Article Text

Abstract
Introduction People living with HIV (PLWH) are more likely to smoke than the general population and are at greater risk of smoking-related illness. Healthcare services need to address this burden of preventable disease.
Methods We evaluated the impact of a brief intervention that asked service users about smoking when they attended for ambulatory HIV care in London, UK, and offered referral to smoking cessation.
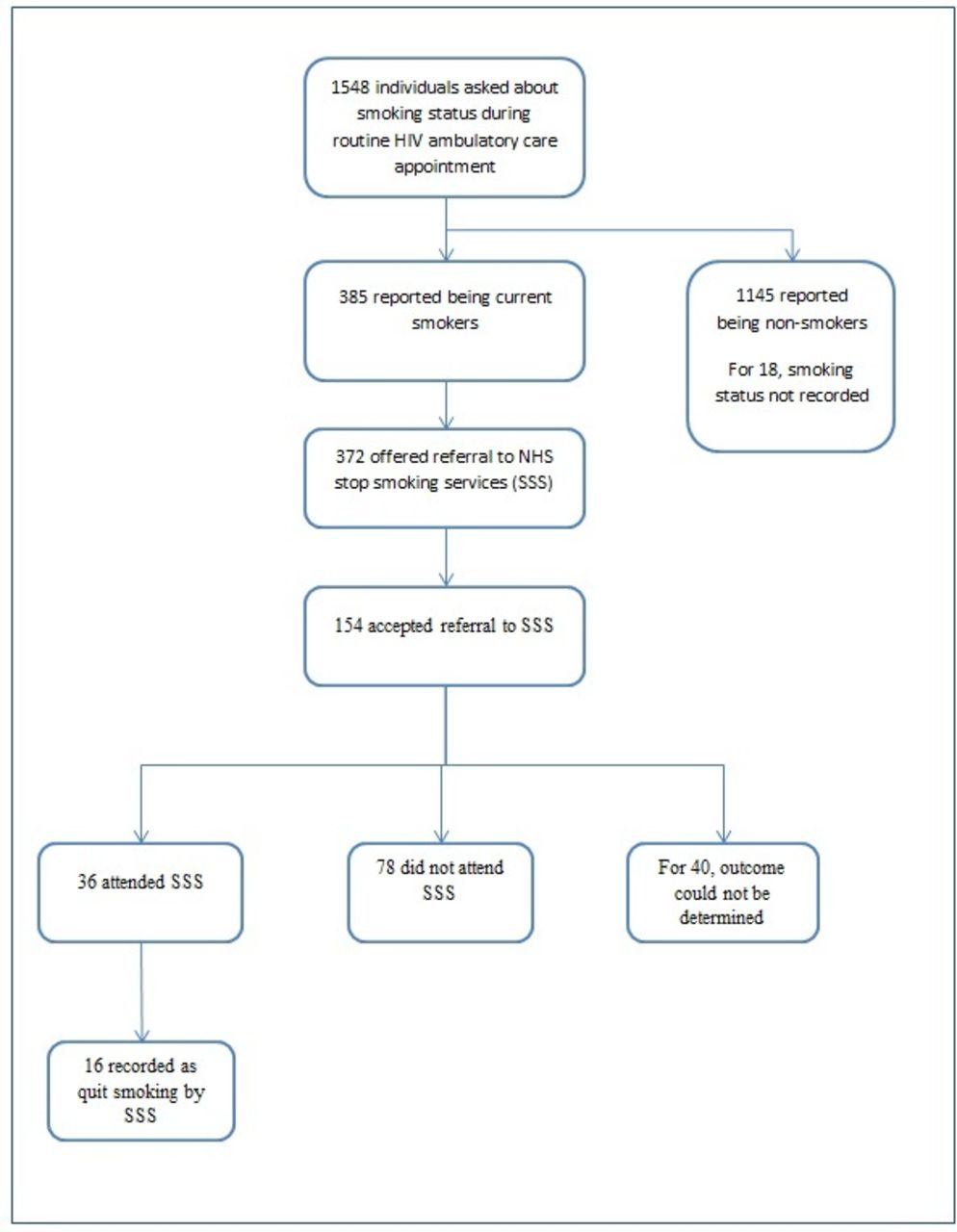
Results Overall, 1548 HIV-positive individuals were asked about their smoking status over a 12-month period. Of this group, 385 (25%) reported that they were current smokers, 372 (97%) were offered referral to smoking cessation services and 154 (40%) accepted this. We established an outcome of referral for 114 (74%) individuals. A total of 36 (10% of smokers) attended stop smoking clinics and 16 (4%) individuals were recorded as having quit smoking.
Discussion The simple intervention of asking PLWH about tobacco smoking and offering referral to smoking cessation services rapidly identified current smokers, 40% of whom accepted referral to smoking cessation services. This highlights the importance of promoting behaviour and lifestyle changes with every contact with health services. However, a large proportion of those referred were either not seen in local services or the outcome of referral could not be ascertained. If the risk of smoking-related morbidity among PLWH is to be reduced, more sustainable referral pathways and ways of improving uptake of smoking cessation services must be developed.
- Tobacco and the lung
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
People living with HIV are more likely to smoke than the general population and are at greater risk of harm caused by smoking; interventions are required to improve smoking cessation in this group.
A simple intervention of asking about smoking and offering referral for smoking cessation was feasible and resulted in a significant uptake of referral; however, a large proportion of those referred did not attend, suggesting that ways of improving uptake of smoking cessation services for HIV-positive people are required.
This article describes a simple intervention that was associated with increased numbers of smokers identified within an HIV service and an increased number of referrals to smoking cessation services compared with the time period before the intervention.
Background
Tobacco smoking represents the most important cause of avoidable premature death worldwide.1 Among people living with HIV (PLWH) with good access to antiretroviral therapy (ART), smoking is now estimated to be responsible for the loss of more life-years than HIV infection itself.2 PLWH in most resource-rich settings are more likely to smoke than the general population,3 4 and may be at greater risk of smoking-related comorbidities, such as cardiovascular and respiratory disease,5 6 and some cancers.7 In the UK, while smoking rates have fallen in the general population, this trend may be less apparent among PLWH,8 for instance, the multisite Antiretrovirals, Sexual Transmission Risk and Attitudes study (which included evaluation of smoking attitudes and behaviours) found that 29% of PLWH were current smokers compared with 19% of the general population.3 There is, therefore, an urgent need to address the high prevalence of tobacco smoking among HIV-positive people and develop cost-effective services to meet this healthcare need.
Smoking cessation interventions have been shown to be cost-effective in many settings.9 These include the provision of very brief advice (VBA) by healthcare workers (a brief structured intervention consisting of assessing smoking behaviours and providing advice and specific recommendations to support smoking cessation), nicotine replacement therapy, prescription of bupropion or varenicline and use of stop smoking clinics.10 To date, few studies have assessed these interventions in the context of HIV care services and none have done so in the UK.11 We sought to evaluate the impact of asking healthcare workers to systematically identify current smokers attending routine HIV ambulatory care appointments and provide VBA.
Methods
We conducted an observational study in an adult HIV care service (Royal Free London NHS Foundation Trust) between October 2014 and October 2015. Healthcare assistants (HCAs) and nursing staff were provided with training regarding the provision of VBA and given details of smoking cessation services prior to the start of the intervention. Training was provided by the hospital in-house specialist stop smoking advisers and the National Centre for Smoking Cessation and Training website.12
HIV-positive individuals attending routine HIV ambulatory care appointments were asked about smoking status by HCAs and nursing staff. This was undertaken when routine observations (blood pressure and weight) were recorded in a cubical allowing patient privacy to be maintained. Patient self-report of whether they considered themselves to be a current smoker was documented; this was not objectively confirmed or more specifically defined. People with a new diagnosis of HIV or those transferring their care from another HIV care provider were specifically evaluated to ascertain whether uptake of stop smoking services in this group differed from the clinic population as a whole.
Individuals who reported that they were current smokers were given VBA and offered referral to smoking cessation services. National Health Service (NHS) stop smoking clinics offer focused support plus provision of nicotine replacement and medications (bupropion or varenicline) where appropriate. In line with national policy, those who accepted this were referred to services in their local area. In-house specialist smoking cessation services were not provided within the HIV care service.
Specific outcomes measured were: (i) the proportion of HIV-positive people reporting current smoking status, (ii) the uptake of smoking cessation referrals and (iii) the outcome of referral to local smoking cessation services.
Data regarding the uptake and outcome of referral to smoking cessation services were obtained by contacting these services directly and by a brief telephone questionnaire to the HIV-positive patients referred to services. The costs and yield in terms of smokers identified and numbers attending smoking cessation achieved by this intervention were estimated.
Data were compiled using Microsoft Excel and statistical analysis was conducted using SPSS V.22 (IBM). To assess differences in the characteristics among HIV-positive people who smoked compared with those who did not, we performed univariable analysis using two-sided χ2 tests for categorical variables and Mann-Whitney tests for continuous variables. All tests of significance used p<0.05 as the threshold of statistical significance.
Patient and public involvement
This study was conducted with the intention of evaluating patient referral to smoking cessation clinics, based on feedback from patients that there was a demand for such a service. There was no formal patient/public involvement in conduct of the study or analysis of the results.
Results
Between October 2014 and October 2015, 1548 HIV-positive patients were asked about their smoking status, representing 47% of the total population served by this HIV clinic. Of these, 385 (25%, 95% CI 23% to 27%) reported being current smokers, 1145 (74%, 95% CI 73% to 76%) being non-smokers and for 18 patients, smoking status was not recorded (figure 1). Patients who smoked were more likely to be male (86% vs 68%, p<0.001), slightly younger (median 48 vs 51 years, p<0.001), more often of White ethnicity (71% vs 51%, p<0.001) and more likely to have acquired HIV through sex between men (66% vs 49%, p<0.001) than non-smokers (table 1). Among those using ART, patients who smoked were more likely to have a detectable HIV viral load than those who did not (11% vs 7%, p=0.03).
Characteristics of smokers and non-smokers

{kind=link}
Flow chart of referrals. NHS, National Health Service.
Of the 385 people identified as current smokers, 372 (97%) were given VBA regarding smoking cessation and offered referral to smoking cessation services. A total of 154 (40%) of the 372 accepted this referral. There were no significant differences in the age, gender, route of transmission, blood CD4 T-cell count or levels of HIV suppression between those who did and did not accept referral to smoking cessation services. Individuals with a new diagnosis of HIV infection and those transferring their care from another HIV service were specifically evaluated; of the 25 individuals in this group who were offered referral to smoking cessation, 10 (44%) accepted this.
To allow for system delays, after a minimum of 3 months from when the referral was sent, we contacted the local smoking cessation clinics to determine the outcome of referrals. We were able to establish this in 114 (74%) of the 154 individuals referred. A total of 36 (32%) were recorded as having attended the smoking cessation clinic and 16 (14%) as having quit smoking; this, therefore, represents 4% of all smokers identified by the intervention. Of the 16 who quit, 10 did so after attending an NHS stop smoking clinic, 2 attended a pharmacy smoking cessation service and 4 quit without any additional specific assistance.
Cost and yield of the intervention
The estimated total cost to HIV care services of providing this additional intervention was estimated to be £2008, based on training three HCAs to deliver VBA, an additional 5 min when taking routine observations to establish and record smoking status and 6 min to deliver VBA for smokers and make referrals to stop smoking services (table 2). Under these conditions, the estimated costs were, therefore, £5.22 for each smoker identified and £55.77 for each individual who attended stop smoking services.
Cost and yield of intervention
Discussion
The harms of smoking and the beneficial effects of smoking cessation on health are well-established. All healthcare staff coming into contact with patients at risk have a role to play in helping smokers to quit, mainly through triggering quit attempts by asking about smoking, delivering VBA on smoking and referring to stop smoking services.
The simple intervention of asking HIV-positive people about smoking when they attended HIV ambulatory care appointments and offering referral to stop smoking services to identified people who were current smokers, allowed VBA advice to be given and 40% of smokers accepted referral to smoking cessation services. This suggests that this intervention was acceptable to people with HIV and there is a demand for such services.
As with other interventions attempting to increase uptake of stop smoking services,13 most individuals offered referral did not take this up. The model of service provision in which dedicated smoking cessation services are not provided within HIV care, but instead individuals are referred to local services or primary care (depending on local commissioning decisions) may represent a barrier to their uptake for PLWH. Specifically targeted interventions in other groups with high smoking prevalence or risk of harm from smoking, such as individuals with peripheral vascular disease,14 diabetes15 or mental health problems,16 have been shown to improve uptake of stop smoking services. We believe that interventions tailored to the needs of PLWH should be evaluated. These might include personalised information about risk of harm from smoking,13 better communication between HIV care and stop smoking services or minimising barriers to access to such services within HIV care.
In the UK NHS setting, smoking cessation services have been shown to be cost-effective.17 The cost associated with the brief intervention we evaluated (estimated to be £55.77 for each person attending stop smoking clinic) was similar to that estimated in an evaluation by Wu et al of a personalised invitation from primary care to stop smoking clinic and appointment for a taster session, with an estimated mean cost of £54 per person. This was found to be cost-effective from an NHS perspective in the long-term.18 Although few studies have comprehensively evaluated the economic impact of smoking cessation across a lifetime, available data suggest that there may be net savings from investing in smoking cessation.19 How this differs in HIV-positive groups in resource-rich settings has not been formally assessed, though the higher prevalence of smoking and greater risk of smoking-related illness is likely to increase these benefits—suggesting that this is a population who should be targeted specifically within smoking cessation policy.
The current means by which smoking cessation interventions are delivered, with few formalised links between HIV and smoking cessation services, may not be suited to the medical, social and psychological needs of PLWH. As a consequence, HIV services could miss this important opportunity to improve health outcomes. Alternative models of care, for instance, facilitating communication between services, training of HIV care providers to deliver smoking cessation assistance or specialist services directly linked to HIV care, should be evaluated. More importantly, asking about smoking and helping smokers to quit must become a core part of the care provided by all healthcare professionals involved with PLWH. Such an approach (described as ‘Making Every Contact Count’) can be a powerful means of generating lifestyle and behaviour change.20
The provision of smoking cessation interventions by the health service in England and Wales has undergone significant changes in recent years: responsibility for preventative public health interventions has moved from healthcare services to local authorities following the Health and Social Care Act 2012. Funding provided to local authorities from central government for public health interventions has subsequently been reduced and smoking cessation services have been one of the targets for cuts.21 At the same time, changes, such as the increased availability of e-cigarettes, have altered the way that some people consume nicotine and may be a means for some individuals to stop smoking, although this remains controversial.22 These changes have been associated with a significant reduction in the number of people accessing NHS stop smoking services.23 Within this changing landscape, HIV services must ensure that appropriate support for their patients is available.
This analysis has limitations which should be considered. Data collection was undertaken as part of clinical service evaluation and for a proportion of referrals made to stop smoking services so we could not establish the outcome of the referral, either because the service had no record of the referral or its outcome, or the smoking cessation service had been decommissioned since the time of referral. This illustrates the current deficiencies in communication between HIV and local smoking cessation services and the reduction in provision of universal smoking cessation services in the UK, as documented by recent national surveys.24 The proportion of HIV-positive individuals identified as current smokers by this intervention (25%) is lower than that found in other recent studies of PLWH in London, where around 30% were current smokers3 8—suggesting that not all smokers disclosed this when asked. Finally, the identification of smokers relied on self-report, rather than being objectively confirmed (for instance with exhaled carbon monoxide measurements) and no objective measurement of quit rates (such as saliva cotinine levels) was performed. Despite these limitations, we believe that our report describing the potential benefit of low-cost smoking cessation interventions for the UK HIV-positive populations and the difficulties highlighted in the management of those smokers who wish to quit highlights the need for joined-up working to improve personal and public health within the NHS.
Footnotes
Contributors JB and ML conceived of the study and led the data analysis. CK, EP, KE and HJ completed data collection. NS, AM, EP and JF collated and analysed data regarding referrals to smoking cessation clinic. AB, JF, AR, ML and JB conducted data analyses. All the authors were involved in the preparation of the manuscript for submission.
Funding This work was partly supported by funding from a Gilead Fellowship Programme grant.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This manuscript describes the results of a quality improvement project undertaken within clinical services for which no additional data were collected beyond that collected for clinical purposes. This, therefore, was exempt from the need for research ethics service approval.
Provenance and peer review Not commissioned; externally peer reviewed.