Article Text

Abstract
Introduction Idiopathic pulmonary fibrosis (IPF) and systemic sclerosis-associated interstitial lung disease (SSc-ILD) are fibrotic ILDs with divergent disease populations. Little is known about health-related quality of life (HRQL) in SSc-ILD relative to IPF.
Methods We used the Kings Brief Interstitial Lung Disease Questionnaire (K-BILD) to compare HRQL in a cross-sectional study of 57 patients with IPF and 29 patients with SSc-ILD. Analysis of covariance was used to adjust for age, gender and lung function.
Results The unadjusted mean K-BILD score was 63.1 (95% CI 57.1 to 69.1) among patients with SSc-ILD, as compared with 54.7 (51.8–57.5) among those with IPF (p=0.005). However, this difference in HRQL was attenuated after adjustment for age, gender and lung function. In a multivariable model, only forced vital capacity was associated with K-BILD scores. K-BILD scores were correlated with both forced vital capacity and with other relevant HRQL measures, regardless of ILD diagnosis.
Discussion Patients with SSc-ILD may have better ILD-specific quality of life than patients with IPF, but this difference appears to be driven primarily by better lung function. These results underscore the impact of lung function on HRQL in fibrotic ILD and the utility of K-BILD to assess HRQL in SSc-ILD.
- systemic disease and lungs
- interstitial fibrosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
How does interstitial lung disease (ILD)-specific quality of life in systemic sclerosis-associated interstitial lung disease (SSc-ILD) compare with idiopathic pulmonary fibrosis (IPF)?
Unadjusted ILD-specific quality of life as measured by the Kings Brief Interstitial Lung Disease (K-BILD) Questionnaire was better in SSc-ILD than in IPF, but this difference appeared to be driven primarily by better lung function among patients with SSc-ILD.
These data highlight the importance of lung function impairment in ILD-specific quality of life, and support the use of the K-BILD Questionnaire to assess disease-specific quality of life in systemic sclerosis-associated ILD.
Introduction
Interstitial lung disease (ILD) is associated with reduced health-related quality of life (HRQL).1 2 While idiopathic pulmonary fibrosis (IPF) has been considered the archetypal fibrotic ILD, it is increasingly recognised that other ILDs may have a progressive fibrotic phenotype in some patients.3 Such patients may have common biological and clinical characteristics independent of underlying diagnosis, which has provided rationale for several recent trials of antifibrotic therapy in non-IPF ILDs.4–6 Systemic sclerosis-associated ILD (SSc-ILD) has recently become the second form of ILD, in addition to IPF, for which the antifibrotic drug nintedanib has been approved in the USA, Canada and Europe.
However, compared with IPF, SSc-ILD is a manifestation of a multisystemic disease affecting a younger population.7 Although individual disease trajectories vary, disease progression is slower and mortality lower in general among patients with SSc-ILD.8 While overall HRQL is impaired in SSc,9 there is a paucity of studies of HRQL using ILD-specific tools in SSc, and the extent to which ILD-related HRQL in SSc-ILD differs from IPF is not well understood.
ILD-specific HRQL instruments, such as the Kings Brief Interstitial Lung Disease (K-BILD) Questionnaire, have been developed and validated across a range of ILDs.10 Disease-specific as compared with generic tools may be more sensitive for identifying impairment and assessing change in HRQL. Assessing differences in HRQL between different fibrotic ILDs is important to understand the patient populations for whom antifibrotic therapy is relevant, and potentially to determine the effects of such treatment.
Because IPF is more frequently progressive than SSc-ILD, we hypothesised that IPF is associated with greater impairment in ILD-specific HRQL than SSc-ILD. We used the K-BILD to assess ILD-specific HRQL in patients with SSc-ILD as compared with IPF.
Methods
Study design and patients
This was a cross-sectional study enrolling adult patients aged ≥18 years with IPF and SSc-ILD during ambulatory visits at three university hospitals in Norway. Diagnoses were based on current consensus criteria for IPF11 and SSc12 at the time of the study. Exclusion criteria included chronic lung diseases other than IPF or SSc-ILD, and inability to understand or complete self-administered questionnaires in Norwegian. As not all patients with SSc have ILD, the presence of ILD was verified by review of both the medical record and chest CT at the time of enrolment. Consecutive eligible patients were approached for inclusion; no patients declined inclusion. Sample size considerations are given in more detail in the online supplementary file. A total of 87 patients provided written informed consent and were included in the original study. One patient did not complete the K-BILD Questionnaire, leaving 86 patients included in the current analysis.
Supplemental material
K-BILD and other quality of life measures
The development of the Norwegian version of the K-BILD Questionnaire is summarised in online supplementary figure 1. The original validated English version of the K-BILD10 was used as a basis for developing the Norwegian version. After consultation with the original developers of K-BILD, the organisation Mapi Research Trust (Lyon, France) conducted the translation as per the developer’s instructions. Briefly, the questionnaire was first translated into Norwegian by two independent bilingual translators. These two independent translations were then reconciled. This reconciled version was then vetted through a process of back-translation to English and review by the original developers of the instrument as well as independent quality assurers for content validity. This vetted, reconciled Norwegian version was subsequently subjected to review by key Norwegian experts within the field of ILD, before linguistic testing with five patients using cognitive interviews, leading to the final Norwegian version of K-BILD. In addition to the K-BILD, patients completed the St. Georges Respiratory Questionnaire (SGRQ),13 Leicester Cough Questionnaire (LCQ)14 and EuroQol-5D (EQ-5D) index.15
Statistical analysis
K-BILD total and domain scores were calculated using the logit-based method. Scores range from 0 to 100 with higher scores indicating better HRQL.16 Mean unadjusted K-BILD scores were compared using t-tests. Analysis of covariance was used to adjust for age, gender, forced vital capacity (FVC) and diffusing capacity of lung for carbon monoxide (DLCO). Covariates were prespecified and selected based on known or clinically plausible effects on ILD-specific HRQL. No form of variable selection was used in the modelling process. Linear models were used to assess the relationships between K-BILD scores, lung function and other HRQL measures. Interaction terms assessed whether relationships differed by diagnosis.
Patient and public involvement
Patients or the public were not directly involved in the design, conduct, reporting or dissemination plans of our research.
Results
Fifty-seven patients with IPF and 29 patients with SSc-ILD were included between September 2017 and October 2018. Compared with patients with IPF, those with SSc-ILD were younger (mean age 59 vs 71 years), predominantly female (79% vs 28%), and had better lung function (FVC 87% vs 73% of predicted, DLCO 57% vs 45% of predicted). The majority of patients with IPF were treated with pirfenidone or nintedanib, whereas over half of those with SSc-ILD were treated with immunosuppressive drugs (table 1).
Demographic and clinical characteristics
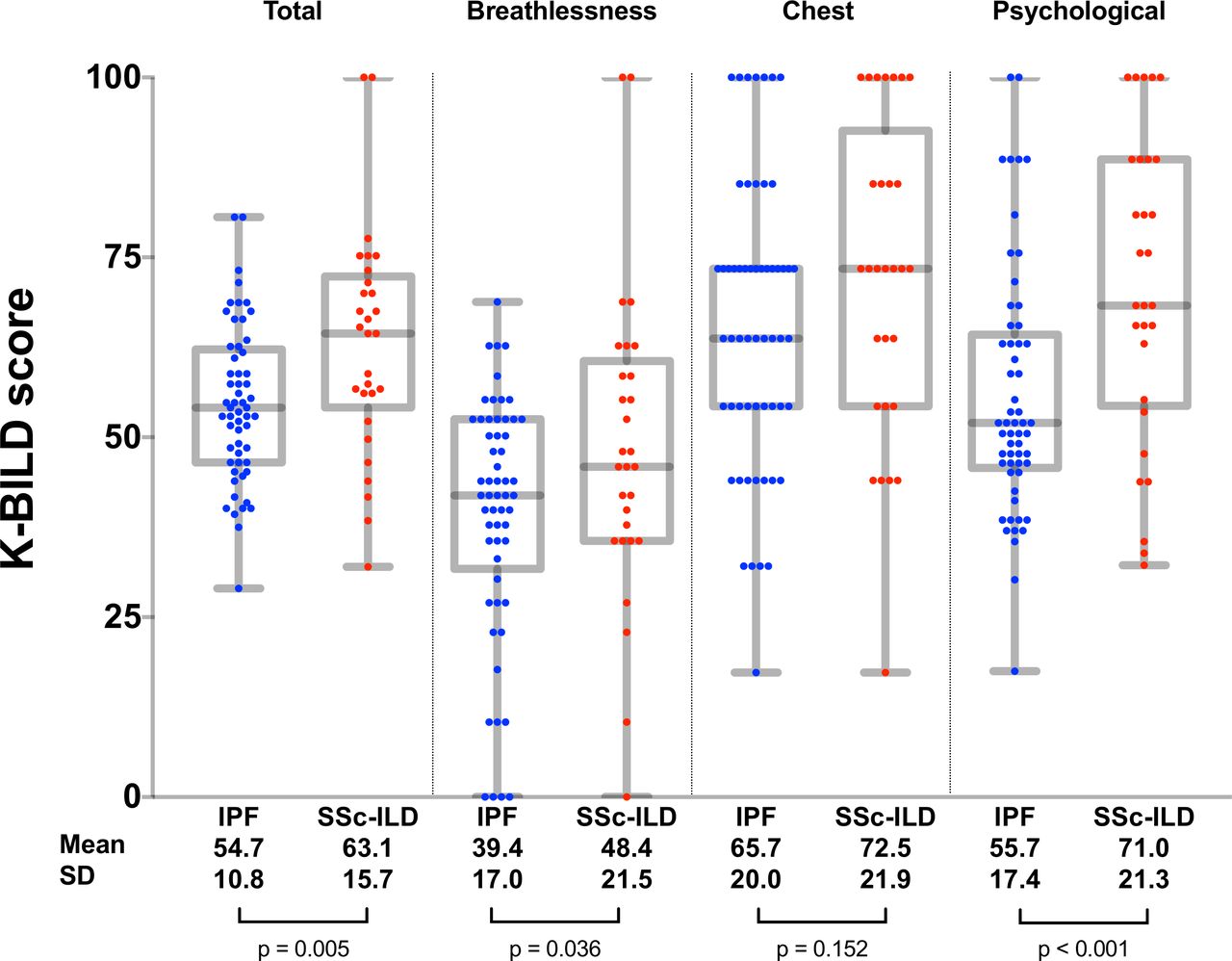
The mean K-BILD score was 63.1 (95% CI 57.1 to 69.1) among patients with SSc-ILD, as compared with 54.7 (95% CI 51.8 to 57.5) among those with IPF (p=0.005), indicating better ILD-related HRQL in SSc-ILD (figure 1). After adjustment for age, gender, FVC and DLCO, the difference was slightly attenuated, with adjusted mean K-BILD score 62.6 (95% CI 57.0 to 68.2) in SSc-ILD and 55.5 (95% CI 51.9 to 59.1) in IPF (p=0.061, table 2).
Adjusted K-BILD total and domain scores
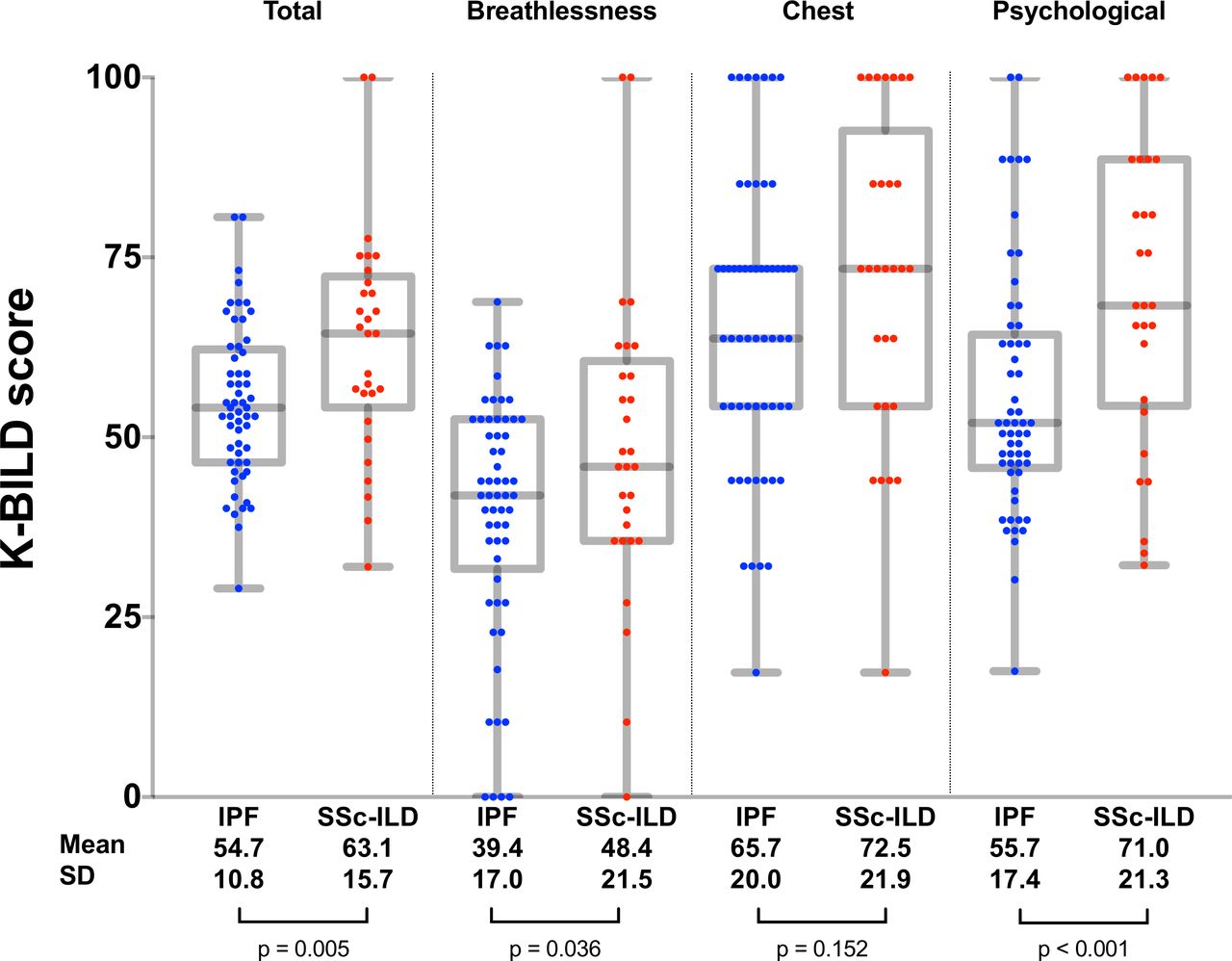
Kings Brief Interstitial Lung Disease (K-BILD) total and domain scores. Unadjusted mean total and domain K-BILD scores are shown for the idiopathic pulmonary fibrosis (IPF) and systemic sclerosis-associated interstitial lung disease (SSc-ILD) groups below the X-axis, with values for individual patients shown in the plot. The box and whiskers plots show median, 25th and 75th percentiles, minimum and maximum values. P values shown are for two-sample t-test comparisons between IPF and SSc-ILD.
K-BILD domain scores indicated that patients with IPF had greater breathlessness compared with patients with SSc-ILD (figure 1), but this difference was not significant after multivariable adjustment (table 2). Psychological domain scores indicated better psychological QOL in SSc-ILD, and this difference remained significant after multivariable adjustment.
Associations between K-BILD total score, lung function and other HRQL measures are shown in figure 2. There was a significant association between K-BILD total score and both FVC and DLCO, with higher FVC or DLCO associated with better HRQL. K-BILD total scores correlated with other HRQL measures, including the SGRQ, LCQ and EQ-5D index. None of these relationships differed by diagnosis (interaction p>0.05 for all).

{kind=link}
{kind=link}
Relationships between Kings Brief Interstitial Lung Disease (K-BILD) total score, lung function and other health-related quality of life measures. Plots show the relationship between the given lung function or health-related quality of life (HRQL) measure and K-BILD total score in the overall study population. There were no significant statistical interactions with diagnosis. Regression coefficients therefore represent the univariable association between K-BILD total score and the given measure in the overall study population, and correspond with the regression line shown. Individual data points are presented separately for each diagnosis for illustrative purposes. DLCO, diffusing capacity of lung for carbon monoxide; EQ-5D, EuroQol; FVC, forced vital capacity; IPF, idiopathic pulmonary fibrosis; LCQ, Leicester Cough Questionnaire; SGRQ, St. George Respiratory Questionnaire; SSc-ILD, systemic sclerosis-associated interstitial lung disease.
In a multivariable model including age, gender, FVC and DLCO, only FVC was significantly associated with total K-BILD scores (online supplementary table 2).
Discussion
ILD-specific HRQL assessed by K-BILD appears to be similar between patients with IPF and SSc-ILD after adjustment for age, gender and lung function, with restrictive lung physiology as measured by FVC strongly correlated with HRQL in both disease groups. However, unadjusted ILD-specific HRQL was better in SSc-ILD than in IPF, suggesting that younger age and better lung function may contribute to better HRQL among patients with SSc-ILD. Patients with SSc-ILD had better psychological quality of life than those with IPF, independent of age and lung function differences.
Compared with the mixed ILD population in which the K-BILD was developed,10 patients with IPF in our study had generally poorer HRQL, despite only slightly lower lung function. Patients with IPF enrolled in a national registry in Sweden had similarly poor HRQL as assessed by the K-BILD.17 Taken together, these findings suggest that IPF may be associated with especially poor HRQL compared with other ILDs. By contrast, K-BILD scores among patients with SSc-ILD in our study were similar to those in previous mixed ILD populations.10
Even after adjustment, psychological HRQL remained markedly better in SSc-ILD. These data suggest that disease-specific factors, rather than severity of lung disease, may be most related to psychological HRQL in the ILD population. Our data cannot offer a definite explanation for this finding, but it is notable that several of the K-BILD items that comprise the psychological domain refer to anxiety, concern or expectations related to disease worsening. In this context, it is possible that the relatively widespread knowledge about poor prognosis and risk of progression in IPF may have negative impact on psychological HRQL among patients, above and beyond their actual objective disease severity at a given time.
Compared with IPF, SSc-ILD is a multisystem disorder, and extrapulmonary manifestations may impact overall HRQL substantially. Having been developed as an ILD-specific instrument, the K-BILD is unlikely to capture the overall impact of SSc on HRLQ. While the K-BILD items refer explicitly to the impact of lung disease, other SSc manifestations with overlapping symptoms, such as pulmonary hypertension, could plausibly affect patients’ responses to the items. On the other hand, patients with IPF may have secondary pulmonary hypertension or other, unrelated, cardiopulmonary comorbidities that impact patient responses.
SSc-ILD is the second form of ILD other than IPF with specific approved therapy, with the SENSCIS trial demonstrating a benefit of nintedanib in reducing the rate of decline in FVC.4 In this context, tools to help understand disease-specific HRQL in SSc-ILD will be increasingly important in understanding disease characteristics, progression and the effects of treatment in clinical practice. In our study, K-BILD scores correlated as expected with FVC and other validated HRQL instruments commonly used in ILD, including the SGRQ, LCQ and EQ-5D. These associations were largely independent of diagnosis, and support the validity of the K-BILD as an instrument to assess HRQL also among patients with SSc-ILD.
Our study has several limitations. First, the cross-sectional design precludes the assessment of K-BILD as a tool for longitudinal assessment of ILD-specific HRQL over time in SSc-ILD. An established tool for assessing changes in ILD-specific HRQL over time would be particularly helpful for evaluating emerging therapies, and represents a pressing need for future patient-reported outcome research. Second, the study enrolled only from academic centres; however, in Norway, the vast majority of patients with IPF and SSc-ILD are managed at such centres, such that our cohort is likely to be representative of the overall Norwegian patient population with these conditions. Finally, available treatments for both IPF and SSc are associated with substantial side effects, which our study design did not allow us to investigate specifically. In particular, nearly all patients with IPF in the study were taking antifibrotic therapy, which did not allow the effects of such therapy to be separated from the main effect of IPF versus SSc, and no patients with SSc-ILD were on such therapy. In contrast, a large majority of patients with SSc-ILD, but no patients with IPF, were taking immunosuppressive medications. While the K-BILD items are specifically formulated to address the effects of the lung disease itself, the impact of treatment side effects is likely to contribute substantially to overall HRQL and should be a priority in future HRQL research in these disease populations.
Conclusions
HRQL as measured by K-BILD is similar in IPF and SSc-ILD after accounting for differences in age, sex and lung function. HRQL is associated with with restrictive lung physiology in both diseases. K-BILD correlates well with other relevant HRQL measures, and appears to be a useful instrument for measuring HRQL also in SSc-ILD. Further studies should compare change in HRQL as measured by K-BILD over time in SSc-ILD and IPF.
References
Footnotes
Contributors MTD performed the statistical analyses and drafted the manuscript. A-MH-V, TME, GB, TMJ and TS enrolled patients and collected data. A-OH, SSB and OEJ contributed to development of the Norwegian version of K-BILD. All authors were involved in planning the study and provided critical feedback on the manuscript.
Funding The development of the Norwegian language version of K-BILD was funded by Boehringer Ingelheim Norway KS.
Competing interests MTD reports research funding from Boehringer Ingelheim Norway KS, unrelated to the current study, lecture and consulting fees from Boehringer Ingelheim, Roche and AstraZeneca, unrelated to the current study, having participated in advisory boards for Boehringer Ingelheim and Roche, and that an immediate family member is a full-time employee of Boehringer Ingelheim who was not involved in this study. A-MH-V reports research funding and/or consulting fees or other remuneration from Actelion, Boehringer Ingelheim, Bayer, Roche, MSD and GlaxoSmithKline. TE reports receiving lecture fees from Boehringer Ingelheim and having participated in advisory boards for GlaxoSmithKline and Boehringer Ingelheim. A-OH and OEJ are full-time employees of Boehringer Ingelheim Norway KS. MBL and GB have no competing interests to report. SB reports research funding to his institution for the use of K-BILD in other studies, but not for the current study. TMJ reports receiving lecture fees from Boehringer Ingelheim and Roche. TS reports lecture fees from Boehringer Ingelheim and Roche.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval All patients provided written informed consent, and the study was approved by the relevant institutional review boards.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available on reasonable request, provided that patient data security requirements of the authors’ institutions are upheld.