Article Text

Abstract
Background Breathlessness, the subjective sensation of breathing discomfort, is common and appears in the daily life of people with cardiorespiratory diseases. Physicians often rely on patient’s history based on symptom recall. The relation between recalled and experienced breathlessness is still poorly understood. This paper presents the protocol for a study primarily aimed at evaluating the relationship between experienced breathlessness and (1) recalled breathlessness and (2) predicted future breathlessness.
Methods A mobile phone application will be used to collect data during daily life. Medically stable participants, ≥18 years of age with mean daily breathlessness of Numerical Rating Scale (NRS) 3/10 and able to use a mobile phone with internet will rate their breathlessness intensity on a 0–10 NRS prompted the user several times daily for 1 week. Participants will recall their breathlessness each day and week. Multivariable random effects regression models will be used for statistical analyses.
Results Results of the study will be submitted for publication in peer-reviewed journals and presented at relevant conferences.
Discussion This protocol describes a study aimed at investigating previously unknown areas of the experience and recall of breathlessness using a new method of data collection.
Registration details Prospectively registered with ClinicalTrials.gov (Nr: NCT03468205).
Ethics and dissemination The study has received ethical approval from the Regional Ethical Review Board Lund (DNr 2017/149). After a general study information including that participation is entirely voluntary, participants will answer the eligibility criteria and be asked to consent to participate before entering the study questions. Written informed consent to participate will be obtained for participants in the clinical sub-cohort. Participation can be discontinued at the discretion of the participant in which case no further data will be collected.
- breathlessness
- dyspnoea
- recall
- mobile phone application
- app
- cohort study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Novel method of collecting data in this field—continuously in daily life through a mobile phone application.
Investigating previously poorly understood areas of the experience and recall of breathlessness.
Multidimensional approach to breathlessness.
Easy to expand or modify study procedure for use in other settings.
One limitation might be the low level of control of included participants in the general cohort.
Introduction
Breathlessness, the subjective sensation of breathing discomfort, is common and appears with varying severity in daily life of people across several diseases such as congestive heart failure, asthma and chronic obstructive pulmonary disease (COPD).1–3 Breathlessness affects nearly a quarter of people aged over 60 years and about half of patients with serious illness.1–3 It is associated with increased anxiety and depression, increased risk of hospitalisation and earlier death.4 5 Several qualitatively distinct sensations of varying intensity constitute breathlessness making it a multidimensional symptom. These dimensions include the experienced intensity and unpleasantness, the associated emotional response and the functional impact on the person’s life.6
Clinical care relies on the patient’s history based on his/her symptom recall. The recalled level of recent breathlessness is used by the health professional to decide on the need for further investigations and treatment. Studies have shown that the recalled intensity of breathlessness during laboratory-provoked symptoms is not the same as the symptom actually experienced in daily life.7 This mismatch has also been shown for other measures for pain or self-perceived happiness.8 Further, previous studies show poor communication about breathlessness between doctors and patients, and ratings performed by healthcare professionals and caregivers of the patient’s symptom severity often do not match. This problem increased with higher levels of symptoms.9 Lack of communication and understanding of the patient’s symptoms lead to poor concordance, inappropriate treatment decisions and influence the patients adherence with treatment.9–11 The gold standard for assessing the symptom severity is currently patient recall.
Several factors may influence the recalled symptom intensity including the highest and the final experienced intensity.12 13 This association is often referred to as the ‘peak-end rule’ and has been found to be important for the overall recall of pain and happiness.12 13 Studies evaluating the ‘peak-end rule’ in breathlessness have previously shown contradictory results between groups.14 The current intensity of breathlessness is the measure shown to be the most associated with the recalled intensity.15 Additionally, even a very small decline in cognitive status influenced the differences between recalled and experienced symptoms, giving a bigger difference and increased variance between actual and recalled symptoms.15
No previous studies exist on how patients own predictions of future breathlessness influence the actual and recalled breathlessness. The hypothesis that patients own predictions may influence the actual intensity of breathlessness will be tested in this study.
This paper presents the protocol for a study of the relationship between experienced and recalled breathlessness with contemporaneous data collected using a mobile phone application. Through this, new information will be gathered on which factors that influence patients recall of breathlessness which is the foundation of several important clinical decisions regarding treatment and evaluations. Better understanding of these issues may thus have a big impact in the daily interactions between breathless individuals and their doctors. Specific research questions are presented in box 1.
Research questions
Three types of breathlessness measures evaluated: experienced (at a time point), recalled (remembered) and predicted (future) breathlessness. The main research questions are:
1 How is the recalled breathlessness intensity for a time period (T1) related to:
1.1 Experienced breathlessness intensity during T1 measured as:
1.1a Mean experienced intensity?
1.1b Peak experienced intensity?
1.1c Most recent experienced intensity?
1.1d Perceived self-efficacy related to the breathlessness?
1.1e Personality trait of high symptom sensitivity at baseline?
1.2 Predicted breathlessness intensity for a future time period (T2)?
2 How is the predicted breathlessness intensity for a subsequent time period (T2) related to:
2.1 Experienced breathlessness intensity during T1?
2.2 Recalled breathlessness intensity during T1?
2.3 Experienced breathlessness intensity during T2?
3 Which factors are associated with the difference score between:
3.1 Experienced and recalled breathlessness intensity during T1?
3.2 Predicted and experienced breathlessness intensity during T2?
Aims
The primary aim is to evaluate the relationship between experienced breathlessness and (1) recalled breathlessness and (2) predicted future breathlessness. Secondary aims are to identify factors that influence the difference between experienced and recalled or predicted breathlessness, to evaluate how people think when they recall breathlessness over defined time periods and to evaluate a novel method of collecting data in this field. (box 1)
Methods and analysis
Study design and population
Inclusion criteria are age ≥18 years with a self-reported breathlessness intensity ≥3 on a 0–10 Numerical Rating Scale (NRS) during the prior 2 weeks not caused by an acute infection such as an upper respiratory tract infection or pneumonia. Participants should be clinically stable without expected need for hospital admission within 1 week, be able to walk without a personal aid (rollator allowed), be able to use a device (smartphone/pad) with internet access regularly and be able to read and complete baseline assessments. The default setting is 1 week of participation, but there is a possibility to continue for additional weeks at the discretion of the participant. Participants will be recruited into two different cohorts, one general cohort which include most participants and one smaller clinical subcohort study with fewer participants but with added data.
Recruitment
Potential participants will be identified by clinical and research staff at the centres of the participating investigators including primary care, pulmonary clinics and internal medicine/cardiology departments in Blekinge, Örebro and Skane University Hospitals (Lund/Malmö). Participants will also be recruited through advertisements in national and local newspapers and magazines including those of the Swedish Respiratory Society, the Swedish Heart-Lung Foundation and the Heart-Lung Association and on webportals/sites.
Mobile phone application-based data collection
The mobile phone application is available on the two major mobile platforms in the market today (iOS and Android) and can be downloaded for free through their respective distribution channels (ie, ‘App Store’ for Apple and ‘Google Play’ for Android) and installed directly on the participants’ personal mobile phones. It was developed by the company ‘Cybercom group’ in close collaboration with the authors of this article and tested repeatedly for functionality in pilot-testing by authors and a small group of healthy volunteers. To access and start the active survey a four-digit code is needed which is distributed to participants by research staff or through the advertising. Baseline data will be recorded when starting the application and individual daily start and stop times will be set. At regular intervals during each day, the application will cue the participant, using sound and homepage notifications, to self-rate the intensity of breathlessness during the last 10–15 min. Each cue can be ignored or filled in later. Recall of breathlessness during the preceding night or day and additional measurements are rated in the application each morning and, for the whole week at the end of each week in the study (figure 1). The participant can quit the application at any time and will be asked to complete the cessation/exit assessments for the completed part of that week. If any problems or questions arise during the study period, there is a help section within the application with an email address to the primary investigators. All application data, linked to the participant-specific study ID, is encrypted and transferred to a central database in real time via the internet connection. If no internet connection is available at the time of transfer or if for some reason the data transfer is interrupted, the data will be stored locally on the device and the application will try to resend when the connection is re-established and stabilised. The data will also be kept on the device until the end of the study as a safeguard to create a redundancy.
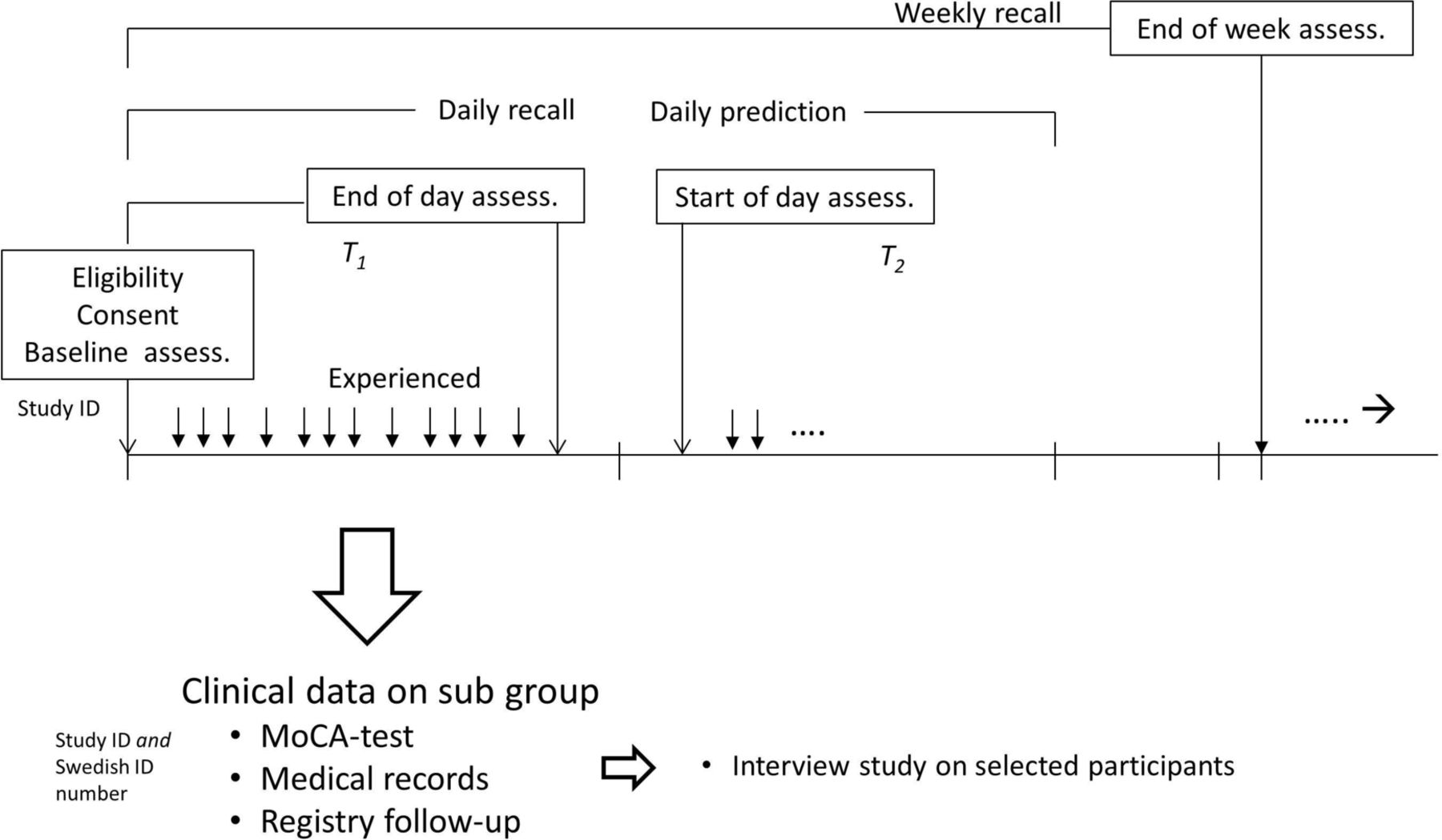
{kind=link}
Overview of the timing of planned assessments, starting with eligibility, consent and baseline assessments then continuing with several daily prompts asking on intensity of breathlessness as well as morning, evening and weekly assessments including daily recall and daily predictions as well as a weekly recall.
Clinical substudy
A subset of participants at the study centres will be asked to participate in a clinical substudy. In addition to the information regarding the main application-based study, these participants will receive specific information about the substudy on paper and be asked to give their written informed consent to participate. Data including demographics, diagnoses, measures of pulmonary and cardiac function, treatments and hospitalisations will be obtained from medical records and national registries with up to 5 years follow-up of diagnoses and hospitalisations (Patient Registry), dispensed medications (Prescribed Drug Registry) and survival (Causes of Death Registry). Participants in the clinical substudy will be assessed for cognitive impairment at the beginning of the study. Some participants will also be invited to take part in a semistructured qualitative interview focusing on their experience of breathlessness and specifically how they cognitively recall breathlessness over different time periods such as ‘now’, ‘last 24 hours’ or ‘last week’. This group of participants will also be interviewed shortly about their experiences on using the mobile application. A separate study protocol and analysis plan will be developed before starting the qualitative substudy.
Assessments
All planned assessments and scales within the application are presented in table 1. Some modifications and new questionnaires were adapted.
Overview of the questionnaires and scales used
Supplemental material
Breathlessness will be assessed using cued questions several times each day asking, ‘How intensive has your breathlessness been in the past 10–15 min?’, rated between 0 (no breathlessness) and 10 (worst imaginable breathlessness). The same type of assessment will be cued each morning (‘How intensive has your breathlessness been during the past night?’) and evening (‘How intensive has your breathlessness been during this day?’), as well as for the whole week (‘How intensive has your breathlessness been during the past week?’). The user will also be asked to predict, using a similar 0–10 NRS scale, how the intensity of breathlessness will be during the coming day, night or week using the question ‘How intensive do you expect your breathlessness to be in the coming day/night/week?’.
The Patient Health Questionnaire (PHQ) is a self-administered version of the Primary Care Evaluation of Mental Disorders diagnostic instrument for common mental disorders which are in the public domain and free to use in research. The PHQ-15 comprises 15 somatic symptoms from the PHQ, each symptom scored from 0 (‘not bothered at all’) to 2 (‘bothered a lot’).16 A minor modification was made in this study by removing one question (pain or problems during sexual intercourse) as the question, during pilot testing, was not deemed to be fully appropriate to ask in this format. The total score of PHQ-15 will be recalculated due to having one question missing in accordance to the instructions from the American Psychiatric Association.17
To assess the self-efficacy of breathlessness, an NRS will be used with the question ‘How confident are you that you can manage breathing difficulty or avoid breathing difficulty during the day’ anchored at 0 (Not at all confident) and 10 (Very confident).
Before and after the main study, the user will be asked some general questions concerning technical knowledge and previous experience on using a smartphone (online supplementary appendix 1a). After the study, some questions will be asked to evaluate the user’s experiences on using the application (online supplementary appendix 1b).
For the participants in the clinical substudy, Montreal Cognitive Assessment Tool (MoCA) will be used to assess for cognitive impairment.18 19 MoCA is a brief and sensitive test for cognitive impairment, assessing visuospatial and executive functions, verbal ability, episodic memory, orientation and attention.19 It has been validated in numerous diseases, including cognitive impairment related to dyspnoea, COPD and heart failure.20–22
Power and sample size
To obtain a power of 80% to detect a clinically and statistically significant difference of 1 point on a 0–10 NRS between the mean experienced and the recalled daily breathlessness score, assuming a pooled SD of 1.81 points, a minimum of 30 participants need to be included into the main study. This is consistent with the sample size of Meek et al .15 To account for loss of data and ensure adequate power, at least 45 participants with data for at least 2 days will be included prior to analysis of the primary research question. The data collection will continue even after this sample size is reached in order to answer also secondary research questions. Specific statistical analysis plans will be developed for each objective.
Statistical analyses
Baseline characteristics will be tabulated using standard descriptive statistics. Mean, peak and end values of experienced, recalled and predicted breathlessness will be graphed and cross-tabulated. Associations between experienced, recalled and predicted breathlessness will be analysed using a mixed model repeated measures approach. Predictors of the difference score between recalled and experienced breathlessness, and between predicted and subsequently experienced breathlessness, respectively, will be analysed using multilevel mixed effects linear regression. Models will then be adjusted for potential confounders including age, sex, body mass index, level of anxiety, depression and functional status. The choice of an appropriate covariance structure will be evaluated.
The minimal clinically important difference score is defined as a 0.5 (small) and 1.0 (moderate/large) change in NRS score.23 The percentage of difference scores ≥0.5 and ≥1.0 points will be calculated.
Statistical significance will be defined as a two-sided p value of <0.05.
Confidentiality
In the application, data are de-identified using a study ID number. For patients who do not participate in the clinical substudy, the Swedish social security number is not recorded. For patients in the clinical substudy, clinical data will be cross-linked with data collected through the application using a key between the study ID (used in the application) and the participant’s Swedish social security number stored securely at the clinical centre.
The database used for the unidentified clinical data is located physically at Blekinge Institute of Technology and is used for several other clinical studies including the Swedish National Study of Ageing and Care (http://ltblekinge.se/snac) following all relevant protocols for data security and integrity. The code key containing the identifier are kept in a locked cupboard on a computer/USB memory not connected to the Internet.
Dissemination
Data will be presented on the group level only, ensuring that individual participants cannot be identified. The findings will be published in national and international peer-reviewed scientific journals and presented on relevant scientific conferences. The de-identified data will be posted in an open access data repository in accordance with the requirements of the scientific journal. Planned future papers will be concerning main and secondary endpoints as well as qualitative analyses on breathlessness measurements.
Authorship will be determined in accordance with the International Committee of Medical Journal Editors guidelines.
Discussion
This protocol describes a study aimed at investigating previously unknown areas of the experience and recall of breathlessness. This study also uses and evaluates a novel way of data collection which could prove to have numerous other applications in other research fields as well as in the current one. A potential limitation of this study is that there will be a low level of control over participants included into the general cohort. This will be regulated by giving out the four-digit code, which is needed to start the application, only to a selected population where breathlessness is anticipated to be highly prevalent. The Relating Experienced To Recalled breathlessness Observational study will answer several important questions such as the impacts and covariates of a breathless patients’ symptom recall. This issue has not been addressed previously and knowledge from this study could be used both clinically (to better understand patients) and in research (to better evaluate participants’ breathlessness reports). This study will further use the multidimensional dyspnoea profile in the assessments and analyses of breathlessness recall and experience which have not previously been used.
Acknowledgments
The authors would like to thank Håkan Lövkvist PhD, Clinical Studies Sweden, Unit for Medical Statistics and Epidemiology, Skåne University Hospital, Lund, Sweden, for valuable help concerning the statistical methods.
References
Footnotes
Contributors ME and JS contributed to the conception and drafting of the article. All authors contributed to the study design and revised the article for important intellectual content and approval of the version to be published.
Funding Jacob Sandberg was funded by an unrestricted grant from the Scientific Committee of Blekinge County Council. Magnus Ekström was supported by unrestricted grants from The Swedish Society of Medicine, the Swedish Respiratory Society, the Swedish Heart-Lung Foundation, the Scientific Committee of Blekinge County Council, the Wera and Emil Cornell Foundation, and the Swedish Society for Medical Research.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.