Article Text

Abstract
Introduction Pulmonary rehabilitation is a core component of the treatment of people with chronic obstructive pulmonary disease (COPD); however, the benefits gained diminish in the ensuing months. The optimal strategy for maintaining the benefits is unclear with weekly supervised maintenance exercise programmes proposed as one strategy. However, the long-term future of maintenance programs is dependent on quality evidence.
Methods and analysis The ComEx3 randomised controlled trial will investigate the efficacy of extending a weekly supervised maintenance programme for an additional 6 months following an initial 10-week maintenance programme (intervention) by comparing with a control group who receive the same 10-week maintenance programme followed by 6 months of usual care. 120 participants with COPD will be recruited. Primary objective is to determine health-related quality of life over 12 months. Secondary objectives are to determine functional exercise capacity trajectory and to perform an economic evaluation of the intervention to the health system. Outcomes will be analysed for superiority according to intention-to-treat and per-protocol approaches.
Ethics and dissemination Approval has been received from the relevant ethics committees. Findings will be disseminated in peer-reviewed journals and conferences, targeting those involved in managing people with COPD as well as those who develop policies and guidelines.
Clinical trial registration ANZCTR 12618000933257
- pulmonary rehabilitation
- exercise
- health economist
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Pulmonary rehabilitation is an effective treatment for reducing dyspnoea and fatigue, increasing functional exercise capacity, improving health-related quality of life (HRQoL) and reducing preventable hospitalisations in people with chronic obstructive pulmonary disease (COPD).1–3 Any benefit from an initial pulmonary rehabilitation programme diminish in the ensuing 6–12 months.4 Various strategies have been recommended to maintain the benefits including supervised maintenance exercise programmes, regular telephone review, home exercise programme (HEP) supervised with home visits or an unsupervised HEP only.5 6 A meta-analysis of five trials of 445 participants with COPD showed that individuals allocated to a supervised maintenance exercise programme experienced fewer respiratory-cause admissions (risk ratio 0.62; CI 0.47 to 0.81; p<0.001)7 compared with those receiving usual care; however, this finding was heavily influenced by one trial8 that provided the longest programme duration (3 years) of supervised maintenance. The optimal strategy for maintaining the initial benefits from pulmonary rehabilitation remains unclear with the authors of the Australia and New Zealand Pulmonary Rehabilitation Clinical Practice Guidelines calling for further research and economic evaluation of a weekly supervised maintenance programme.4 9 An economic evaluation of a single 2-hour maintenance pulmonary rehabilitation session at 3, 6 and 9 months after the initial programme has shown it to be cost-effective.10 The ComEx3 study described here is a randomised controlled trial (RCT) with integral economic evaluation to assess the value of continuing a weekly supervised maintenance programme for an additional 6 months following completion of the current 10-week maintenance programme offered in community settings.
Methods and analysis
Study design
This single-blinded, parallel groups, RCT compares a 6-month extended supervised maintenance exercise programme plus an unsupervised HEP (intervention) to a 6-month usual care unsupervised HEP only (control). Both groups will then enter a ‘follow-up phase’ of usual care for 6 months (figure 1).
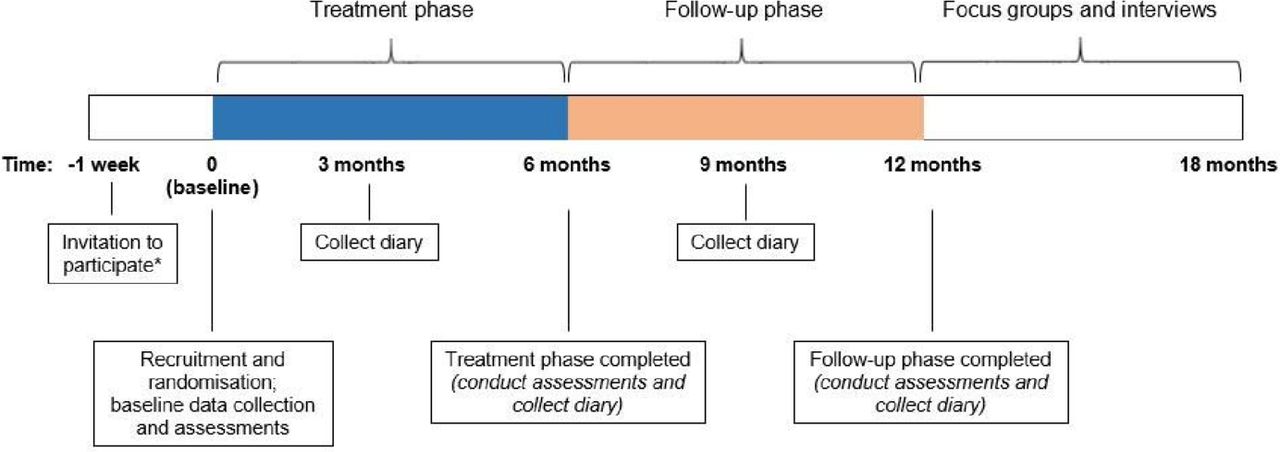
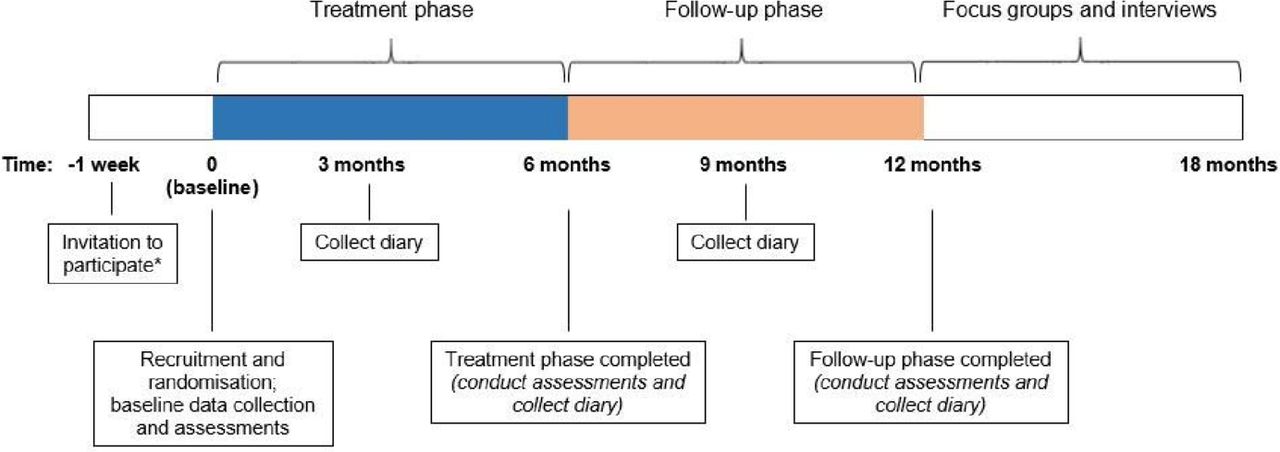{kind=link}
Flowchart depicting timing of processes, measures, focus groups and interviews during the study. *Those invited to participate have completed an 8‐week supervised initial pulmonary rehabilitation program and a 10‐week supervised maintenance program.
Hypothesis and objectives
We hypothesise that participants allocated to the intervention group will have a superior HRQoL trajectory than those in the control group over the 12-month study period. The primary objective is to determine participants’ HRQoL at 0, 6 and 12 months. Secondary objectives are to compare functional exercise capacity at 0, 6 and 12 months and healthcare utilisation at 12 months in these two groups. Furthermore, we will explore the potential economic benefits of the intervention to the Western Australian (WA) health system and participants’ perceptions of the study.
Participants
All people attending the 10-week maintenance pulmonary rehabilitation programme have completed an 8-week supervised, twice weekly initial programme. We will recruit 120 participants with a diagnosis of COPD (forced expiratory volume in 1 s (FEV1) to forced vital capacity ratio <0.7 and FEV1 <80% predicted normal) who completed at least seven classes of the 10-week maintenance programme (if absent due to illness, a further two consecutive classes on return11 at any of the six Community Physiotherapy Services (CPS) non-medical venues across Perth, WA). Recruitment will commence in June 2019 and continue until July 2020 or when 120 participants have been recruited, whichever is earlier. Individuals will be excluded if they have a new medical diagnosis (eg, stroke, musculoskeletal injury) that would preclude them from further classes or if they are unable to provide written informed consent.
Recruitment
Individuals who meet the inclusion criteria will be contacted prior to completing their 10-week maintenance programme (figure 1). Those who agree to participate will complete a 12-month healthcare utilisation history questionnaire and baseline (Time 0) assessments (see ‘Primary and Secondary measures’). This will occur prior to randomisation to blind the physiotherapist to the participant’s treatment allocation. A minimum dataset obtained from CPS records will be kept of individuals who decline to participate to determine any differences in demographic and clinical characteristics between these individuals and study participants.
Randomisation
Following baseline data collection, the trial coordinator will allocate participants to either the intervention or control group by accessing a pre-loaded randomisation list on REDCap data platform.12 The list was created using Stata V.13 in block sizes of 2 or 4 (to reduce predictability of the allocation), in a 1:1 allocation ratio, and stratified by the CPS venue.
Intervention group
Participants will attend a weekly physiotherapist-led maintenance class for a further 6 months. Each 60 min class comprises lower limb endurance exercise (20–30 min of walking prescribed at 80% of the average speed achieved on the 6 min walk test (6MWT)) and a circuit of upper limb endurance exercises and functional lower limb exercises using hand weights and body weight, respectively.5 13 Exercise intensity and duration will progress according to participant’s symptoms according to recommended guidelines.4 A 10 min ‘education session’ on the prevention and management of COPD exacerbations or the importance of exercise and physical activity will be conducted once a fortnight. These sessions will encourage individuals to actively participate and problem solve. Participants will also be encouraged to perform their HEP provided during the initial programme on three or four additional days/week. This HEP includes walking and upper and lower limb exercises as performed during classes. Participants will be provided with a weekly diary to record their adherence to the HEP, any exacerbations and hospital admissions. The diaries will be collected every 3 months. The Research Associate (RA) will contact participants each month by short message service or scripted phone call to remind them to complete the diary.
Control group
Participants will not attend any further maintenance classes but will be encouraged to perform their HEP on 4 or 5 days/week for 6 months, complete the same diary and be contacted monthly by the RA as outlined for the intervention group.
Adverse events
Any adverse event where exercise is stopped and medical advice sought will be recorded on a WA Department of Health Adverse Event Reporting Form (Datix CIMS) by the class physiotherapist and reported to the trial coordinator.
Blinding
Role separation will blind the assessor and those involved in analysis and interpretation to the treatment allocation.
Primary measures
The Chronic Respiratory Disease Questionnaire (CRQ, individualised dyspnoea domain)14 and COPD assessment test (CAT)15 will provide a comprehensive assessment of multiple HRQoL domains. These self-complete questionnaires will be administered at 0, 6 and 12 months (table 1).
Time points and descriptions for HRQoL and exercise capacity assessments
Secondary measures
Functional exercise capacity trajectory
Functional exercise capacity will be assessed at 0, 6 and 12 months (table 1) using the 6MWT performed in accordance with guidelines.16 As there is a familiarisation effect, two tests will be completed at 6 and 12 months, with the greater 6 min walk distance (6MWD) used in the analysis.16
Healthcare utilisation
The following healthcare utilisation measures will be obtained:
Non-hospitalised exacerbations are defined as a worsening of the lung condition that required the participant to take antibiotics and/or corticosteroids, doctor prescribed increased inhaler use, or visit their GP and/or specialist, or present to an emergency department that did not result in a hospital admission. Exacerbations during the entire 12-month study period will be recorded by the participant in their weekly diary.
All-cause and respiratory-related hospital admissions during the 12-month study period will be recorded by the participant in their weekly diary. Details for each admission will be verified from hospital and WA Department of Health records. Respiratory-related and all-cause admissions will be analysed separately as the number of episodes and total bed days. An episode is defined as a continuous hospital admission including inter-hospital transfers.17
Time to the first respiratory-related hospital admission will be determined from the dates recorded for hospital admissions.
Economic benefits to the WA health system
To explore the potential cost-effectiveness of the intervention to the WA health system over the entire 12-month period, healthcare utilisation will be determined as described earlier for all-cause and respiratory-related hospital admissions. To determine a participant’s self-evaluation of health status at a specific point in time for the economic evaluation, the 36-Item Short Form Health Survey (SF-36)18 will be used and converted into utility values to calculate quality adjusted life years (QALYS) (see ‘Analysis’ section).
Participants’ perceptions
An independent interviewer will conduct focus groups and interviews to explore participants’ perceptions of the study. These data will complement and expand the findings from the quantitative assessments. Up to 20 participants from each group will be recruited in the 6-month period following completion of their 12-month assessment (figure 1 and table 1).
Sample size
We aim to recruit 120 participants to allow for 20% loss to follow-up. Based on participant numbers in the maintenance programme over the last 5 years, it is feasible to recruit 60 participants to each group during a 12-month period. Based on previous research, we estimate 70% power with 50 patients per group to detect a difference of 0.5 points per item in the CRQ between the intervention and the control groups with a SD of 1.0 and alpha=0.05.11 19 This trial is planned as a pilot study to provide data (eg, an estimate of the minimal effect size for power calculations) for a future full-scale RCT.
Patient and public involvement
The trial will involve two consumer representatives who will provide links between the research team, other consumers and community members, organisations and the funding body throughout the project and after its completion.
Data management and statistical analysis
All outcomes will be analysed for superiority where analyses will be two-sided, and considered statistically significant at the 5% level. Unless otherwise stated, all analyses will be adjusted for baseline characteristics. Both intention-to-treat and per-protocol approaches will be used. A participant is considered to have completed the intervention if they attended at least 18 of the 26 (approximately 70%) community classes. In an attempt to minimise the missing data due to item non-response, the RA will document as accurately as possible the reasons for any non-completion or missing data. Missing data will be imputed using an appropriate multiple imputation method.
Analysis of the primary objective outcomes
Scores for CRQ and CAT at 0, 6 and 12 months will be analysed using linear mixed effects models including fixed effects of time, group and time by group interaction as appropriate and random effects of individual. An appropriate correlation structure for the errors will be incorporated. This will provide between-group comparisons for each time point and between time comparisons within groups.
Analysis of outcomes associated with the secondary objectives
Functional exercise capacity trajectory
The 6MWD at 0, 6 and 12 months will be analysed as per the primary objective outcomes.
Healthcare utilisation
The number of episodes of non-hospitalised exacerbations, number of episodes and total bed days of all-cause and respiratory-related hospitalisations will be analysed using either a Poisson (non-dispersed data) or negative binomial (over-dispersed data) model with adjustments for length of follow-up (accounting for death and withdrawals) and baseline covariates. Kaplan–Meier curves will be used to display the differences between the two groups in the time to first respiratory-related hospital admission, with any differences between groups compared using the log rank test. Follow-up time will be calculated from Time 0 until censoring or death before 12 months, whichever is earlier. Cox proportional hazards regression will be used to quantify the effect of intervention with adjustment for baseline covariates.
Economic benefits to the WA health system
The economic evaluation will comprise a cost-effectiveness analysis comparing differences in costs and QALYs between the two groups after 12 months from Time 0. SF-36 scores will be converted into utility values using an algorithm for the Australian population, with QALYs calculated from utility values. The perspective adopted for the evaluation will be the cost to the WA health sector. Unit costs of services will be obtained from the WA Department of Health (or hospital business units) and CPS. Differences in QALYs and total costs (including ongoing pulmonary rehabilitation costs) will be estimated as the difference between values at 0 and 12 months. Unadjusted differences in costs and health outcomes will be tested using paired t-tests for each group using 10 000 bootstrapped samples. Simple regression analysis using the measured covariates will be used to guide the extent to which more complex analysis can be undertaken to take account of the distributional characteristics of the data and any differences in baseline characteristics despite random allocation. Incremental cost-effectiveness ratios will be calculated as the net cost of the intervention over the difference in QALYs. The net cost is the cost of the intervention minus any savings in reduced hospital admissions. Net savings will be calculated as the difference between hospital admission costs for each group (after 12 months from Time 0) and will be compared with the total cost of the intervention. Sensitivity analyses will assess the robustness of the cost-effectiveness ratios subject to changes in the main variables. All costs will be calculated in Australian currency ($AUD) using 2020 as a base year.
Participants’ perceptions
Focus groups and interviews will be digitally recorded and contemporaneous notes will be made. Recordings will be transcribed verbatim while maintaining participant anonymity. Depending on the approach and findings, an appropriate framework will be chosen to analyse the transcripts.
Dissemination
We plan to disseminate findings in peer-reviewed journals, national and international conferences, targeting those involved in the clinical care of people with COPD as well as those who develop policies and guidelines for this patient population. A summary of the findings in lay terminology will be developed with the assistance of a consumer representative for sharing the findings with the study participants and the wider community. The trial is registered with Australian and New Zealand Clinical Trials Registry (Registration No: 12618000933257).
Possible risks
Participants may enrol in the study to receive further pulmonary rehabilitation; however, those allocated to the control group may then choose to withdraw from the study. Should this occur, the trial coordinator will encourage the participant to remain in the trial by emphasising the benefits of regular exercise inherent with both groups.
Quality control and mitigation of bias
As several physiotherapists are involved, the trial coordinator will perform fidelity checks of the class physiotherapists and the independent assessor to ensure they are operating according to protocol. Randomisation of participants and blinding of the investigators will reduce bias. To further reduce bias, the RA contacting participants for data collection will follow a scripted protocol to ensure equitable management of both groups. It is possible that participants may inadvertently reveal their group allocation to the independent assessor. To monitor this, following each assessment the assessor will be asked to state whether this has occurred.
Strengths and limitations
The strength of this study lies with the long-term follow-up of participants through record linkage with administrative health data from State and Federal government agencies. Limitations are the relatively modest sample size and the fact that this is a single-centre study.
Conclusion
This RCT will provide evidence as to whether HRQoL can be maintained by extending the current 10-week supervised pulmonary rehabilitation maintenance exercise programme and the cost-effectiveness of the intervention. The findings may provide a feasible format for an effective maintenance strategy that could influence clinical and policy-based decision-making across Australia to benefit people living with COPD.
References
Footnotes
Contributors DL, NC, HL, FS, EG and SJ conceived the initial study concept, and together with JC and AC, they designed the trial and wrote the protocol with statistical support from KM. DL wrote the first draft of the manuscript and NC, JC, AC, HL, FS and SJ provided early critical feedback. TB, FB, KM, KP and DP reviewed the later iterations and provided input to the study design and protocol.
Funding This project is supported by the WA Department of Health Research Translation Project grant.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval Approval has been received from the ethics committees of South Metropolitan Health Services (RGS645), WA Department of Health (DOH HREC #−2018/11) and The University of Western Australia (RA/4/20/4672). Consent will be obtained in accordance with the Australian National Health and Medical Research Council National Statement on Ethical Conduct of Human Research for the trial and for linkage to health-related administrative data from State and Federal government agencies for a future study to determine long-term outcomes (up to 10 years). The trial will be conducted according to the principles of Good Clinical Practice and Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.