Article Text

Abstract
Background Haemoglobin vesicles (HbVs) are red blood cell (RBC) substitutes with a phospholipid bilayer membrane and a polyethylene modified surface (diameter=250 nm; P50=28 Torr). They can be preserved for years and can be used in patients of all blood types without the risk of infection. Their oxygen affinity can be modified by changing the allosteric effectors.
Methods Left pneumonectomy was performed under mechanical ventilation on rats, followed by rapid exsanguination of ~30% of the total circulating blood volume. Rat RBCs shed in 5% human serum albumin (HSA) solution (rat RBC), HbV with high oxygen affinity in 5% albumin solution (low-P50 HbV, P50=9 Torr), normal HbV suspended in 5% albumin (HbV, P50=28 Torr) or 5% HSA was infused for resuscitation. Haemodynamics and oxygenation were evaluated.
Results Systemic arterial blood pressure significantly decreased after exsanguination and increased after each infusion. In the HbV, low-P50 HbV and rat RBC groups, all rats were liberated from mechanical ventilation and blood pressure was stabilised, whereas 50% of the rats in the HSA group died within 1 hour after weaning from mechanical ventilation. The PaO2 in arterial blood for 1 hour after liberation from mechanical ventilation in the rat RBC, HbV and low-P50 HbV groups was 59.4±12.5, 58.3±10.1 and 70.5±14.5 mm Hg, respectively. The PaO2 in the low-P50 HbV group was significantly higher than those in the rat RBC and HbV groups (p=0.05 for both). Serum lactate elevations due to hypoxic damage were minimised by HbV, low-P50 HbV as well as rat RBCs.
Conclusions The oxygen-carrying ability of HbV was comparable to that of rat RBCs, even under impaired lung function after pneumonectomy. HbVs with high oxygen affinity may have more beneficial effects on oxygenation in pulmonary resection.
- thoracic surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Can haemoglobin vesicles (HbVs) be used as a substitute for the perioperative transfusion of red blood cells (RBCs) in thoracic surgery, when or where donated RBCs are not immediately available?
HbVs, which are liposomes-containing concentrated haemoglobin, were developed as artificial oxygen carriers that serve as an alternative to transfusion.
The infusion of HbVs suspended in serum albumin could compensate for rapid ~30% blood loss in pneumonectomised rats with severely impaired lung functions.
Introduction
Lung cancer is a highly lethal disease in many countries.1 2 Surgery offers the best chances for cure in patients with early stage non-small cell lung cancer.3 Advances in surgical technology and anaesthesia techniques have enabled lung resection to be performed safely. However, the risks of massive surgical haemorrhage remain unchanged because pulmonary vessels are fragile, and malignant tumours may invade these vessels. McKenna et al reported that blood transfusion was required in 45 of 1100 patients (4.1%) who underwent thoracic lobectomy.4
Haemoglobin vesicles (HbVs), which are liposomes-containing concentrated haemoglobin, were developed as artificial oxygen carriers that serve as an alternative to transfusion. Haemoglobin is extracted from outdated human red blood cells (RBCs) for transfusion, purified and virus-inactivated and then encapsulated in liposomes5 with a polyethylene modified surface (diameter=250 nm; P50=28 Torr). HbVs can be preserved for years and used irrespective of the blood type and are free from the risk of infection.6 They are expected to show various clinical applications, including management of surgical haemorrhage, in the near future, although all trials for the clinical application of other artificial oxygen carriers developed as substitutes for RBC transfusion have ended in failure due to side effects or a lack of effectiveness.
A notable characteristic of HbV is that its oxygen affinity can be modified by changing the allosteric effectors encapsulated with the purified haemoglobin in the vesicles.7 The oxygen affinity of normal HbVs is set at a P50 level of 28 Torr, and that of HbVs with high oxygen affinity is set at a P50 level of 9 Torr (low-P50 HbVs). In previous investigations on tumour oxygenation, low-P50 HbVs increased tissue partial oxygen pressure and facilitated the effects of irradiation on tumours.8
We expect low-P50 HbVs to help improve oxygen intake at the lung and carry more oxygen into organ tissues in animals that undergo lung resection. These effects may facilitate rapid stabilisation of haemodynamics and oxygenation in cases showing massive surgical haemorrhage during lung resection, which can cause remarkable reductions in pulmonary function. In the present study, the immediate effects of systemic administration of HbVs or low-P50 HbVs were evaluated after massive blood exsanguination in a rat pneumonectomy model.
Materials and methods
The investigation conformed to The Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 85–23, revised 1996).
Preparation of HbVs
HbVs were prepared in sterile conditions at Nara Medical University, as previously described.9 10 Haemoglobin was purified from outdated donated blood provided by the Japanese Red Cross Society (Tokyo, Japan). The encapsulated haemoglobin (380 g/L) contained 14.7 mmol/L of pyridoxal 5′-phosphate (PLP) as an allosteric effector at an Hb/PLP molar ratio of 2.5. The lipid bilayer was composed of a mixture of 1,2-dipalmitoyl-sn-glycero-3-phosphatidylcholine, cholesterol and 1,5-bis-O-hexadecyl-N-succinyl-L-glutaminate at a molar ratio of 5/5/1 and 1,2-distearoyl-sn-glycero-3-phosphatidylethanolamine-N-poly(ethylene glycol). HbV was suspended in saline at an Hb concentration of 100 g/L. The physicochemical parameters of the HbVs were as follows: particle diameter 251±80 nm; methemoglobin concentration <2% and oxygen affinity (P50) 28 Torr.
Preparation of low-P50 HbVs
HbVs with a P50 of approximately 9 Torr (low-P50 HbVs) were prepared using the same protocol except that pyridoxal 5′-phosphate was not added.7 The P50 and Hill numbers of each HbV solution were calculated from the oxygen dissociation curves measured using a Hemox Analyzer (TCS-Medical Products, Huntington Valley, Pennsylvania, USA). Particle diameter was controlled to 250±64 nm. Vesicle properties were considered to be equivalent to those of normal HbVs, except for the P50. Detailed characteristics of the HbVs with different oxygen affinities have been described by previously published literature.11
Preparation of washed rat RBCs suspended in HSA
Rat RBCs suspended in HSA were used as a reference to compare the effectiveness of HbVs and low-P50 HbVs, and to demonstrate the influence of the exchange transfusion procedure. Wistar rats were anaesthetised with subcutaneous injections of 100 mg/kg of ketamine and 10 mg/kg of xylazine. A polyethylene catheter (PE-31) was implanted in the carotid artery, and blood was withdrawn with heparinised syringes, while 8 g/dL HSA solution was infused alternately by exchange transfusion. The collected blood was centrifuged to obtain an RBC concentrate. This concentrate was washed twice to remove plasma components and the buffy coat by redispersion in HSA and centrifugation at 3000 g for 3.5 min. The Hb concentration was adjusted to 86 g/L, which was equivalent to the concentration of HbV and low-P50 HbV.
Animal preparation
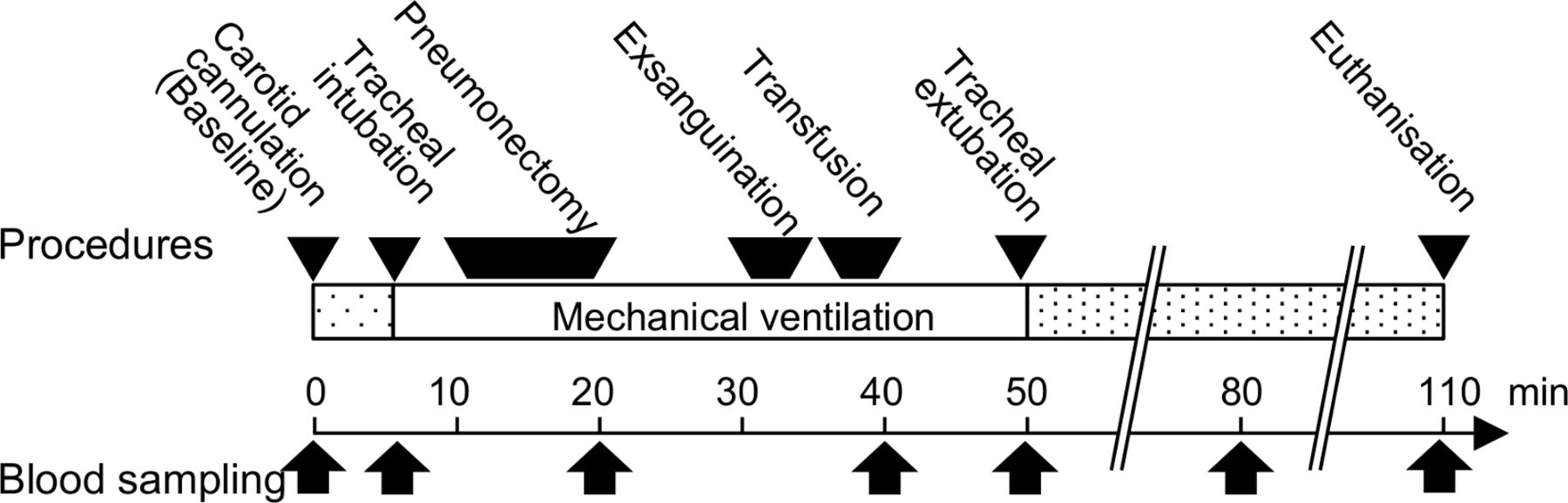
Specific, pathogen-free, inbred male Wistar rats aged 8 weeks and weighing between 250 and 350 g were purchased from CLEA Japan Tokyo, Japan. The rats were kept on a 12 hours light/dark cycle with free access to food and water. The schematised experimental protocol is shown in figure 1A.
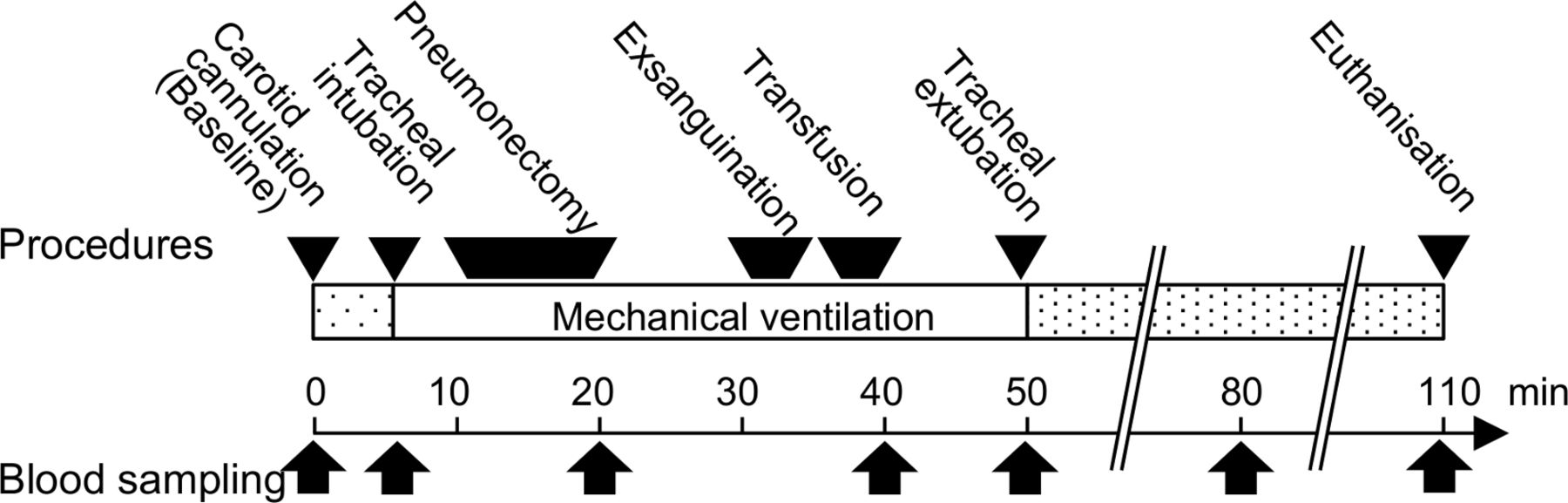
Schematised representation of the time course of interventions and blood samplings in the present protocol.
Continuous monitoring of mean arterial blood pressure
The rats were anaesthetised with a subcutaneous injection of 100 mg/kg of ketamine and 10 mg/kg of xylazine and placed on a heating pad. After an incision was made in the neck, a heparinised polyethylene catheter (SP-31 tubing; outer diameter=0.8 mm; inner diameter=0.2 mm) was introduced into the right carotid artery. Blood samples were withdrawn to obtain baseline values of blood count, blood gas analysis and lactate level. The arterial catheter was connected to a blood pressure measurement system (KN-213/KN-212; Natsume Seisakusho, Tokyo, Japan) for continuous recording of the mean arterial pressure (MAP). Another catheter (SP-31) was inserted into the right internal jugular vein for sample infusion.
Surgical procedures for left pneumonectomy
The rats were orotracheally intubated with a 14 G catheter and connected to a rodent ventilator (model SN-480-7; Shinano, Tokyo, Japan) adjusted to maintain a respiratory rate of 60 breath/min, tidal volume of 10 mL/kg, positive end-expiratory pressure of 2 cmH2O and inspired O2 concentration of 0.21. Blood samples were obtained to determine the values on mechanical ventilation. A postero-lateral incision was made, followed by a thoracotomy at the fifth intercostal space. The hilum was ligated with a 3–0 silk suture, and the lung was removed. The fifth intercostal space was closed with a single surgical suture, and the skin and muscle incisions were closed with four loose sutures. The operation was performed using a sterile technique. After removal of the left lung, the tidal volume was reduced to 8 mL/kg to avoid ventilator-induced lung injury.12 13 The duration of all surgical procedures was set at 10 min in all experimental groups. Blood samples were obtained to determine the values after pneumonectomy.
Rapid exsanguination and isovolemic transfusion
We set the volume of exsanguination at 30%, because a 30% blood loss in rats is equivalent to 2000 mL of blood loss and haemoglobin levels <80 g/L in patients with an average body weight, which is considered to be a trigger for blood transfusion in clinical settings. After pneumonectomy and stabilisation of the animal’s condition, 30% of the estimated total circulating blood volume of the rat was rapidly withdrawn via a carotid artery. Since the systemic blood volume was estimated to be 56 mL/kg body weight, as reported in a previous rat experiment,14 the calculated 30% of total blood volume was 16.8 mL/kg. The rats were then infused with an isovolemic volume of 5% human serum albumin solution (HSA, n=8), rat red blood cells shed in 5% albumin (rat RBC, n=5), HbV suspended in 5% albumin (HbV, P50=28 Torr, n=5) or HbV with high oxygen infinity in 5% albumin (low-P50 HbV, P50=9 Torr, n=8) via an internal jugular vein at the speed of 1 mL/min. Haemoglobin and albumin concentrations were adjusted to 86 g/L and 5 g/dL, respectively in the rat RBC, HbV and low-P50 HbV groups.15 Blood samples were obtained to determine the values after infusion.
Monitoring survival after weaning from mechanical ventilation
After haemodynamic stabilisation and a trial of spontaneous breathing, the rats were extubated. To minimise pain and distress, carprofen was administered subcutaneously at a dose of 5 mg/kg body weight. When severe respiratory distress was observed, the animals were euthanised by exsanguination via the caudal vena cava under deep anaesthesia with subcutaneous injection of ketamine (100 mg/kg) and xylazine (10 mg/kg) as a humane end point. The animals’ survival was monitored and the effects of HbV on survival were measured, and MAPs were recorded until 1 hour after weaning from mechanical ventilation. Blood samples were taken via the carotid arterial line to obtain the values 30 and 60 min after tracheal extubation. Thereafter, all the rats were euthanised with injections of ketamine (100 mg/kg) and xylazine (10 mg/kg), and blood was drawn from the caudal vena cava.
Arterial blood gas and haematology analysis
Arterial blood samples of approximately 200 µL taken after each procedure or at time points after tracheal extubation were used for haematological analysis, blood gas analysis and lactate measurements. The i-STAT 1 portable analyser (Abbott Point of Care, Princeton, New Jersey, USA) and the test cartridges (CG4+; Abbott Point of Care) were used with 100 µL samples for gas analysis and lactate measurements, while 50 µL of each blood sample was analysed using the pocH-100iV Diff haematology analyser (Sysmex). Haematocrit was measured with glass capillaries.
Organ tissue oxygen tension measurement
The tissue oxygen tension was measured in the cortex of the kidney after each procedure and at the 30 and 60 min time points after tracheal extubation (n=3 for each group). After induction of anaesthesia and cannulation into a carotid artery and a jugular vein, the abdomen was opened and the kidney was exposed. Left pneumonectomy along with exsanguination and infusion were performed as described above in the sections of Surgical procedures for left pneumonectomy and Rapid exsanguination and isovolemic transfusion. The needle probe was inserted into the cortex of the kidney and connected to the dissolved oxygen (dO2) monitoring device, isoPod (EP354; eDAQ, Australia) and the e-corder Systems (ED410; eDAQ) for each measurement. Stable values obtained dozens of seconds after probe insertion were employed in further analyses.
Calculation of oxygen arterial content
Oxygen arterial content (CaO2) was calculated by the following equation:

Statistical analysis
The data are presented as means±SD. Measurements of haematocrit and haemoglobin levels are presented as it is, whereas the haemodynamic values, blood gas analysis data, calculated CaO2 values and serum lactate levels are shown as a percentage of the basal values or as differences from the basal values. Between-group differences at points after the interventions were examined by Bonferroni/Dunn tests. Longitudinal data obtained at three time points after weaning from mechanical ventilation were compared by repeated-measures analysis of variance. When significant differences were detected, post hoc analyses were performed using Bonferroni’s corrections. A p value <0.05 was considered to be statistically significant. The data were analysed with StatView-J software, V.5.0 (Abacus Concepts, Berkeley, California, USA).
Patient and public involvement
This research was carried out without involving any patients. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
Basal values
Values for all the measurements at baseline collected after anaesthesia are shown in table 1. No significant intergroup differences were detected for any of the measurements.
Basal values for haemodynamic and blood sample parameters
Survival after pneumonectomy and ~30% blood exchange
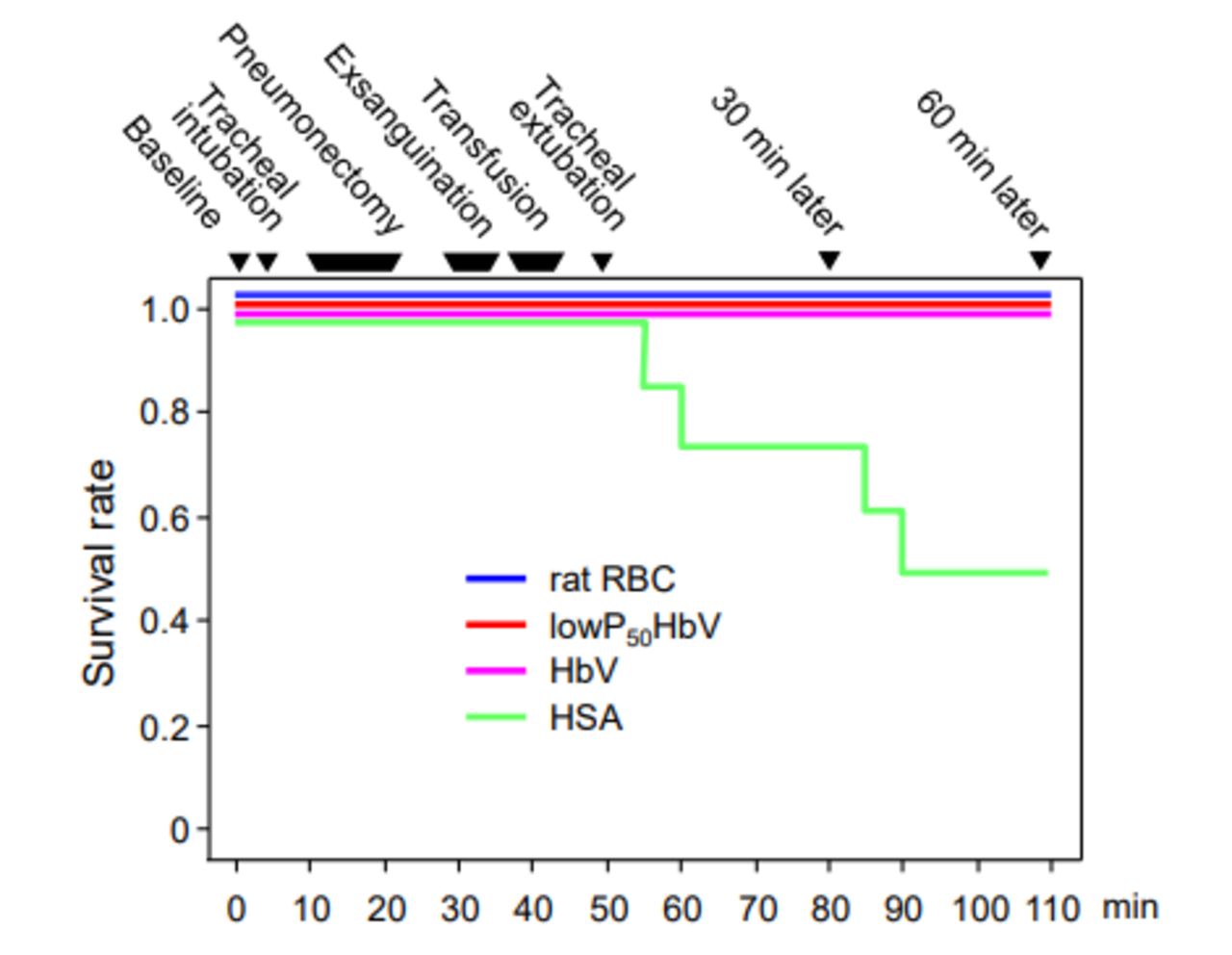
All rats that underwent left pneumonectomy followed by ~30% blood exchange in the rat RBC (n=5), low-P50 HbV (n=8) and HbV (n=5) groups survived for 1 hour after weaning from mechanical ventilation. In contrast, in the HSA group (n=8), four of the eight rats died within 1 hour (figure 2). The measurements in the HSA group that are described below in the figures 3–7 were obtained from the rats that survived after tracheal extubation.
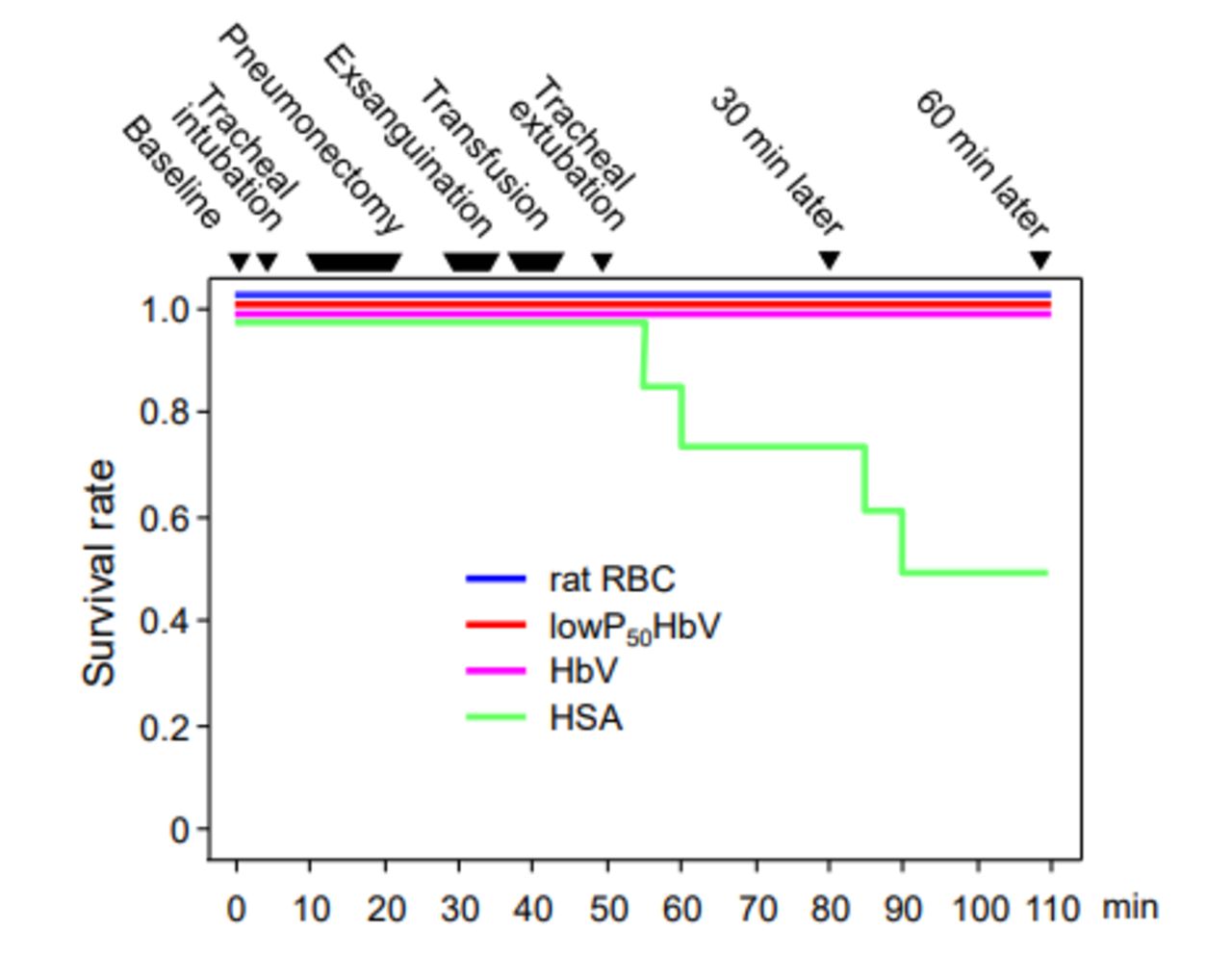
Survival curve after left pneumonectomy, exsanguination of 30% of circulating blood and isovolemic transfusion using rat red blood cells (rat RBC, blue, n=5), haemoglobin vesicles with high oxygen affinity (low-P50 HbV, P50=9 Torr, red, n=8), haemoglobin vesicles (HbV, P50=28 Torr, pink, n=5) or human serum albumin (HSA, green, n=8).

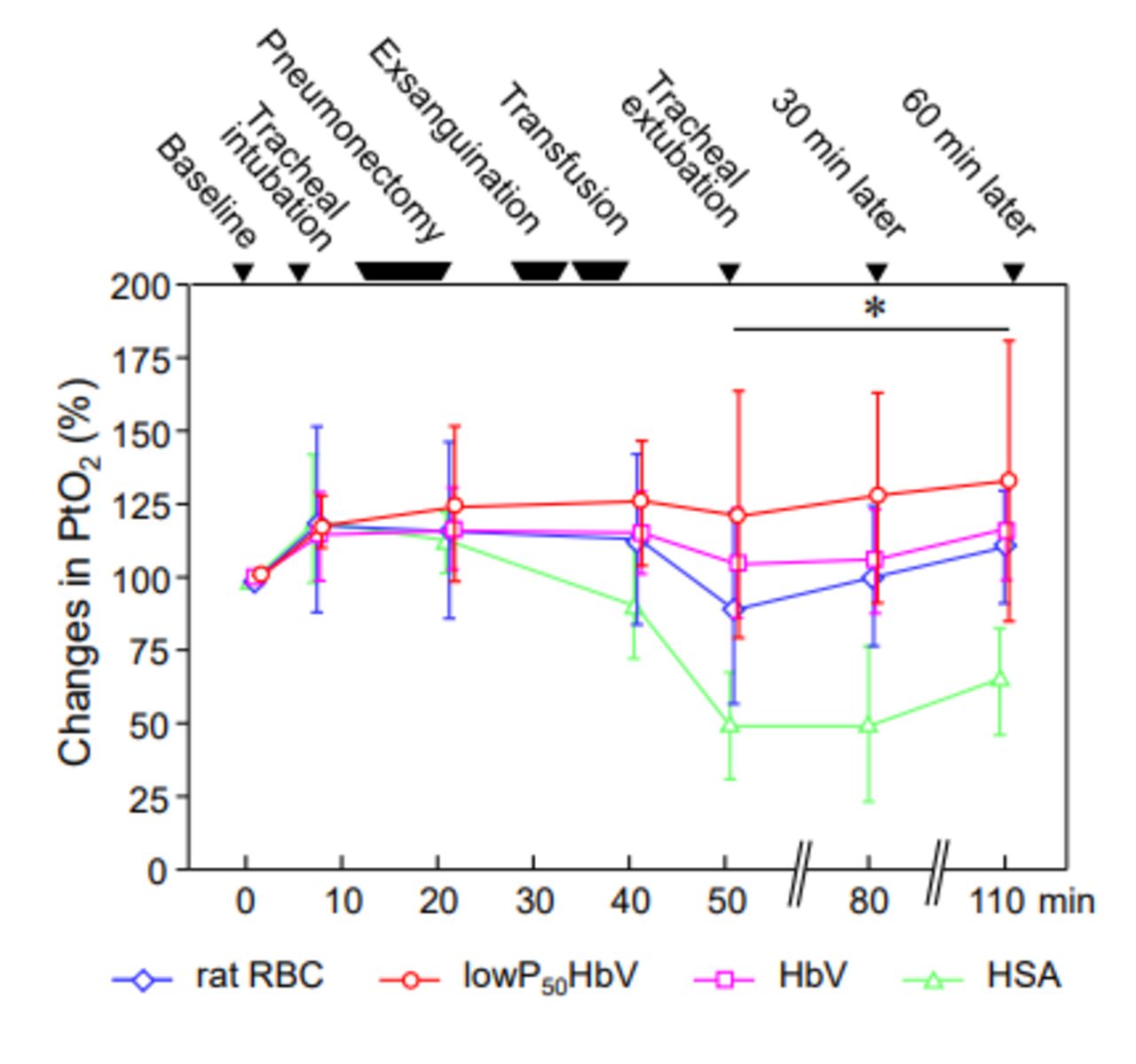
Changes in tissue oxygen pressure (PtO2) of the renal cortex (A) and skeletal muscle (B) after each procedure are shown as percentages of the basal values. Rat red blood cell (rat RBC) group (n=5); haemoglobin vesicle with high oxygen affinity (low-P50 HbV) group (n=8); haemoglobin vesicle (HbV) group (n=5); human serum albumin (HSA) group (n=5). Values are means±SD. *P<0.05, low-P50 HbV vs rat RBC; #p<0.0001, HSA vs rat RBC and HbV, repeated-measures analysis of variance.
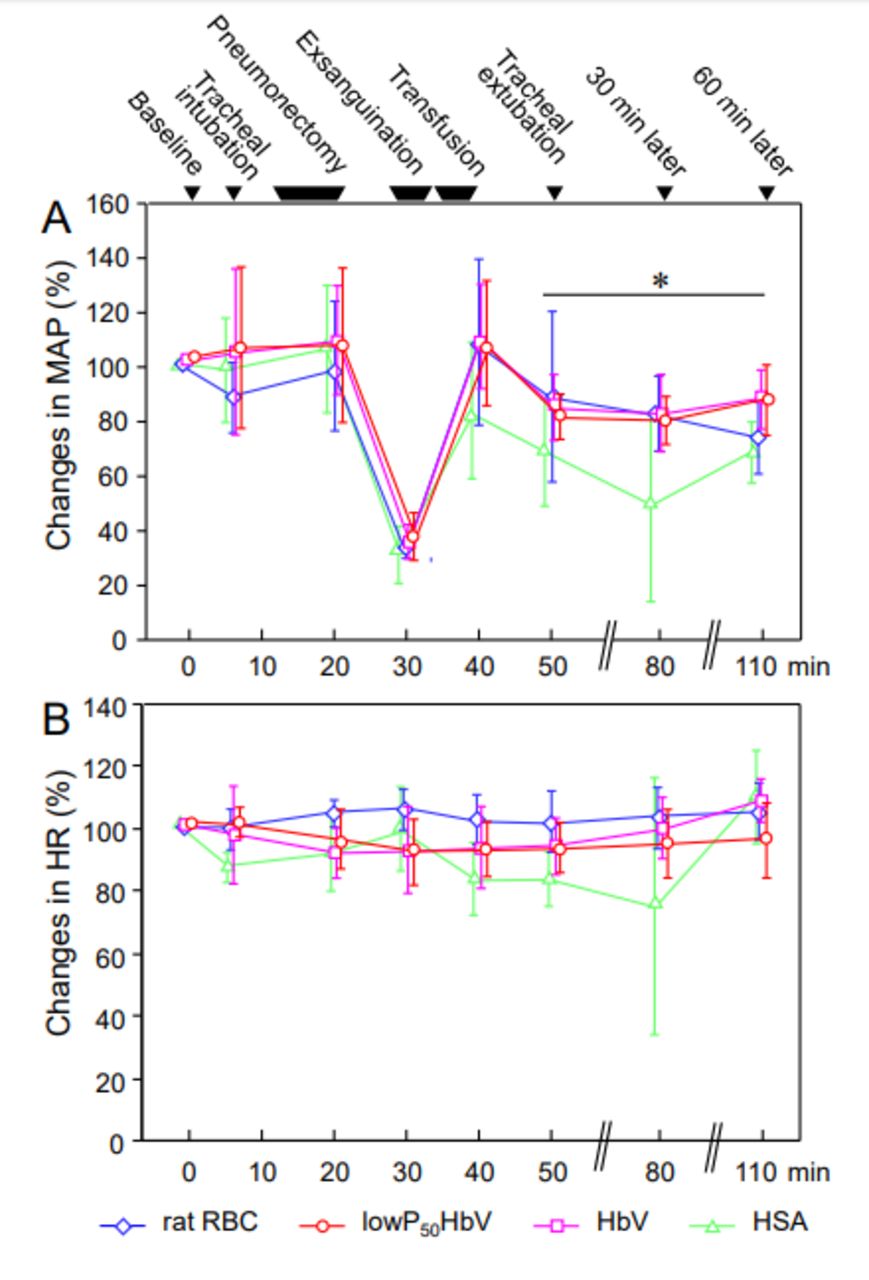
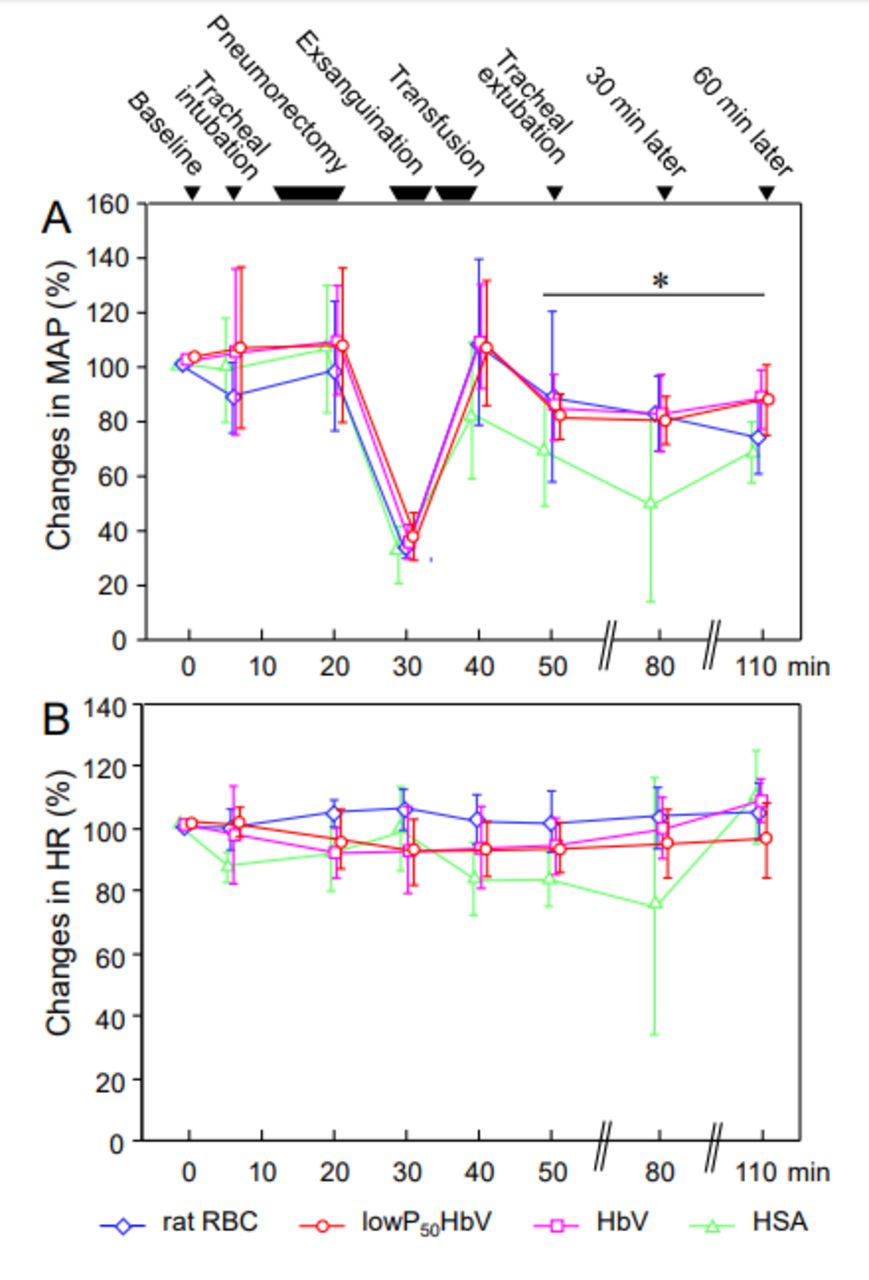
Changes in mean arterial blood pressure (MAP) (A) and heart rate (HR) (B) during the course of left pneumonectomy, 30% exsanguination and transfusion and weaning from the mechanical ventilation are shown as percentages of the basal values based on the transfusion substitute, namely, rat red blood cells (rat RBCs, n=5), haemoglobin vesicles with high oxygen affinity (low-P50 HbV, P50=9 Torr, n=8), haemoglobin vesicles (HbV, P50=28 Torr, n=5) or human serum albumin (HSA, n=4~8). Values are means±SD. *P<0.05, HSA vs all other groups, compared by repeated-measures analysis of variance.
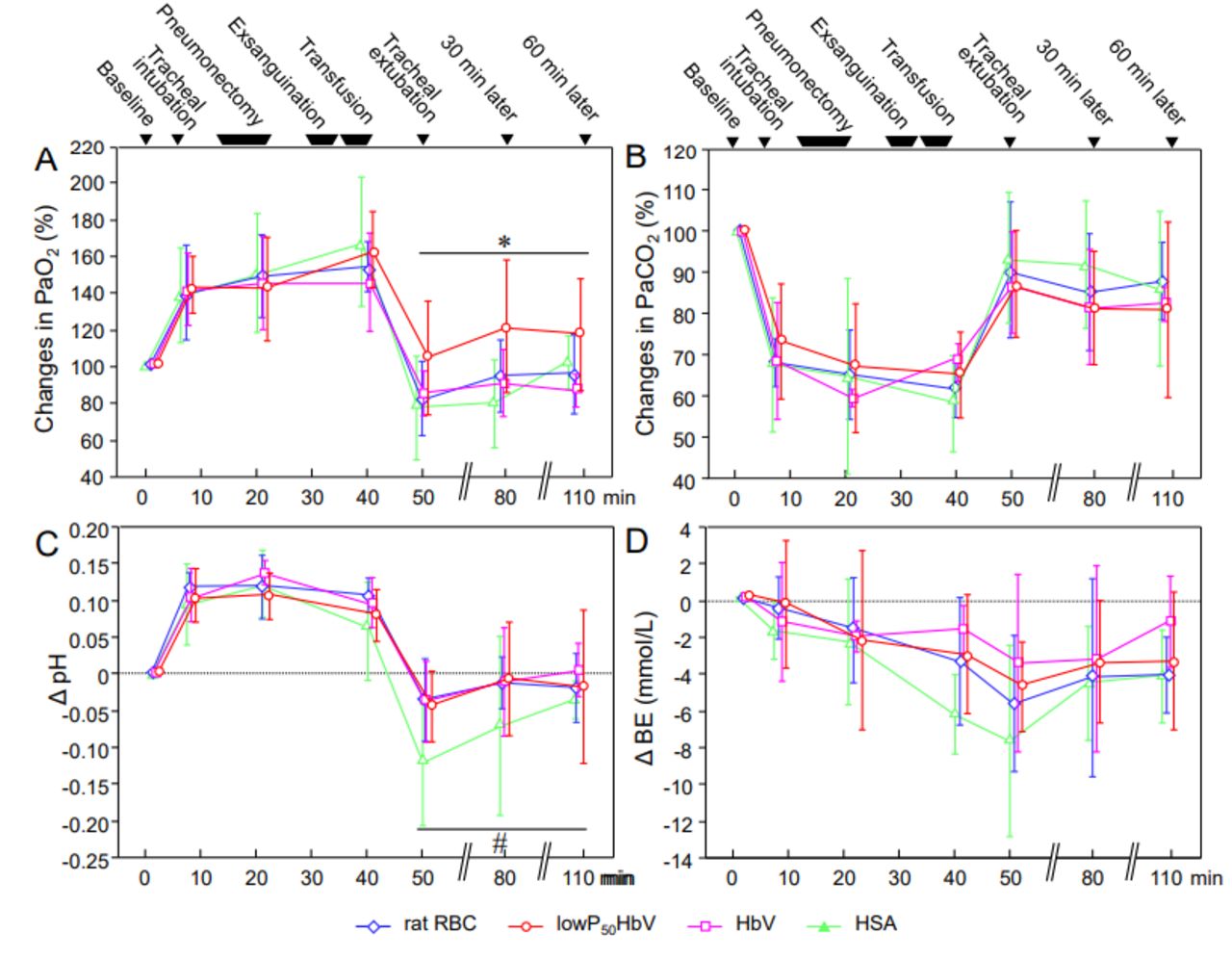
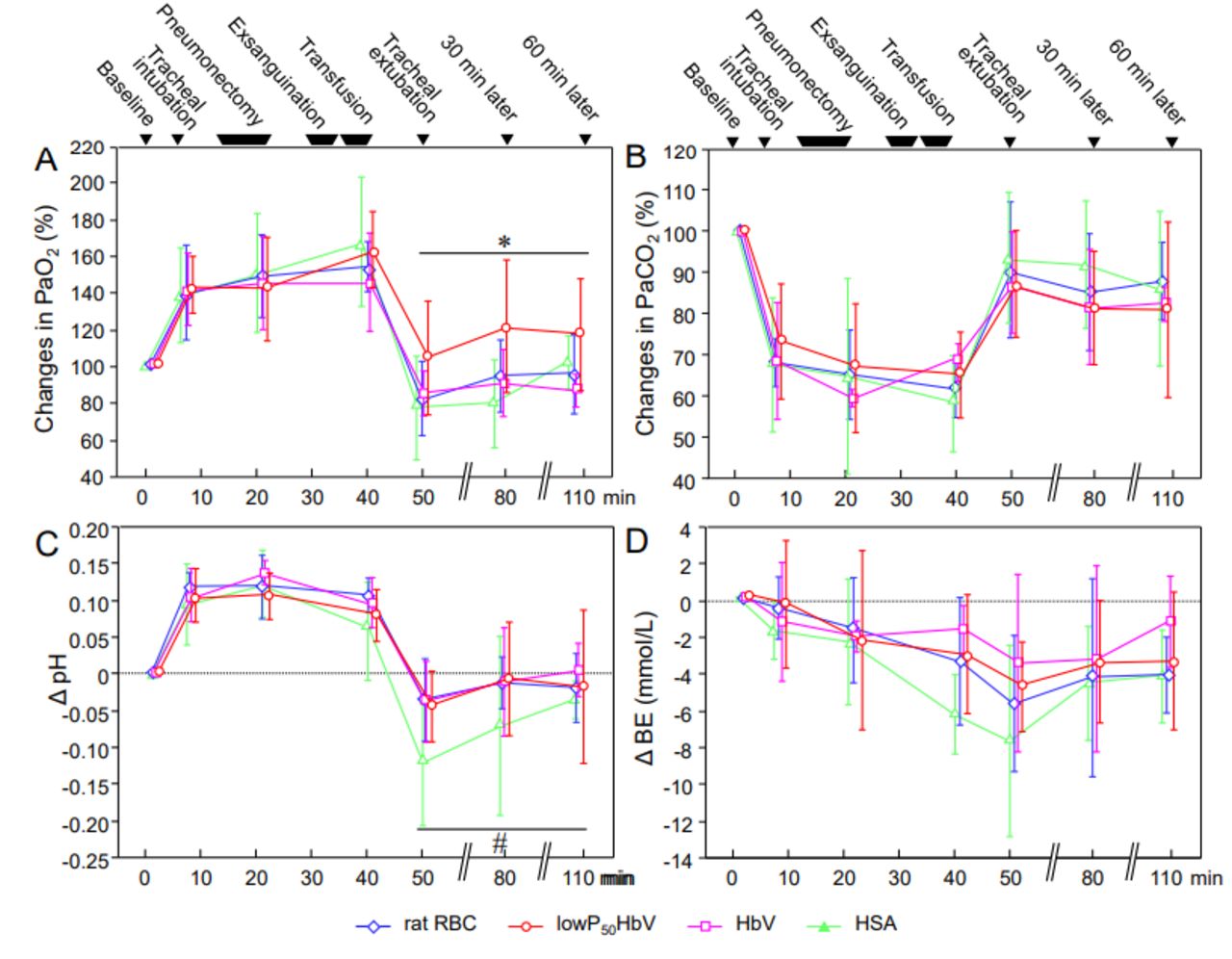
Changes in PaO2 (A) and partial pressure of arterial carbon dioxide (PaCO2) (B) after each procedure shown as percentages of the basal values. The pH (C) and base excess (BE) (D) after each procedure are shown as differences from the basal values. Rat red blood cell (rat RBC) group (n=5); haemoglobin vesicle with high oxygen affinity (low-P50 HbV) group (n=8); haemoglobin vesicle (HbV) group (n=5) and human serum albumin (HSA) group (n=4~8). Values are means±SD. *P<0.05, low-P50 HbV vs the other groups; #p<0.05, HSA vs the other groups, compared by repeated-measures analysis of variance.

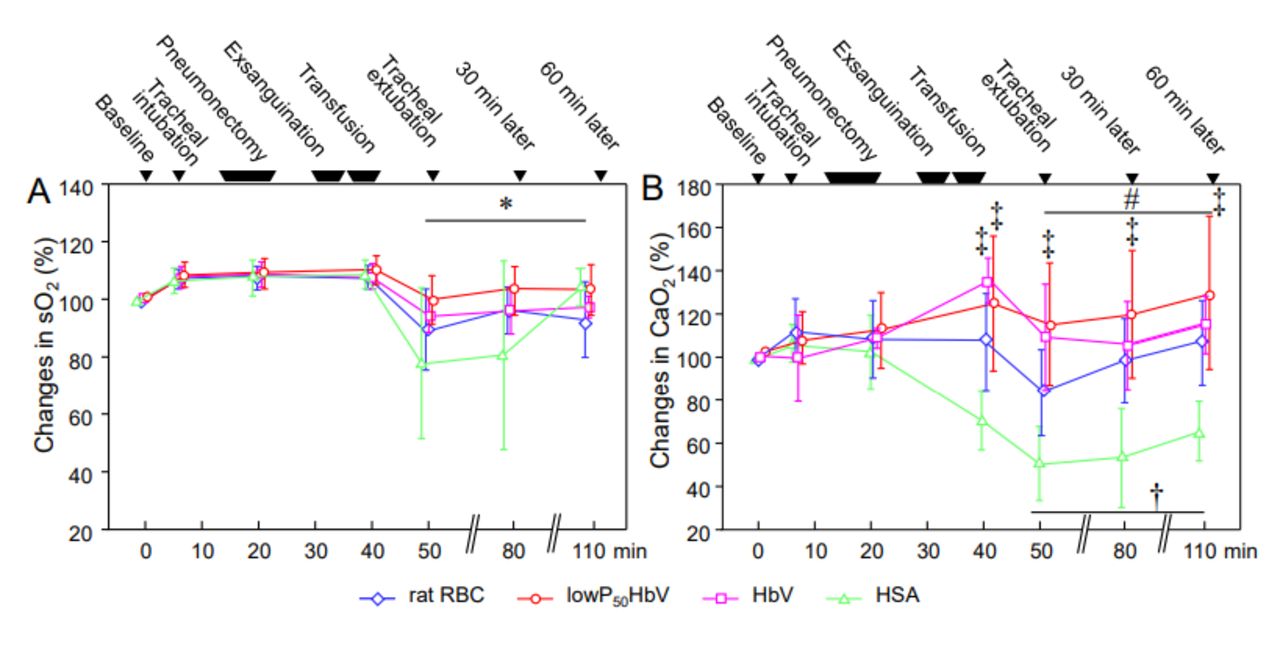
Changes in arterial oxygen saturation (sO2) (A) and arterial oxygen content (CaO2) (B) after each procedure are shown as percentages of the basal values. Rat red blood cell (rat RBC) group (n=5); haemoglobin vesicle with high oxygen affinity (low-P50 HbV) group (n=8); haemoglobin vesicle (HbV) group (n=5) and human serum albumin (HSA) group (n=4~8). Values are means±SD. *P<0.05, low-P50 HbV vs the other groups, repeated-measures analysis of variance. #P<0.05, low-P50 HbV vs rat RBC and HSA groups, repeated-measures analysis of variance. †P<0.05, rat RBC and HbV vs HSA groups, repeated-measures analysis of variance. ‡P<0.05 vs HSA, Bonferroni/Dunn test.
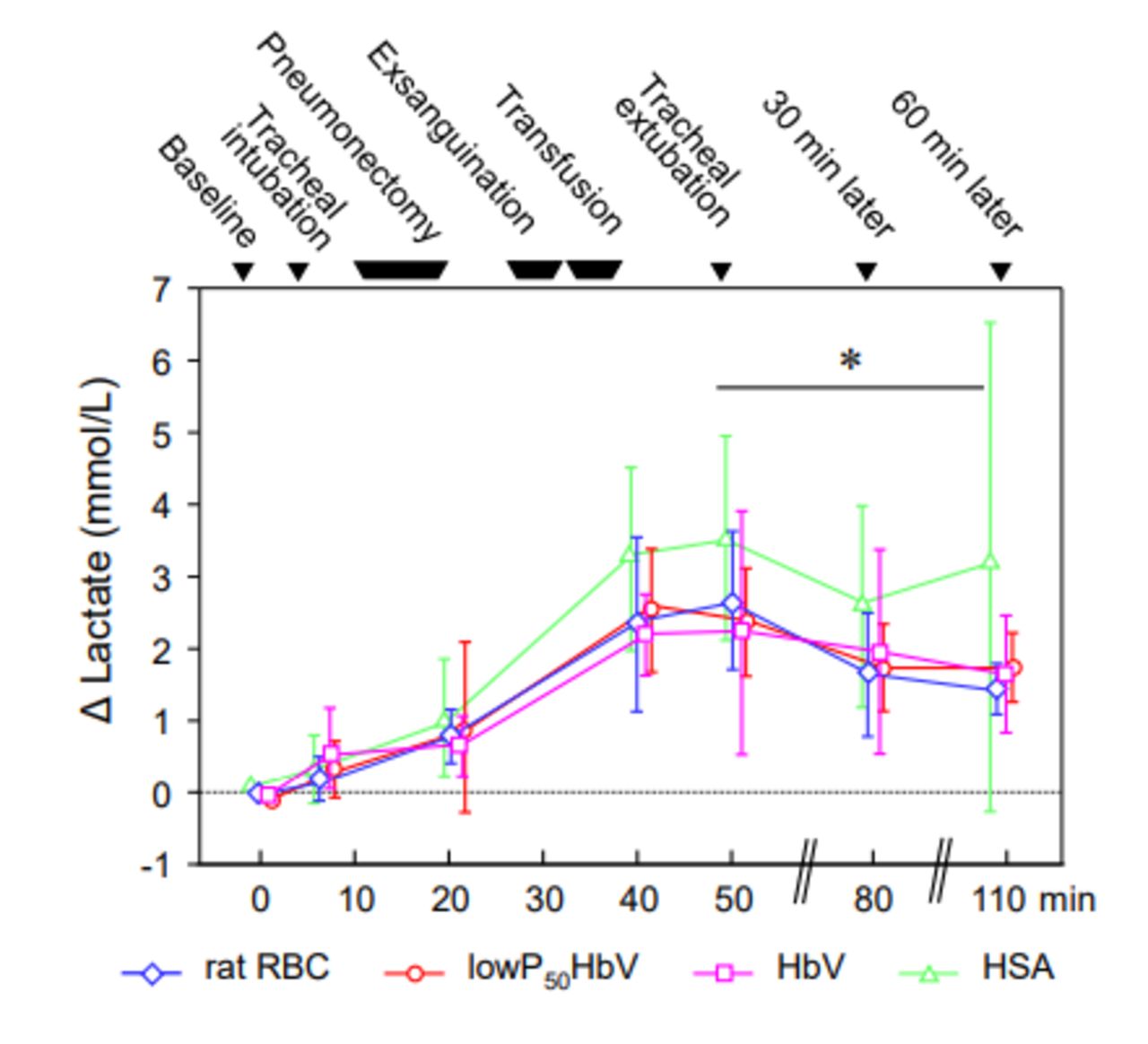
Changes in serum lactate levels. Serum lactate levels after each procedure are shown as differences from the basal values. Rat red blood cell (rat RBC) group (n=5); haemoglobin vesicle with high oxygen affinity (low-P50 HbV) group (n=8); haemoglobin vesicle (HbV) group (n=5); human serum albumin (HSA) group (n=4~8). Values are means±SD. *P<0.05, low-P50 HbV vs HSA group, repeated-measures analysis of variance.
Changes in haematocrit and haemoglobin levels
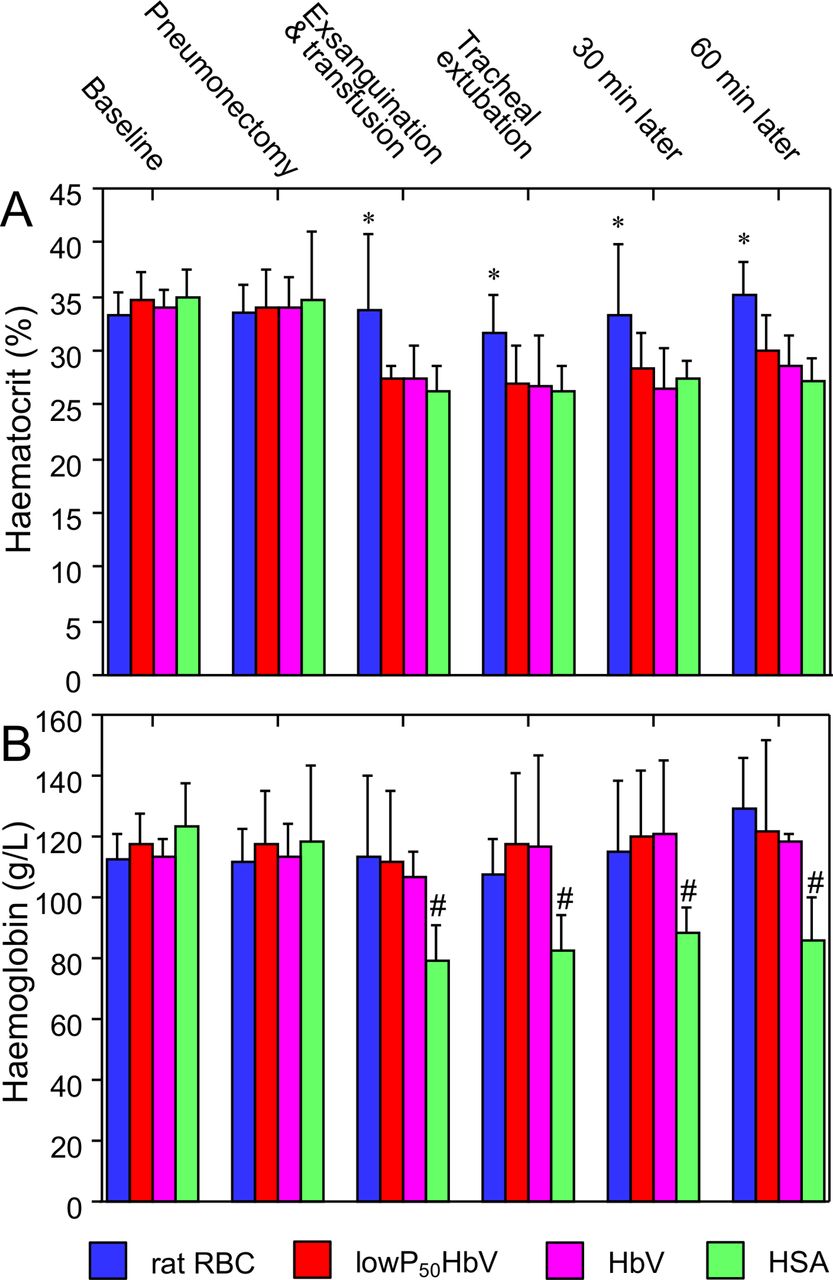
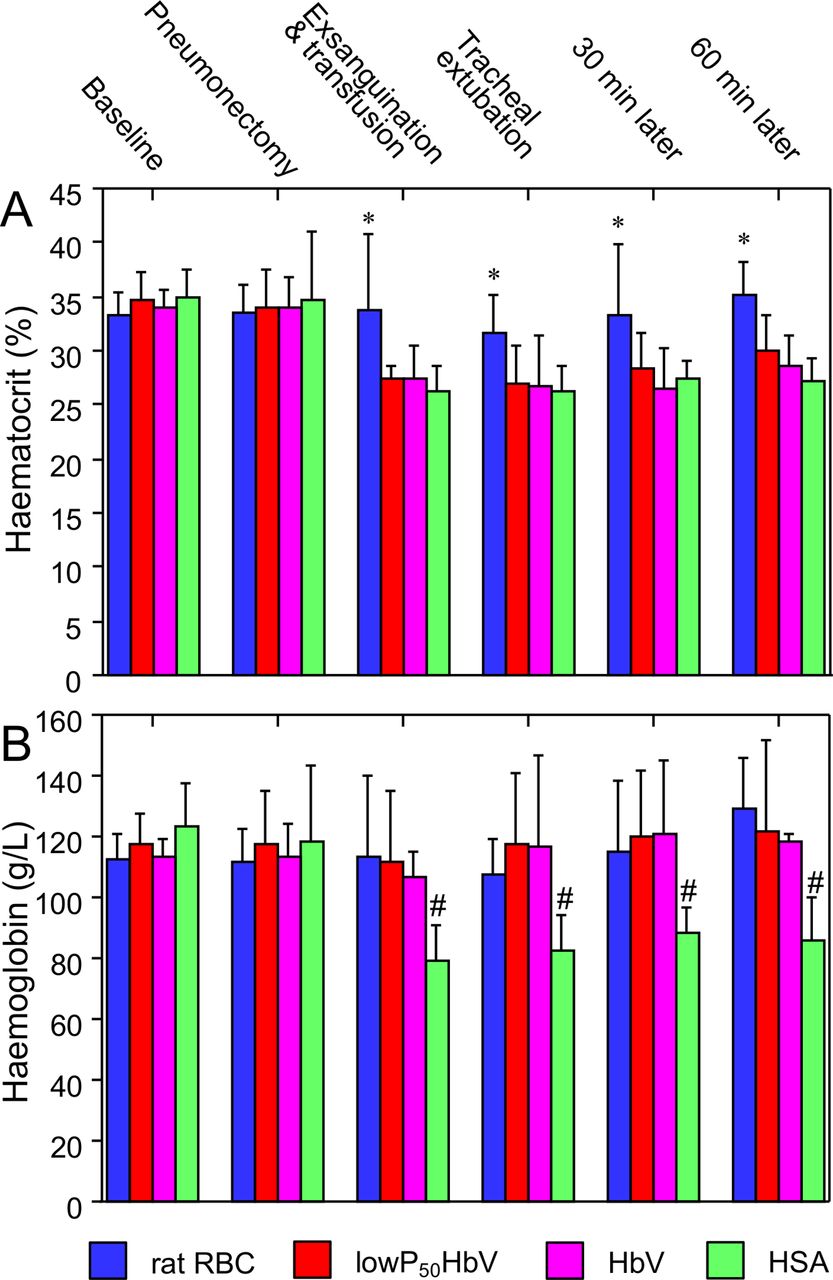
Haematocrit and haemoglobin levels after each surgical procedure are shown in figure 8. At the completion of pneumonectomy and ~30% exsanguination and isovolemic transfusion, the ratio of haematocrit values to the basal values decreased to 71.9%±7.1% in the HSA group, whereas the ratio was 95.5%±13.6% in the rat RBC group. Since HbVs are not precipitated by conventional centrifugation, the haematocrit ratios were 72.3%±9.3% in the low-P50 HbV group and 71.4%±13.9% in the HbV group. Differences in haematocrit ratios between the rat RBC group and the other three groups after the exsanguination and transfusion were significant (p<0.01, each). These values showed that ~30% of the circulating blood was actually replaced by exsanguination and transfusion. On the other hand, the corresponding ratios for the haemoglobin levels were 98.6%±17.5% in the rat RBC group, 94.4%±18.8% in the low-P50 HbV group, 95.3%±12.4% in the HbV group and 68.7%±9.3% in the HSA group. Thus, the haemoglobin encapsulated in HbVs showed similar measurements as that in RBCs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in haematocrit (A) and haemoglobin (B) levels during the course of the pneumonectomy followed by exsanguination of 30% circulation blood volume and isovolemic transfusion with rat red blood cell (rat RBC, n=5), haemoglobin vesicles with high oxygen affinity (low-P50 HbV, P50=9 Torr, n=8), haemoglobin vesicles (HbV, P50=28 Torr, n=5) or human serum albumin (HSA, n=4~8). Values are means±SD. *P<0.01 vs all other groups; #p<0.05 vs all other groups, Bonferroni/Dunn test.
Changes in mean arterial pressure and heart rate
The changes in MAP and heart rate (HR) are presented as percentages of the basal values (figure 3). Rapid exsanguination of 30% of the circulating blood volume caused shock with an approximately ~70% decrease in MAP. The MAP was elevated by each isovolemic infusion. In the rats infused with rat RBCs, HbV or low-P50 HbV, the MAP was maintained for 1 hour after cessation of mechanical ventilation. However, in the HSA group, the MAP decreased in some rats who could not maintain spontaneous respiration, and half of the rats died within 60 min (figure 3A). There were significant differences in longitudinal MAP measurements after liberation from mechanical ventilation between the HSA and the other three groups (HSA vs rat RBC, p<0.05; HSA vs low-P50 HbV, p<0.005; HSA vs HbV, p<0.01; repeated-measures analysis of variance). HR was stable throughout the experimental period in the rat RBC, low-P50 HbV and HbV groups. In contrast, in the HSA group, HR decreased, especially in the rats showing decompensation, and the SD of the HR values increased (figure 3B).
Changes in the PaO2
The changes in PaO2 are shown as percentages of the basal values according to the transfusion substitutes at each procedure and time point (figure 4A). There were no significant intergroup differences at any time point. However, there was a significant difference in longitudinal PaO2 measurements after liberation from mechanical ventilation between the low-P50 HbV and the other three groups (low-P50 HbV vs rat RBC, p<0.05; low-P50 HbV vs HbV, p<0.01 and low=P50 HbV vs HSA, p<0.005, repeated-measure analysis of variance).
Changes in the partial pressure of arterial carbon dioxide
The changes in PaCO2 are shown as percentages of the basal values according the transfusion substitutes at each time point (figure 4B). There were no significant intergroup differences at any of the time points. Moreover, there were no significant intergroup differences in longitudinal PaCO2 measurements after liberation from mechanical ventilation.
Changes in pH
The changes in pH are shown as differences from the basal values (figure 4C). In some rats of the HSA group, pH decreased and SD increased, although there were no significant intergroup differences at any of the time points. However, there was a significant difference in longitudinal pH measurements after liberation from mechanical ventilation in the HSA and the other three groups (HSA vs rat RBC, p<0.05; HSA vs low-P50 HbV, p<0.05; HSA vs HbV, p<0.05; repeated-measures analysis of variance).
Changes in base excess
The changes in base excess (BE) are shown as differences from the basal values (figure 4D). In some rats of the HSA group, BE decreased and SD increased, although there was no significant difference between any of the groups at any of the time points. Moreover, there were no significant intergroup differences in longitudinal BE measurements after liberation from mechanical ventilation.
Changes in oxygen saturation
The changes in oxygen saturation (sO2) are shown as percentages with reference to the basal values (figure 5A). In some rats of the HSA group, sO2 decreased and SD increased, although there were no significant intergroup differences at any time point. However, there were significant differences in longitudinal sO2 measurements after liberation from mechanical ventilation between the low-P50 HbV and the other three groups compared by repeated-measures analysis of variance (vs rat RBC, p<0.05; vs HbV, p<0.05; vs HSA, p<0.005).
Changes in arterial oxygen content
The changes in arterial oxygen content (CaO2) are shown as percentages with reference to the basal values (figure 5B). CaO2 in the low-P50 HbV group was significantly larger than that in the HSA group at transfusion (p<0.005), extubation (p<0.005), 30 min later (p<0.01) and 60 min later (p<0.01). The CaO2 value in the HbV group was also significantly larger than that in the HSA group at the transfusion (HbV vs HSA, p<0.005). There were significant differences in longitudinal CaO2 measurements after liberation from mechanical ventilation between the low-P50 HbV and rat RBC groups or the HSA group (low-P50 HbV vs rat RBC, p<0.05; low-P50 HbV vs HSA, p<0.0001; repeated-measures analysis of variance). The CaO2 levels in the rat RBC and HbV groups were significantly higher than that in the HAS group, in a comparison using repeated-measures analysis of variance (rat RBC vs HAS, p<0.0001; HbV vs HAS, p<0.0001).
Changes in serum lactate levels
The changes in serum lactate levels at each procedure are shown as differences from the basal values (figure 6). There were no significant intergroup differences at any of the time points. However, the longitudinal lactate measurements obtained after liberation from mechanical ventilation significantly differed between the low-P50 HbV and HSA groups in comparisons using repeated-measures analysis of variance (p<0.05).
Changes in the partial tissue oxygen pressure (PtO2) in renal cortex
The changes in renal cortical partial tissue oxygen pressure (PtO2) are shown as percentages with reference to the basal values (figure 7). There were no significant intergroup differences at any of the time points. However, the longitudinal PtO2 measurements showed significant differences between the low-P50 HbV group and the rat RBC and HSA groups after liberation from mechanical ventilation, in comparisons using repeated-measures analysis of variance (low-P50 HbV vs rat RBC, p<0.05; vs HAS, p<0.0001). The longitudinal PtO2 measurements in the rat RBC and HbV groups were significantly higher than those in the HSA group (rat RBC vs HSA, p<0.0001; HbV vs HSA, p<0.0001).
Discussion
The main findings in the present study are that an infusion of HbVs suspended in serum albumin, as well as transfusion of RBCs, could stabilise the haemodynamics after rapid ~30% blood loss in pneumonectomised rats with severely impaired lung function. All the rats infused with HbV solution survived after liberation from ventilation, although half of the rats infused with albumin solution without oxygen carriers died within 1 hour. HbVs, which can be preserved for years at room temperature and used irrespective of blood type with no risk of infection, could be quickly used as an alternative for RBC transfusion whenever necessary to manage unexpected massive haemorrhage in the operating room. Moreover, low-P50 HbVs with high oxygen affinity may offer advantages in increasing arterial blood oxygen content and improving organ tissue oxygenation after pulmonary resection.
Various types of haemoglobin-based oxygen carriers have been developed as transfusion alternatives, including intramolecular cross-linked, polymerised and polymer-conjugated haemoglobins.16 However, the cell-free structures of these chemically modified haemoglobin-based oxygen carriers resulted in retention of some of the side effects of molecular haemoglobins, such as renal toxicity, vasoconstriction, hypertension, higher incidence of infarction and death, and therefore clinical phase trials with these carriers failed. After the discovery of liposomes, to avoid the toxic effects of molecular haemoglobins, many research groups have attempted encapsulation of haemoglobins using liposomes, improving their biocompatibility, stability during storage and oxygen-carrying capacity.17 Although most research groups terminated their attempts because these issues were so difficult to resolve, our academic team has carried on with ongoing research and development of HbVs, successfully obtaining the present version of HbVs.18
HbVs have been proven to work as oxygen carriers in various animal models of exchange transfusion. Rats can survive after 90% exchange transfusion.19 HbVs are also used and effective for resuscitation after haemorrhagic shock in animals.15 20 Pharmacodynamic, serologic and metabolic analyses have been performed for their effects on the reticuloendothelial system. Safety evaluations include assessments of the fluctuation of cytokine levels and platelet activation after exposure to HbV.7 9 21 22 As a preclinical study, long-term survival tests after exchange transfusion of HbV in canines have also been performed.23 We expect that HbVs, which have a long expiration date, will gain widespread use in the near future in emergency medicine, isolated areas or major natural disasters, and other scenarios where donated blood cannot be provided immediately.
Lung resection procedures are fraught with the risk of the haemorrhage. In particular, anatomical lung resection procedures such as segmentectomy, lobectomy and pneumonectomy for malignant tumours entail dissection of fragile pulmonary arteries and are therefore associated with the danger of massive haemorrhage.4 Furthermore, tumour invasion to vessels increases the risk of haemorrhage. Delays in transfusion can occasionally occur even at hospitals equipped with a blood transfusion system, and these delays may expose patients to life-threatening situations. Even when resuscitation and haemostasis are successful, delays in blood transfusion can cause irreversible aftereffects such as hypoxic encephalopathy or myocardial damage due to shock and/or hypoxia. HbVs, which can be preserved at room temperature in the operation room and can be quickly transfused without a cross-matching test and without fear of infection, may be useful in avoiding these life-threatening situations and the irreversible after effects.
The short-term to long-term effects of normal HbV infusion have been evaluated in a mouse pneumonectomy model in which 40% of circulating blood was exchanged with an HbV solution.24 All the pneumonectomised mice survived after acute isovolemic haemodilution with HbV suspended in serum albumin, although half of the mice died after albumin transfusion without oxygen carriers, similar to the results obtained in the present study. The haemodilution with HbV avoided hypoxia in major organs such as the kidney, liver and brain as well as RBC transfusion, and did not cause adverse effects on recovery of food intake, body weight and spontaneous activity, and long-term survival for >6 months after surgery. However, the study did not perform haemodynamic evaluations and blood gas analysis, because the mice are too small to estimate the haemodynamic status, and the circulating blood volume in mice is too little to allow repeated analysis of blood oxygenation. Therefore, in the present rat study, we successfully evaluated the short-term effects of HbV administration on haemodynamics and conducted serial arterial blood gas analysis.
Isovolemic infusion of HbV or low-P50 HbV as well as rat RBCs with 5% of albumin compensated for ~30% blood loss and the low pulmonary function after pneumonectomy, on the basis of animal survival data and stabilisation of haemodynamics. Blood analysis showed that the arterial blood of the HbV group was oxygenated equally to the rat RBC group, and that the arterial oxygen content was also even between the HbV and rat RBC groups. The myocardium seemed to be well-oxygenated by the collaboration of HbVs and RBCs, and cardiac output could be recovered while maintaining arterial pressure. As a result, the PtO2 remained high and elevation of plasma lactate levels due to haemorrhagic shock was minimised in the HbV groups. The slight increase in lactate levels following exsanguination in all groups is thought to result from lactate production as the tissue becomes hypoxic during the several minute-shock period from blood removal to completion of transfusion. The administration of HbVs or low-P50 HbVs is not considered to compensate for the tissue hypoxia in a shock state, similar to RBC transfusion.
In our previous study, the effect of high O2-affinity HbV on oxygenation of blood and tissue was investigated in non-pneumonectomized animals with severe haemodilution (haematocrit, 11% of baseline).7 The investigations were performed in hamsters with a dorsal skinfold chamber window, and high-resolution microvascular PO2 measurements were made using phosphorescence-quenching microscopy. The findings showed improved blood and tissue PO2 when RBCs deliver oxygen in combination with a high-affinity rather than low-affinity O2 carrier. In the present study, similar improvements in blood and tissue oxygenation with high O2-affinity HbV were observed. The arterial oxygen content (CaO2) data showed that low-P50 HbV (HbV with higher O2 affinity) could take more O2 in the blood in pneumonectomised rats in which the vascular bed of the lungs which were a place of the uptake of O2 decreased. In addition, the PtO2 data seemed to indicate that more O2 was delivered to the peripheral organ tissue by low-P50 HbVs than by rat RBCs. It is possible that low-P50 HbVs retain O2 in the normal tissue while unloading O2 to a targeted hypoxic tissue. The small HbVs (250–280 nm diameter) are distributed homogeneously in the plasma phase, and HbVs can transport oxygen into hypoxic tissue through the narrow constricted arteries in animals with shock.25 Thus, infusion of low-P50 HbVs might offer an advantage over RBC transfusion in cases of shock due to the rapid and massive haemorrhage during pulmonary resection, which causes considerable decrease of pulmonary function. To precisely confirm this advantage of high oxygen affinity, we are currently conducting a study using larger-sized animals in which repeated measurement of cardiac output and analysis of mixed venous blood can be done under pneumonectomy conditions to analyse oxygen delivery and consumption.
Our study has some limitations with respect to its generalisability to a human clinical setting. First, we used small animals because no production facility has been established yet to generate HbVs in large quantities, and many HbVs are unavailable for use at a time. Prior to clinical application, it is necessary to evaluate efficacy and safety in large animals such as dogs. Second, our current evaluation only included the acute phase. We will conduct a long-term evaluation that includes the true survival time of rats in the HbV groups in the future. We did not quantify hypoxia-inducible factor-1 alpha expression, which is used as a marker to evaluate the oxygenating effects of HbVs on hypoxic organs, because we measured the tissue oxygen tension in the cortex of the kidney. Finally, the current study lacked an assessment of wound healing. Considering the potential applicability of HbV to surgery, impact on wound healing, including the measurement of collagen synthesis in wounds and the tensile strengths of suture lines, will be assessed in the future.
In conclusion, HbV stabilised circulation in the pneumonectomised rats with haemorrhagic shock as well as RBCs, and HbVs with high oxygen affinity provided better oxygenation. The present study may indicate the potential clinical application of HbVs with normal and high oxygen affinity in cases of acute massive haemorrhage during lung resection.
Acknowledgments
The authors thank the Support Center for Medical Research and Education, Tokai University School of Medicine, for assistance with animal experiments.
References
Footnotes
Presented at This study was previously presented as an abstract at the 25th European Conference on General Thoracic Surgery. This study has been also presented as an abstract at the 26th Annual Meeting of the Society of Blood Substitutes, Japan.
Contributors Conceptualisation: MK, MW, HH, KK. Funding acquisition: MK, HS. Investigation: RH, MK, KO, HO. Methodology: MK, HH. Resources: HS. Formal analysis: RH, MK. Supervision: HS, KK, MI. Validation: MK. Visualisation: MK. Writing—original draft: RH. Writing—review and editing: MK.
Funding This work was supported by Grants Promoting Clinical Trials for Development of New Drugs and Medical Devices from Japan Agency for Medical Research and Development (Grant Number 18lk1403022h0001 to HS and MK), and by a Grant-in-Aid for Fundamental Scientific Research from the Japan Society for the Promotion of Science (KAKENHI 25462183 to MK).
Competing interests HS is an inventor on patents related to the production and utilisation of haemoglobin vesicles.
Patient consent for publication Not required.
Ethics approval All procedures described in this report were approved by the Animal Experimentation Committee of Tokai University (Protocol No. 184044).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. No additional data are available.