoidosis fatigue and depression.15 We found no difference in fatigue presentation between men and women which contrasts with a recently published European phenotyping study of 2163 Caucasian patients where fatigue was seen at a higher incidence in women.16 Although the registry does not record the likely cause of fatigue, given the prevalence in our data, we suggest routine use of a fatigue questionnaire both as part of all new patient appointments and as a longitudinal assessment for patients who have difficult to manage fatigue.
The inferences of our findings are subject to some general limitations. Importantly, there is bias towards selective UK sites as although 24 hospitals entered data, it is possible that these represent sites where there are clinicians who have a specific interest in sarcoidosis. Indeed, of the 24 hospitals, 11 of them are designated tertiary centres for interstitial lung diseases where there may be a greater access to specialist services. It would be important to capture further data from general respiratory clinics as well as from these specialist ones. Additionally, we do not have information on whether the absence of a biopsy influenced the decision to offer treatment, given that in some cases, physicians may be less likely to initiate pharmacological treatment without a definite tissue diagnosis. Finally, few patients had follow-up data. More detailed longitudinal capture may prove useful in determining how often patients are followed up and when they can be discharged from specialist care.
Collection of data across multiple sites has both advantages and limitations. In a disease such as sarcoidosis with significant variation in practice and a lack of clear evidence on diagnostic and management pathways, multisite data collection allows researchers to review variations in practice across different institutions and provide support to experts as they write the next set of clinical guidelines for the disease. However, a significant limitation is the lack of standardisation of data collection across sites. For instance, although patients may have the same investigations, the interpretation of some of these is not standardised, for example, the finding of abnormalities on CT scans or the reporting of chest X-ray stage by Scadding classification. In order to mitigate against these variations, a central method of analysis and recording of all data is needed, but this will have significant logistical and financial implications due to the need for data transfer, centralised reporting of imaging and review of clinical records. Such a centralised process would therefore improve the accuracy of data collection but may be prohibitively expensive to attain.
As the BTS registry grows in volume of patient records, a number of important new questions will need to be asked which will require further analysis of the data and may require new data points for entry. First, as detailed in the original aims for this analysis, there is no clear evidence on either the need for a biopsy or in cases where tissue is obtained, the type of biopsy used to diagnose disease. A future approach to the registry will be to perform a subanalysis on the radiographic differences between patients who had a biopsy and those in whom a diagnosis was made on clinico-radiological grounds alone. This analysis may require a more detailed collection of CT imaging findings but may allow us to determine the radiological phenotype of patients in whom a biopsy is performed, for example, in those without classical CT findings such as bilateral hilar lymphadenopathy alone with no concerning radiological or clinical features to suggest an alternative diagnosis. Additionally, a further analysis is needed to determine whether the CT appearance influences the method of biopsy, for example, whether patients with predominantly hilar disease are subjected to EBUS-TBNA compared with those with predominantly parenchymal disease who may have TBBX. These findings would be important to both support future clinical statements in sarcoidosis and to design larger studies to help determine which type of biopsy to perform for a given phenotype of sarcoidosis.
Second, further questions need to be asked regarding the use of steroid-sparing agents. Our findings identified methotrexate as the most commonly used drug, but the registry currently has limited follow-up data on these patients. A targeted approach to specifically record longitudinal data on patients prescribed steroid-sparing agents will allow us to record the clinical outcome, changes in lung function and blood biomarkers and the incidence of side effects including fibrosis or liver toxicity. Such data would be important in helping design future trials with both traditional steroid-sparing agents and any novel medications to determine their use in the pharmacological management pathway for sarcoidosis.
Finally, it is noteworthy that none of the 308 patients were enrolled in clinical trials at the time of data capture. This may reflect the lack of available clinical trials for this disease, rather than a lack of enthusiasm for physicians to enter patients into trials. Sarcoidosis is a complex disease and drug regimens used have not been proven in randomised controlled trials. New treatments are needed for patients with multisystem and progressive forms of disease. One important use of such a patient registry may be to address this gap by identifying patients for new clinical trials.
Acknowledgments
The British Thoracic Society would like to thank the Maria Loughenbury for her assistance with manuscript preparation as well as the sites which contribute to the ILD Registry: England: Addenbrooke's Hospital, Birmingham Heartlands Hospital, Castle Hill Hospital, Central Middlesex Hospital, Cheltenham General Hospital, Churchill Hospital, Countess of Chester Hospital, Croydon University City Hospital, Darlington Memorial Hospital, Ealing Hospital, George Eliot Hospital, Gloucestershire Royal Hospital, Good Hope Hospital, Guy’s Hospital, Hammersmith Hospital, Harrogate District Hospital, Hinchingbrooke Hospital, King’s College Hospital, Liverpool Heart and Chest Hospital, Musgrove Park Hospital, New Cross Hospital, Norfolk and Norwich University Hospital, North Devon District Hospital, Northern General Hospital, North Middlesex University Hospital, Northwick Park Hospital, Nottingham City Hospital, Peterborough City Hospital, Queen Alexandra Hospital, Queen Elizabeth Hospital, Royal Devon and Exeter Hospital, Royal Free Hospital, Royal Lancaster Infirmary, Royal Papworth Hospital, Royal Victoria Infirmary, Solihull Hospital, Southampton General Hospital, Southmead Hospital, St James’ University Hospital, St Mary’s Hospital, University College Hospital, University Hospital (Coventry and Warwickshire), University Hospital Aintree, University Hospital of North Midlands, University Hospital of North Tees, Wansbeck Hospital, Wythenshawe Hospital. Scotland: Aberdeen Royal Infirmary, Glasgow Royal Infirmary, Lorn and Islands District General Hospital, Royal Alexandra Hospital, Vale of Leven District General Hospital. Wales: Glan Clwyd Hospital, University Hospital Llandough, Wrexham Maelor Hospital. Northern Ireland: The Ulster Hospital.
References
Footnotes
Contributors All authors contributed to the planning and drafting of the manuscript, MT and RC took overall responsibility for the final document, All authors approved the final manuscript.
Funding The BTS ILD Registry (including the Sarcoidosis Registry) is fully funded by British Thoracic Society. A grant from HQIP contributed to the initial development of the Registry (from 2012 to 2014) and the data collection software was enhanced in 2014 due to financial assistance from Boehringer Ingelheim and InterMune.
Competing interests NC and MT received funding from Roche, BI; LGS and IF received funding from BI. TMM received funding from Roche, BI, Biogen, Bayer, GSK, UCB,
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.