Article Text

Abstract
Background A low-cost, quantitative method to evaluate sleep in the intensive care unit (ICU) that is both feasible for routine clinical practice and reliable does not yet exist. We characterised nocturnal ICU sleep using a commercially available activity tracker and evaluated agreement between tracker-derived sleep data and patient-perceived sleep quality.
Patients and methods A prospective cohort study was performed in a 40-bed ICU at a community teaching hospital. An activity tracker (Fitbit Charge 2) was applied for up to 7 ICU days in English-speaking adults with an anticipated ICU stay ≥2 days and without mechanical ventilation, sleep apnoea, delirium, continuous sedation, contact isolation or recent anaesthesia. The Richards-Campbell Sleep Questionnaire (RCSQ) was administered each morning by a trained investigator.
Results Available activity tracker-derived data for each ICU study night (20:00–09:00) (total sleep time (TST), number of awakenings (#AW), and time spent light sleep, deep sleep and rapid eye movement (REM) sleep) were downloaded and analysed. Across the 232 evaluated nights (76 patients), TST and RCSQ data were available for 232 (100%), #AW data for 180 (78%) and sleep stage data for 73 (31%). Agreement between TST (349±168 min) and RCSQ Score was moderate and significant (r=0.34; 95% CI 0.18 to 0.48). Agreement between #AW (median (IQR), 4 (2–9)) and RCSQ Score was negative and non-significant (r=−0.01; 95% CI −0.19 to 0.14). Agreement between time (min) spent in light (259 (182 to 328)), deep (43±29), and REM (47 (28–72)) sleep and RCSQ Score was moderate but non-significant (light (r=0.44, 95% CI −0.05 to 0.36); deep sleep (r=0.44, 95% CI −0.11 to 0.15) and REM sleep (r=0.44; 95% CI −0.21 to 0.21)).
Conclusions A Fitbit Charge 2 when applied to non-intubated adults in an ICU consistently collects TST data but not #AW or sleep stage data at night. The TST moderately correlates with patient-perceived sleep quality; a correlation between either #AW or sleep stages and sleep quality was not found.
- equipment evaluations
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key Messages
Can a commercially available activity tracker routinely report nocturnal sleep data in the intensive care unit (ICU) and do these assessments agree with patient-perceived sleep quality?
Use of a Fitbit Charge 2 in the ICU consistently collects total sleep time (TST) but not number of awakenings (#AW) or sleep stage data.
Fitbit Charge 2-derived TST moderately correlates with patient-perceived sleep quality; a correlation between either #AW or sleep stage and sleep quality was not found.
Introduction
Patients often complain of poor sleep during their intensive care unit (ICU) admission.1 Disrupted sleep in this setting may increase delirium risk and prolong mechanical ventilation.1 2 The use of sleep improvement protocols in the ICU, while being shown to reduce noise and patient interruption3 and lower delirium,4 have generally not been shown to improve sleep quality.1 An important barrier to demonstrating ICU sleep protocols improve sleep quality is the current lack of a low-cost, quantitative method to evaluate sleep in the ICU that is both reliable and feasible to use in daily practice.
While subjective, patient-derived sleep evaluations like the Richards Campbell Sleep Questionnaire (RCSQ) may help patients communicate their perceived sleep quality to clinicians, these instruments are challenging to use in patients who are sedated or who have delirium.5 While polysomnography (PSG) remains the gold standard method to measure sleep, in the ICU, PSG results can be difficult to score with traditional PSG scoring criteria given the relative absence of K complexes and sleep spindles in the critically ill and the frequent use of medications known to disrupt sleep architecture and regulation.6 7 Moreover, PSG is not a feasible method by which to routinely evaluate sleep in the ICU.1 Research-grade actigraphs have been shown to be feasible for use in the ICU but have not been shown to consistently agree with PSG assessments in critically ill adults. Moreover, these actigraphs are expensive and generally not available in most ICUs.8 9
Commercial activity trackers are readily available, have a relatively low cost, and if applied to critically ill adults would be unlikely to interfere with ICU daily care. These trackers have shown to quantitatively characterise sleep in healthy patients as well as actigraphy10 11 or PSG.12–14 However, published reports of their use in the ICU do not exist. Characterising the ability of an activity tracker to generate sleep quality data in the ICU, and how these data compare to patient-perceived sleep quality, are important first steps when determining the potential role of activity trackers in this setting.
The primary objective of this study was to evaluate the ability of a commercially available activity tracker to generate nocturnal values for total sleep time (TST), sleep awakenings (#AW), time spent at light, deep and REM sleep in adult, non-intubated ICU patients. A secondary objective of this study was to measure agreement between the tracker-derived TST, #AW and sleep state values and patient-perceived sleep quality. Based on published commercial activity tracker research in healthy adults we hypothesised that TST, #AW and sleep state values could be consistently collected in critically ill adults and each of these values would significantly positively correlate with patient-perceived sleep quality.
Methods
Setting
This prospective, single-centre, cohort study was conducted in the 40-bed medical/cardiac ICU in a 1350-bed community teaching hospital (Advent Health; Orlando, Florida, USA). AdventHealth Institutional review board approval (study number 1220470-9) and informed consent were obtained prior to study enrolment. All patients were managed with existing ICU pain assessment and treatment, spontaneous breathing and early mobilisation protocols. Daytime napping is discouraged. While earplugs and eye masks were available in the unit for clinicians to employ at their clinical discretion, the use of these or other sleep improvement strategies were not protocolised during the study period.
Patients
On each weekday, all adults (≥18 years) admitted to the study ICU underwent a preliminary study screen by a clinical pharmacist. A study investigator then screened and removed patients from further consideration who had one or more of the following factors that could affect the ability of the activity tracker to evaluate sleep and/or the patient to self-report sleep quality using the RCSQ: paraplegia/quadriplegia, history of sleep apnoea/insomnia, anaesthesia within 24 hours, mechanical obstruction to tracker placement, delirium, contact isolation, non-English speaking, blind or deaf, or who were currently receiving continuous sedatives. Patients meeting all study criteria were administered the Epworth Sleepiness Scale (ESS) and excluded if the ESS was >16 in an effort to remove patients from the study with an undiagnosed or undocumented pre-existing sleep condition that could confound TST measurements.15
Patient and public involvement
Patient complaints of poor sleep in the ICU and persistence after ICU discharge are well established.16 17 Increasingly, healthy adults are measuring their sleep at home using a commercially available activity tracking device.18 ICU clinicians report the current lack of a low-cost, easy-to-use, quantitative method to evaluate sleep in the ICU as an unmet need.1 19 Patients were not directly involved in the protocol development nor involved in study design, recruitment or the conduct of the study. Results will not be disseminated directly to study participants; study participants were notified of this limitation in the consent process. The burden of the intervention was not assessed by patients.
Interventions
The Fitbit Charge 2 (Fitbit; San Francisco, California, USA)18 was chosen as the commercially available activity tracker for the study given its low cost, its high global market share at the time of study and its extensive investigation as a sleep monitoring device in healthy adults.20 21 The RCSQ was chosen to evaluate patient-perceived sleep quality in the study given it has been validated against PSG in the ICU.5
Assessments
The Fitbit Charge 2 was applied to each patient’s preferred wrist over the radial tip by a study investigator to be worn continuously until ICU discharge, 7 days elapsed or a study exclusion criterion occurred. Temporary removal during procedures was permitted. Each morning, a study investigator, after confirming proper tracker placement and full battery charge, synched the Fitbit with its smartphone-enabled application using a Bluetooth connection and downloaded sleep data from the prior nocturnal (20:00 to 09:00) period.
The Fitbit Charge 2 was compared with the RCSQ. Neither actigraphy nor PSG was deemed necessary to incorporate in our study given the results of prior healthy-adult validation studies showing agreement between the Fitbit Charge 2 and both actigraphy and PSG.10–14 Patient-perceived sleep quality was measured daily between 08:00 and 13:00 using the RCSQ completed by the patient under supervision of a trained investigator.5 Responses for each domain were recorded on a 100-mm Visual Analogue Scale and averaged across the five domains to generate an overall RCSQ Score. To better characterise sleep quality distribution, <33 was deemed to denote poor sleep, 33–66 fair sleep and >66 good sleep.22
Statistical analysis
When extreme skewness was detected for any of the Fitbit outcomes, values were transformed to approximately normal distribution. Therefore, the #AW were cos-transformed, light sleep time was log-transformed and REM sleep was square root-transformed. Each outcome was then evaluated for correlation with the RCSQ Score using mixed, repeated measures models that incorporated correlation structure on random effects and residuals.23 CIs were estimated using a 1000 times cluster bootstrap method. All analysis was performed using SAS V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Among 507 patients evaluated, 76 (15%) were enrolled (age 57±15 years; 62% male, ICU length of stay (9 (4–15) days) between December 2017 and June 2019 (figure 1). The vast majority of patients were enrolled within 2 days of ICU admission and most were admitted to the ICU because of an acute on chronic cardiac/pulmonary condition (eg, decompensated heart failure and/or pulmonary hypertension). For these 76 patients, the Fitbit was applied and an RCSQ was completed for 232 nights/days (median (IQR) average =2 (1–5)). Among the 232 nights, RCSQ and TST data were available for 232 (100%), #AW for 180 (78%) and sleep stages for 73 (31%). Ten (13%) patients had no nights with #AW data; 27 (36%) had missing data for ≥1 night. Thirty (39%) patients had no nights with sleep stage data; 32 (42%) had missing data for ≥1 night.
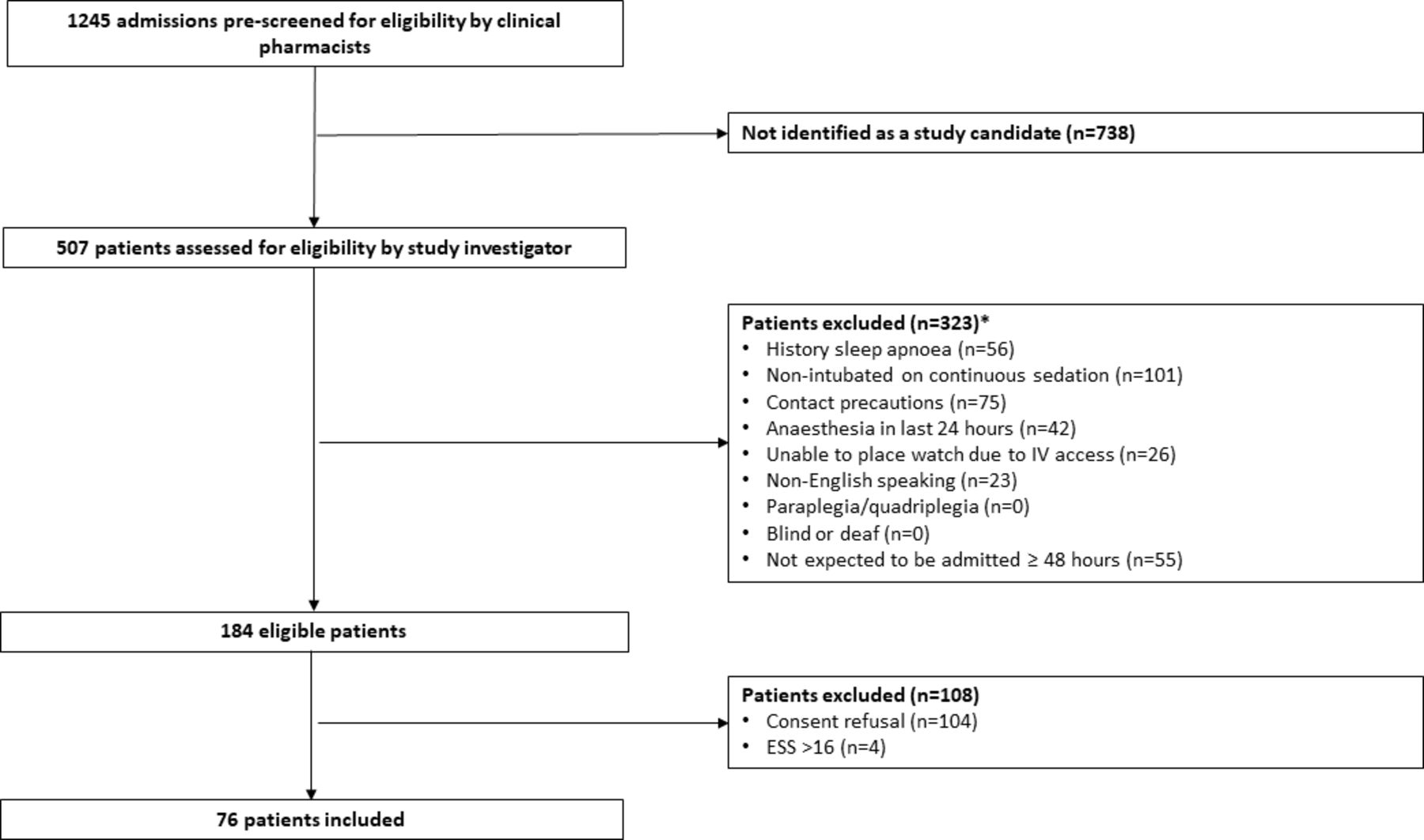
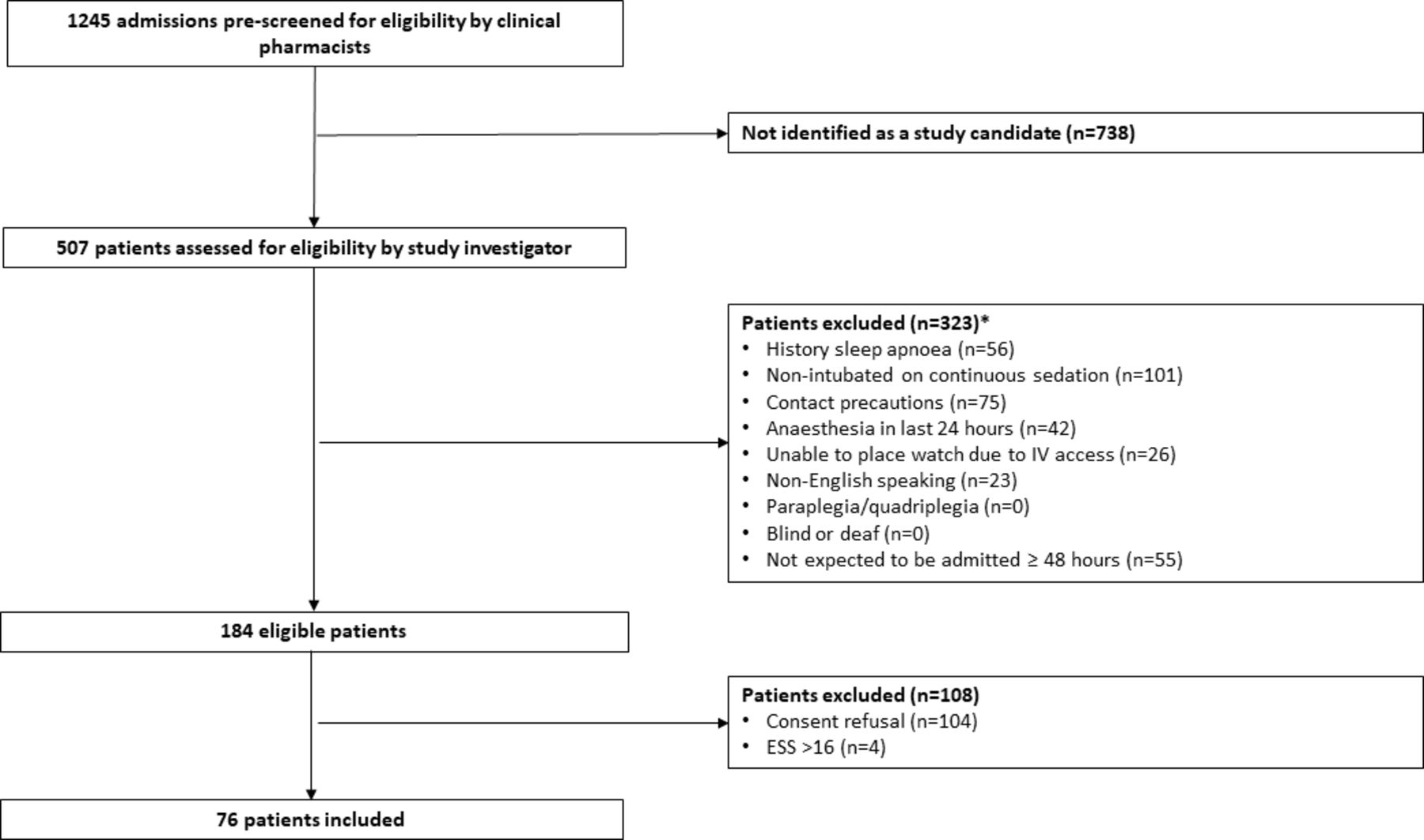{kind=link}
Patient screening and enrolment. Some patients had more than one exclusion criteria. ESS, Epworth Sleepiness Scale; IV, intravenous.
Agreement between each sleep measure and the RCSQ Score (on nights where both available) are shown in the table 1. Only TST showed significant agreement with the RCSQ Score.24 No patients had a sustained heart rate ≥100 beats per minute during any nocturnal period. The RCSQ Scores (mean, 52±25) were evenly distributed among poor (30%), fair (35%) and good (35%) sleep.
Activity tracker sleep outcomes and agreement with patient-perceived sleep quality
Discussion
Our study represents the first published investigation of using a commercially available activity tracker to evaluate sleep in the ICU. We evaluated more patients than any prior healthy patient study.10 12–14 Wearable technology such as research-grade actigraphy or other advanced activity watches show potential for various healthcare applications.25 The Fitbit Charge 2 was chosen due to its potential for more broad application as it offers the advantage of widespread availability, low cost, favourable patient perception, ease of cleaning and potential for utilisation for other areas than sleep such as mobility (step) tracking both during and after the ICU stay.20 21
When applied to a highly selected group of non-intubated adults, the Fitbit Charge 2 was able to characterise TST for all patients on all ICU nights. However, it was able to characterise awakenings on all ICU nights in only half the patients and sleep stage data on all ICU nights in less than a fifth of the patients. The reason for the high prevalence of missing awakening and sleep stage data remains unclear given TST data were available on all ICU nights and the reported frequency of missing awakening and sleep stage data in healthy adults has been reported to be less than 5%.12 13 According to the manufacturer, sleep data are most frequently missing during periods of substantial heart rate variability (HRV), which is not further defined, or when the TST is <3 hours.18 Of note, the Fitbit Charge 2 relies on detecting the heart rate fluctuation that occurs during sleep stage transitions to differentiate between light, deep and REM sleep. Exact algorithms are considered proprietary by device and not available. Although HRV could be affected by underlying cardiac disease, no patient had sustained nocturnal tachycardia and the TST was <3 hours on only 26% of the nights where awakening and/or sleep stage data were missing.
While the Fitbit did provide data on number of times restless (median (IQR) 7 (3–13)) and the minutes awake (23 (8–41)) for some of the assessments where sleep staging data were unavailable, the relationship between these values and sleep stage tracking is not known. Fragmented sleep, while not evaluated in our study, is common in the ICU and may influence tracker device output.13 19 26 The ICU day the assessment was conducted may have also confounded the results we report as the degree of sleepiness during an ICU stay may grow over the course of the admission. Future investigation is required to better understand how patient, time in ICU and sleep-related characteristics differ between critically ill and healthy adults and how these factors affect sleep-related tracker values.
The TST-RCSQ agreement we report is consistent with Fitbit-generated TST evaluations of healthy adults where TST also correlated moderately with patient-perceived sleep quality.11 In other healthy patient studies, Fitbit-derived TST has been shown to correlate strongly with TST measured by actigraphy or PSG.12 13 The Fitbit Charge 2 has been shown to underestimate sleep stage readings with missed #AW in health populations,12 13 26 and utility of stage tracking for everyday consumers has been questioned.27 While our results suggest a moderate correlation may exist between Fitbit-derived ICU sleep stage data and patient-perceived sleep quality, sleep stage data were available on too few nights to reach significance and make any firm conclusions on sleep stage-RCSQ agreement. These results suggest the need for more study prior to routine use in ICU patients. Given the Fitbit Charge 2 relies on detecting light, deep and REM sleep transitions using a combination of triaxial accelerometry (ie, movement) and optical heart rate sensors,12 future studies should also incorporate both continuous patient video and heart rate monitoring.
The RCSQ was able to be completed in 100% of attempts, a completion rate higher than other studies,28–30 that demonstrates its feasibility when administered as a repeated assessment in an ICU cohort. Overall, sleep was classified as fair with a mean RCSQ of 52±25, which is comparable to previously reported ICU means of 34–60.28–30 The even distribution of RCSQ scores across poor, fair and good sleep groups suggests that all correlation efforts were conducted across the entire spectrum of patient-perceived sleep quality.
Generalisability from our study to all ICU patients is limited given patients with a history of a sleep condition, a factor potentially affecting Fitbit assessment (paraplegia/quadriplegia), or a condition affecting reliable RCSQ completion (eg, delirium) were excluded. While our results cannot be applied to mechanically ventilated adults with a higher severity of illness, it is possible that the Fitbit detection issues we observed in our study may be even greater in sicker ICU populations. The RCSQ has limitations as a method to validate ICU tracker use in the ICU given it cannot reliably estimate TST or #AW like actigraphy or time spent at each sleep stage like PSG. Moreover, the RCSQ may be subject to potential recall bias and rater fatigue when administered repeatedly.5 Although up to 50% of sleep in critically ill adults occurs during the daytime, we discourage daytime sleeping in our ICUs to facilitate regular daytime mobilisation.19 31 Therefore, only nocturnal values were included in our analysis. Future investigations should evaluate the ability of the Fitbit two to detect altered circadian rhythmicity. Based on these concerns and the results of our study, future studies investigating nocturnal sleep tracker use in the ICU should incorporate actigraphy (or PSG), collect heart rate continuously and consider characterising daytime sleep patterns. Newer activity tracker models, not available at the time of our study, incorporate continuous HR measurement in their algorithms and may be options to incorporate into future studies.
Conclusions
The Fitbit Charge 2 appears to measure TST in non-intubated ICU patients, the results of which correlate moderately with patient-perceived sleep quality. However, it cannot consistently measure #AW or sleep quality in the ICU. Future research is required before commercially available activity trackers should be used to characterise sleep in the ICU.
Supplemental material
References
Footnotes
Contributors PL takes full responsibility for the content of the manuscript. JA, XT, EP, MA and PL were involved in the conception and design of the study and acquired all data. JA, XT, EP, MA, PL,YD and JD analysed the data and drafted the manuscript.
Funding This study was supported by an unrestricted grant from the American Society of Health-System Pharmacists. Neither the sponsor (or the manufacturer of the activity tracker used in the study) had a role in the conception, design or conduct of this study; collection, management, analysis, interpretation or presentation of data; or preparation, review or approval of this manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.