Article Text

Abstract
Background The diagnosis of chronic obstructive pulmonary disease is based on the presence of persistent respiratory symptoms and chronic airflow limitation (CAL). CAL is based on the ratio of forced expiratory volume in 1 s to forced vital capacity (FEV1:FVC) after bronchodilation, and FEV1:FVC less than the fifth percentile is often used as a cut-off for CAL. The aim was to investigate if increasing percentiles of FEV1:FVC were associated with any respiratory symptom (cough with phlegm, dyspnoea or wheezing) in a general population sample of never-smokers and ever-smokers.
Methods In a cross-sectional study comprising 15 128 adults (50–64 years), 7120 never-smokers and 8008 ever-smokers completed a respiratory questionnaire and performed FEV1 and FVC after bronchodilation. We calculated their z-scores for FEV1:FVC and defined the fifth percentile using the Global Lung Function Initiative (GLI) reference value, GLI5 and increasing percentiles up to GLI25. We analysed the associations between different strata of percentiles and prevalence of any respiratory symptom using multivariable logistic regression for estimation of OR.
Results Among all subjects, regardless of smoking habits, the odds of any respiratory symptom were elevated up to the GLI15–20 strata. Among never-smokers, the odds of any respiratory symptom were elevated at GLI<5 (OR 3.57, 95% CI 2.43 to 5.23) and at GLI5–10 (OR 2.57, 95% CI 1.69 to 3.91), but not at higher percentiles. Among ever-smokers, the odds of any respiratory symptom were elevated from GLI<5 (OR 4.64, 95% CI 3.79 to 5.68) up to GLI≥25 (OR 1.33, 95% CI 1.00 to 1.75).
Conclusions The association between percentages of FEV1:FVC and respiratory symptoms differed depending on smoking history. Our results support a higher percentile cut-off for FEV1:FVC for never-smokers and, in particular, for ever-smokers.
- clinical epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Which percentiles of forced expiratory volume in 1 s to forced vital capacity ratio (FEV1:FVC) are associated with increased prevalence of respiratory symptoms in the general population?
This study demonstrates that a higher percentile (≥10th) of FEV1:FVC, among never-smokers, but in particular among ever-smokers, is associated with chronic obstructive pulmonary disease-related respiratory symptoms.
Our results indicate that the prevalence of respiratory symptoms is increased also at percentiles of FEV1:FVC exceeding the fifth percentile.
Introduction
Chronic airflow limitation (CAL) is defined by spirometry after bronchodilation, while diagnosis of chronic obstructive pulmonary disease (COPD) requires respiratory symptoms in addition to CAL.1 2 However, it has been reported that smokers with normal lung function have increased prevalence of respiratory symptoms, as well as a number of comorbidities.3 4 A considerable proportion of individuals with COPD have never smoked, and data are sparse on how this phenotype differs from COPD among smokers in terms of symptoms and mortality.5 6
There is a number of different ways to assess CAL. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends using a fixed ratio of forced expiratory volume in 1 s to forced vital capacity (FEV1:FVC) <0.70.1 An alternative approach is to estimate the distribution of FEV1:FVC in a healthy population, conditional on factors such as age, sex and height.7 An FEV1:FVC less than the fifth percentile of this value is used as a cut-off, referred to as the ‘lower limit of normal (LLN5)’. This approach has been jointly recommended by the American Thoracic Society (ATS) and the European Respiratory Society (ERS).8 Several different reference equations have been presented, many of which were estimated using ordinary least squares regression. These have been criticised for the underlying assumption that the values are conditionally normally distributed with constant variance.9 Reference equations published by the Global Lung Function Initiative (GLI) were estimated using the lambda-mu-sigma (LMS) method. This method relaxes the assumptions of linearity, constant variance and normality.9 10
The assessment of CAL is based on the FEV1:FVC ratio with different cut-off limits proposed, and the underlying assumption is that the selected cut-off limit is a marker of increased morbidity and mortality.10 However, there is no clear threshold for lung function, and measures of lung function such as FEV1:FVC as well as many other clinical measurements are measured along a continuous scale. Hence, the decision limits must be based on both epidemiological data and clinical considerations. One way of establishing decision limits is to evaluate the effect of successively higher percentiles in relation to clinically relevant symptoms.11 12 In a general population-based study from the USA comprising 3502 individuals, it was shown that among subjects with FEV1:FVC below LLN5 based on the LMS method, the adjusted ORs for respiratory symptoms (cough with phlegm, wheezing or dyspnoea) were significantly and almost threefold increased.9 However, at higher percentiles, the adjusted ORs were still increased, but lower and without statistical significance. No separate analyses of never-smokers were presented, even if never-smokers constituted 40% of the population.
We therefore propose that successively higher (more inclusive) LMS-derived percentiles should be evaluated in relation to clinically relevant symptoms, a composite outcome of cough with phlegm, dyspnoea and wheezing, in large powerful studies, and that these associations should specifically be evaluated in never-smoking populations.
Methods
Study population
Participants were randomly selected from the Swedish population register and invited to participate in the Swedish CArdioPulmonary bioImage Study (SCAPIS), a cross-sectional study of a general population sample. The participation rate was around 50%.13 14 The present study was part of an interim analysis and was performed when half of the expected sample had been included. Thus, the current population sample included 15 810 adults, 7122 of whom were never-smokers, aged 50–64 years, 7625 men and 8185 women. All subjects answered an extensive respiratory questionnaire comprising the modified Medical Research Council (mMRC) scale, which includes five grades (0–4) for assessing dyspnoea, along with items about smoking habits and socioeconomic status.
Spirometry
Dynamic spirometry including FEV1 and FVC was performed at least 15 min after inhalation of 400 µg of salbutamol with the subject in a sitting position using a nose clip.15 In all measurements, a Jaeger MasterScreen PFT (Vyaire, Mettawa, Illinois, USA) was used. All procedures were performed according to the ATS/ERS standards.15 Based on the GLI equations, z-scores were calculated for FEV1:FVC, FEV1 and FVC.10 A local reference material was used for calculation of per cent predicted of FEV1 and FVC and LLN5 for FEV1:FVC.16
Definitions
CALGOLD was defined as FEV1:FVC <0.7.1
CALGOTHENBURG was defined as FEV1:FVC ratio below LLN5 using local reference equations.16
CALGLI was defined as FEV1:FVC below GLI5 applying the GLI equations.10
Restrictive spirometric pattern (RSPGLI) was defined as FEV1:FVC ≥LLN5 and FVC <LLN5 based on the GLI equations.17
Normal lung function (NormalGLI) was defined as FEV1:FVC ≥GLI5 and FVC ≥GLI5 using the GLI equations.
Asthma was defined as ‘physician-diagnosed asthma’.18
Cough with phlegm was defined as cough with phlegm lasting for at least three consecutive months for at least 2 years.
Dyspnoea was self-reported using the mMRC scale, and for this study dyspnoea was defined as mMRC >1.19–21
Wheezing was defined as an affirmative answer to ‘Do you have wheezing or whistling in your chest?’
The primary outcome was a composite outcome any respiratory symptom, defined as having cough with phlegm, dyspnoea and/or wheezing. The different respiratory symptoms were also analysed separately, as secondary outcomes.
Smoking history was categorised as current smokers, former smokers and never-smokers. Former smokers were defined as those who had smoked for at least 1 year but not during the last year. Ever-smokers included both current and former smokers. Pack-years were calculated for all participants with a history of smoking. Never-smokers were defined as those who gave an affirmative answer to the item ‘No, I have never smoked’.
Body mass index (BMI) was defined as measured weight/height2.
Patient and public involvement
Patients and the public were not involved in the design, or conduct or reporting of the present research, the SCAPIS. The Swedish Heart and Lung Foundation is involved in the dissemination of the results.
Statistics
We calculated z-scores for the FEV1:FVC ratio using the GLI reference equations.10 We transformed the z-scores to quantiles of the normal distribution and defined groups using the 5th, 10th, 15th, 20th and 25th percentiles as cut-off points. For the sake of brevity, we here used the notation GLI with a number or range, for example, GLI5–10 refers to individuals with FEV1:FVC between the 5th and 10th percentiles according to the GLI equations. We analysed the association between the GLI-defined strata and the primary outcome, any respiratory symptom, using OR estimated with multivariable logistic regression models among never-smokers, ever-smokers and all subjects. We also analysed the secondary outcomes, cough with phlegm, dyspnoea and wheezing. All models included age, sex, BMI, asthma, smoking and pack-years. The latter variables were not included in models for never-smokers. In one approach, we used individuals above the 25th percentile (GLI25) as the reference group and presented the results in similarity with Vaz Fragoso et al.9 We used cubic restricted splines with four knots placed at the 5th, 35th, 65th and 95th percentiles for BMI and pack-years, respectively.22 We also performed sensitivity analyses excluding all subjects with RSP, excluding all subjects with FVC <10th percentile and one model not adjusted for current smoking, that is, the model included only pack-years.
In an extended analysis, we treated the z-scores as a continuous variable using a spline with five knots placed at the observed quantiles 0.05, 0.275, 0.5, 0.725 and 0.95. We used a z-score of 0, that is, the 50th percentile (GLI50), as the reference point for ORs and present the results as graphs with the x-axis indicating percentiles.
All analyses were performed using SAS V.9.4 M5. All results from the logistic regression models are expressed as OR with 95% CI. P values <0.05 were considered significant.
Results
Of the 15 810 individuals originally included, 162 subjects were excluded due to incomplete spirometry data, 12 subjects because FEV1>FVC and 508 subjects due to incomplete data on smoking habits. The final study population of 15 128 subjects is presented in table 1. The mean age of participants was 57.5 years, 52.0% were women and 47.1% were never-smokers. The prevalence of any respiratory symptom was 13.3%, among never-smokers 9.5% and among ever-smokers 16.8%. The prevalence of CALGOLD (9.7%) and CALGOTHENBURG (9.1%) was significantly higher compared with CALGLI prevalence (5.1%). RSPGLI was found in 338 individuals (2.2%).
Descriptive data of the study participants, by sex and smoking
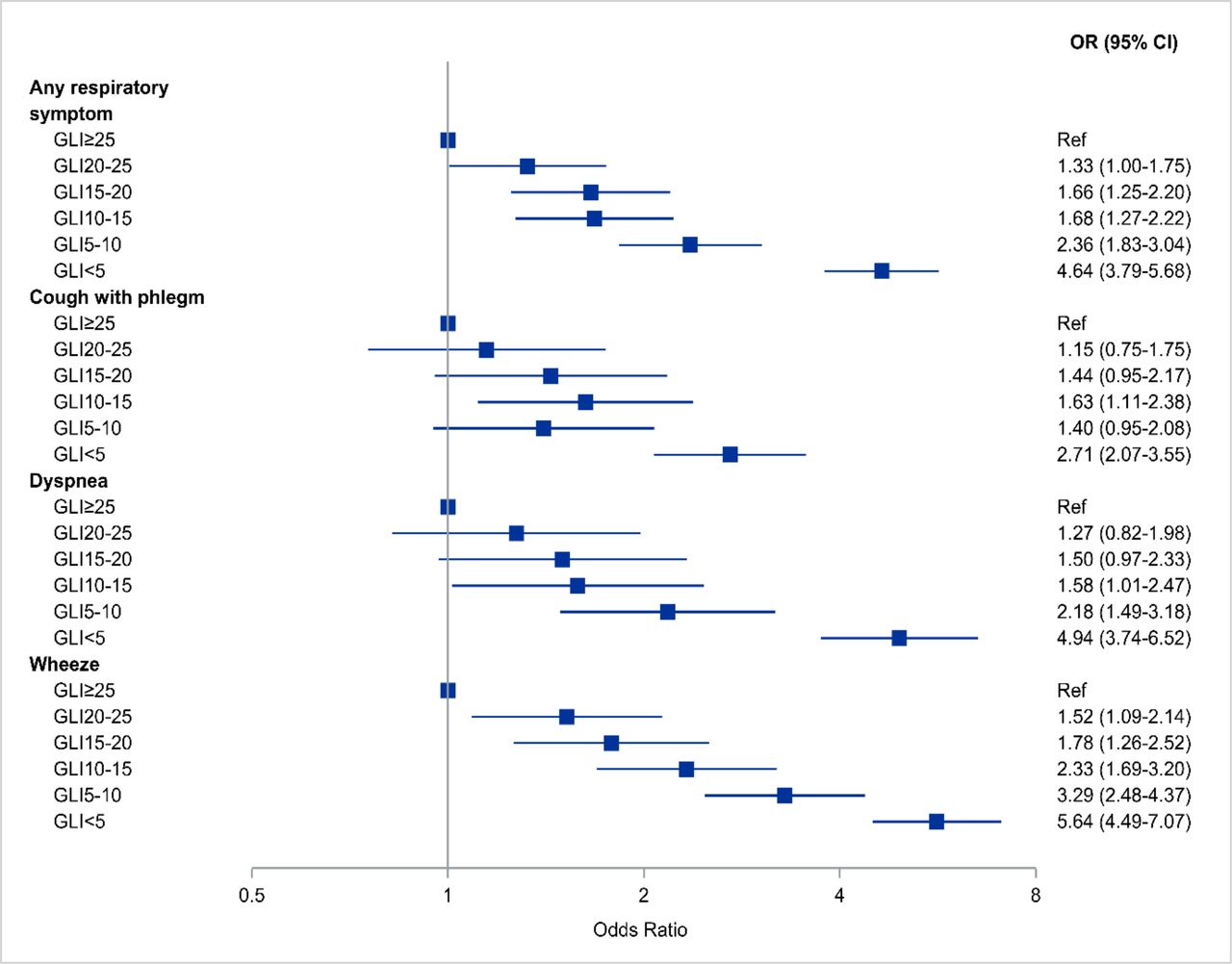
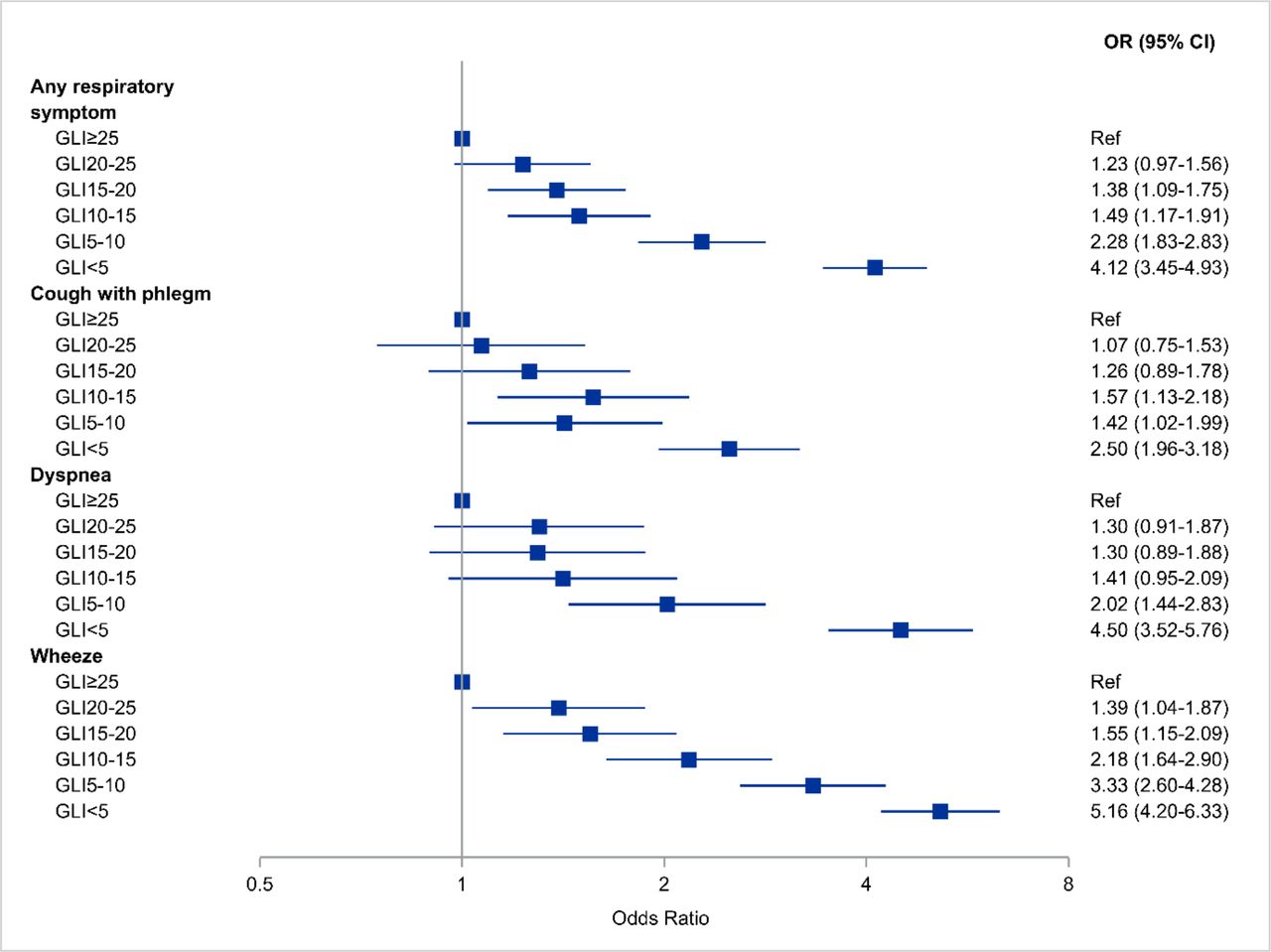
Figures 1 and 2 show the forest plots of OR for any respiratory symptom for never-smokers and ever-smokers stratified according to the GLI strata for the FEV1:FVC ratio, using GLI≥25 as the reference category. In never-smokers (figure 1), any respiratory symptom was significantly elevated in GLI<5 (OR 3.57, 95% CI 2.43 to 5.23) and in the stratum GLI5–10 (OR 2.57, 95% CI 1.69 to 3.91). Among ever-smokers (figure 2), any respiratory symptom was significantly increased in all five strata from GLI<5 to GLI20–25.

Forest plot of OR among never-smokers for any respiratory symptom, cough with phlegm, dyspnoea or wheezing according to GLI-based lower limit of normal for FEV1:FVC ratio at successively higher percentiles. All models are adjusted for age, sex, body mass index and asthma. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GLI, Global Lung Function Initiative; ref, reference.
Forest plot of OR among ever-smokers for any respiratory symptom, cough with phlegm, dyspnoea or wheezing according to GLI-based lower limit of normal for FEV1:FVC ratio at successively higher percentiles. All models are adjusted for age, sex, body mass index, asthma, smoking and pack-years. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GLI, Global Lung Function Initiative; ref, reference.
For the secondary outcomes, the separate symptoms, the results were somewhat different. Among never-smokers (figure 1), cough with phlegm and dyspnoea were only increased in the lowest strata (GLI<5), but wheezing was increased up to GLI10–15. Among ever-smokers (figure 2), cough with phlegm, dyspnoea and wheezing were elevated up to GLI10–15, and wheezing was increased even in the GLI15–20 strata.
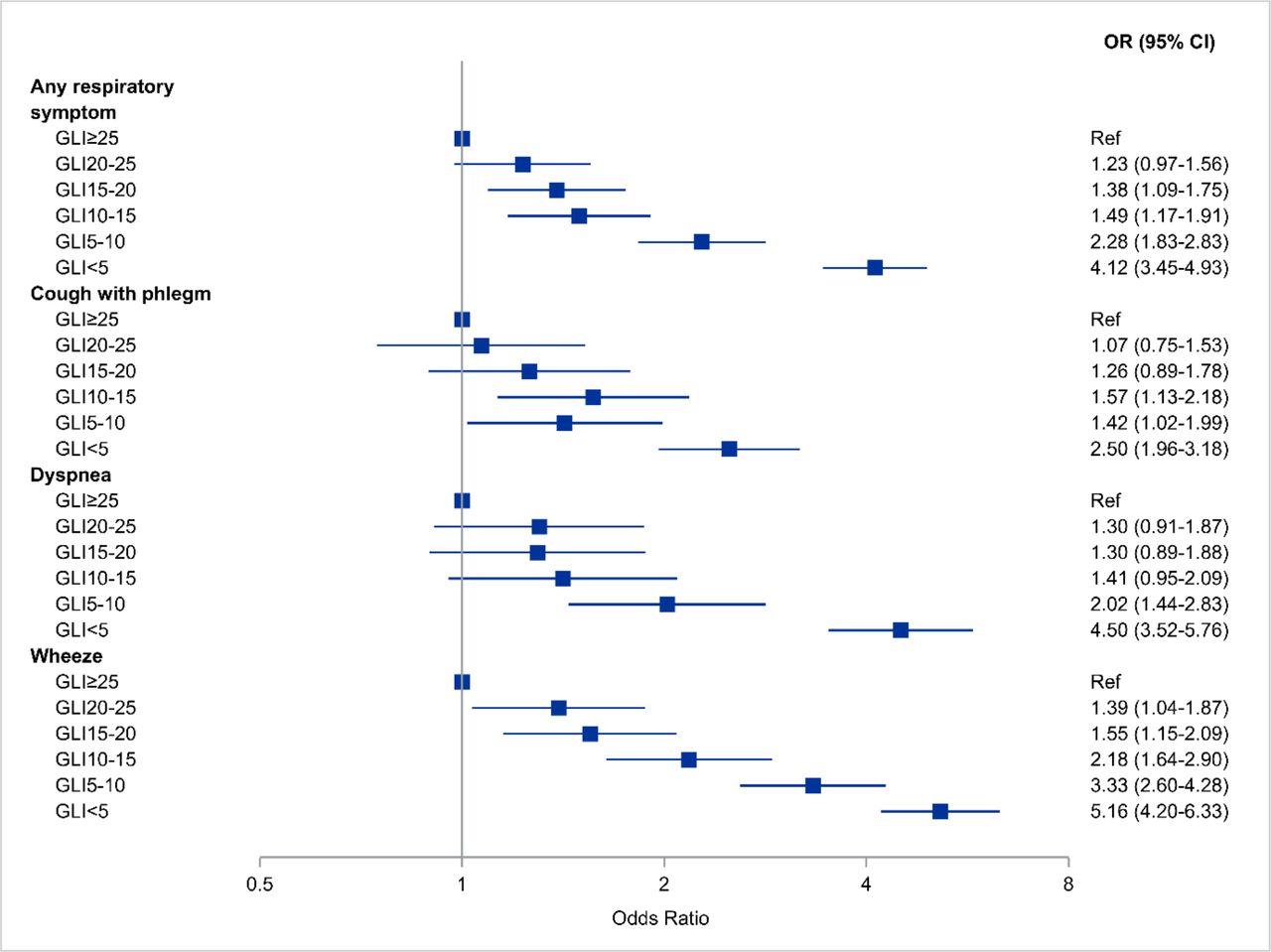
In figure 3 the results are shown for all subjects, regardless of smoking habits. The odds of any respiratory symptom were elevated up to the GLI15–20 strata, with less clear results for the separate symptoms of cough with phlegm, dyspnoea and wheezing.
Forest plot of OR among all subjects for any respiratory symptom, cough with phlegm, dyspnoea or wheezing according to GLI-based lower limit of normal for FEV1:FVC ratio at successively higher percentiles. All models are adjusted for age, sex, body mass index, asthma, smoking and pack-years. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GLI, Global Lung Function Initiative; ref, reference.
A sensitivity analysis was performed excluding all individuals with RSP (data not presented). The results were almost similar for any respiratory symptom and the separate symptoms of cough with phlegm, dyspnoea and wheezing.
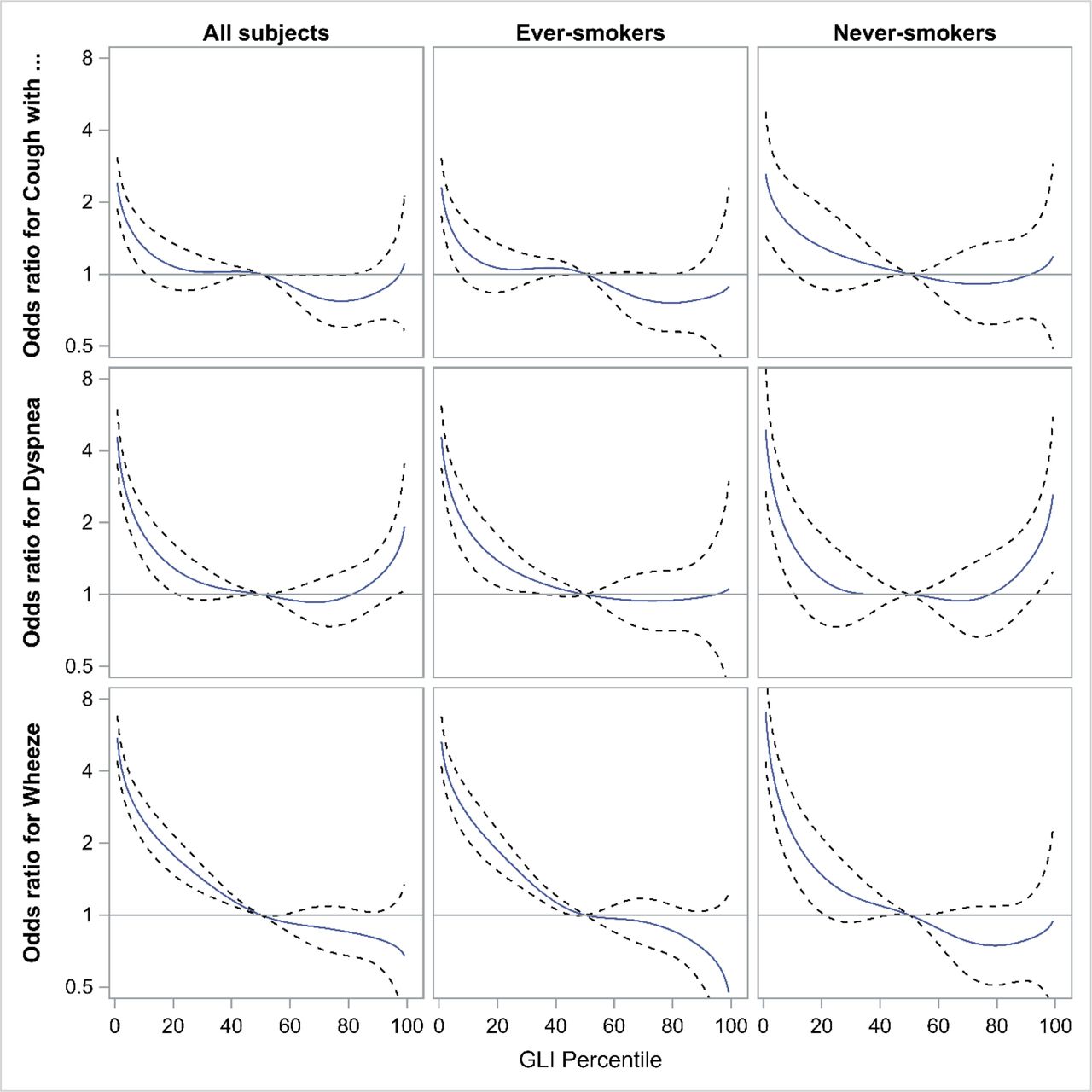
In an additional approach, we plotted the ORs for any respiratory symptom and the different symptoms of cough with phlegm, dyspnoea and wheezing in relation to GLI percentiles for never-smokers, ever-smokers and all subjects using GLI50 as the reference point (figures 4–6). The odds of any respiratory symptom continuously decreased with increasing GLI percentiles and flattened out towards unity at around GLI50. At higher percentiles the CIs were very wide. The results were similar for cough with phlegm, dyspnoea and wheezing. At higher GLI percentiles the odds of dyspnoea increased among never-smokers and among all subjects (figure 6).

OR from multivariable logistic regression models for any respiratory symptom among never-smokers and ever-smokers in relation to FEV1:FVC ratio at successively higher percentiles. We used the GLI reference equations with the 50th percentile as the reference point. All models are adjusted for age, sex, body mass index and asthma, and models for ever-smokers are also adjusted for smoking and pack-years. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GLI, Global Lung Function Initiative.
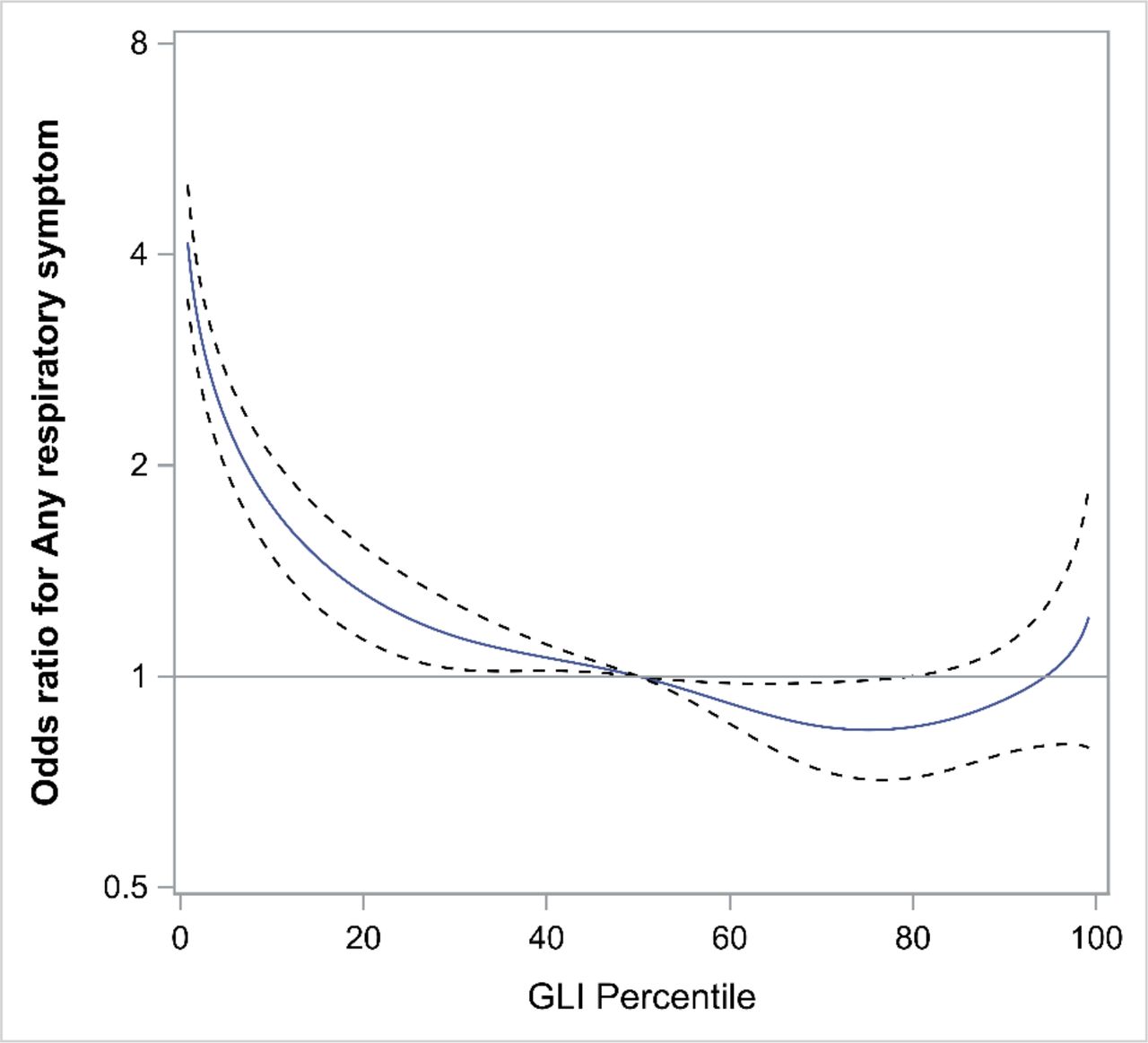
OR from multivariable logistic regression models for any respiratory symptom among all subjects in relation to FEV1:FVC ratio at successively higher percentiles. We used the GLI reference equations with the 50th percentile as the reference point. All models are adjusted for age, sex, body mass index, asthma, smoking and pack-years. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GLI, Global Lung Function Initiative.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
OR from multivariable logistic regression models for cough with phlegm, dyspnoea and wheezing among all subjects, never-smokers and ever-smokers in relation to the FEV1:FVC ratio at successively higher percentiles. We used the GLI reference equations with the 50th percentile as the reference point. All models are adjusted for age, sex, body mass index and asthma, and models for ever-smokers are also adjusted for smoking and pack-years. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GLI, Global Lung Function Initiative.
In a sensitivity analysis, we excluded all individuals with FVC below the 10th percentile, that is, individuals with low FVC. This resulted in a curve that flattened out after GLI50, similar to the other symptoms (data not shown). There was no obvious difference between never-smokers and ever-smokers regarding the shapes of the curves.
In an additional analysis we did not adjust for current smoking and the results were similar to previous analysis (see online supplementary file for details).
Supplemental material
Discussion
In the current paper, we describe substantial and important differences in the associations between CAL and respiratory symptoms depending on smoking history. Among never-smokers, we found support for a percentile cut-off of 10 rather than 5 when analysing increasing percentiles of FEV1:FVC in relation to the odds of COPD-related respiratory symptoms. In ever-smokers, the results indicated even higher percentile cut-offs, showing a notable difference between never-smokers and ever-smokers. Our results provide new data and may have important implications for how we in the future should define COPD. Important limitations of the study are the cross-sectional design and the lack of direct comparisons with the fixed ratio of FEV1:FVC.
For decades, the diagnosis of COPD has been based on the presence of CAL (after bronchodilation). The use of FEV1:FVC <0.7 has been advocated in previous and more recent guidelines, either using the fixed ratio or as LLN.23 It has also since long been recognised that individuals with FEV1:FVC ≥0.7 have increased prevalence of cough with phlegm and dyspnoea. This group was previously labelled as GOLD stage 0, as they were regarded as a high-risk group among smokers to develop COPD.24 In recent GOLD recommendations, stage 0 is not included as there was insufficient evidence to conclude that this group had an increased risk to progress to COPD.25 However, there are a number of studies indicating that smokers with normal spirometry and respiratory symptoms may have evidence of airway disease and an increased risk for COPD.3 25–28 It has been proposed that these individuals may have early COPD yet without CAL.25
There is lack of data among never-smokers, but in the analyses of the Copenhagen General Population Study the presence of respiratory symptoms among never-smokers with normal lung function, defined as FEV1:FVC ≥0.7, predicted COPD exacerbations and pneumonia hospitalisations in individuals with up to 15 years of follow-up data.4 Further, COPD in never-smokers was associated with an increased morbidity due to lung-related hospitalisations, despite a lower mortality compared with smokers with COPD.29 Our results add evidence to this discussion, as we show that never-smokers (and ever-smokers) with FEV1:FVC >GLI5 have increased odds of respiratory symptoms. We are fully aware that our results are based on cross-sectional data; however, our results still add evidence to the discussion whether the criteria for COPD or defining a population at risk for COPD should be revised, by for instance using a higher percentile instead of the fifth percentile.
We also analysed cough with phlegm, dyspnoea and wheezing and found that the odds of cough with phlegm and dyspnoea were increased up to GLI5–10 among never-smokers; however, the CIs included unity. The odds of cough with phlegm and dyspnoea were clearly increased up to GLI10–15 among ever-smokers. The odds of wheezing were increased even in the higher strata. The increased odds of wheezing, also at higher thresholds, probably reflect that wheezing also occurs among individuals with normal lung function, for instance in those with mild asthma. Given that we performed spirometry after bronchodilation, we minimised the risk of including individuals with asthma with reversible airflow limitation. Also, we adjusted in our models for self-reported asthma. Furthermore, chronic bronchitis may be associated with wheezing without necessarily being associated with significant CAL.
We extended the analysis and plotted the odds of any respiratory symptom, but also cough with phlegm, dyspnoea and wheezing and using GLI50 as the anchor point. Here, we observed that the odds of respiratory symptoms continuously decreased the higher the GLI percentiles, and flattened out towards unity at a level close to GLI50. At higher levels the CIs were very wide. The main conclusion from this analysis is that whether increased odds in a stratum would be significant or not will depend on the sample size. Since all the information of the GLI z-score is used in these analyses, unlike the categorical analyses (in figures 1–3), a higher statistical power is expected.
Of note is that individuals with dyspnoea showed a different pattern. At high GLI percentiles, the odds increased, which means that subjects with high FEV1:FVC ratio, that is, individuals with low FVC, also have increased prevalence of dyspnoea. In a sensitivity analysis, we excluded all individuals with FVC under the 10th percentile, which resulted in a curve that flattened out after GLI50, similar to the other symptoms.
The use of the LMS method for assessing the percentiles has a strong methodological support. The main advantage is that it accounts for the age-related increase in airflow limitation, as well as the variability and normality deviations among the reference materials.8–10 Importantly, our analyses have a similar design as previous research, and our results among never-smokers are in line with previous results.9 However, when analysing the whole population and plotting the ORs, we obtained a smooth function without obvious thresholds. This fact lends further support to the idea that the decided level for an operational definition of COPD should be a decision based both on clinical and epidemiological evidence.30
We used a cross-sectional sample and based our analyses on the most important respiratory symptoms. Symptoms may be more sensitive to reporting bias compared with the more definitive outcome of mortality. On the other hand, respiratory symptoms reflect the individual’s perceived health status, and respiratory symptoms are closely linked to exacerbations, disability and healthcare consumption.15 31 Mortality is doubtless a clinically relevant outcome, and we have recently shown that there is no difference in cause-specific mortality for the GOLD and the ATS/ERS definitions.6 A similar analysis should be performed when it comes to different GLI thresholds. However, all-cause mortality has been shown to be increased using LLN5 as a threshold with the LMS method.9
We are fully aware of the weaknesses of the present study. As previously commented, it is a cross-sectional study, which limits the validity of the conclusions. The study was performed within a narrow age range, namely 50–64 years, limiting the external validity to that age interval. Moreover, selection bias may be a problem, as the participation rate was around 50%. In the current study population, having COPD and cardiovascular disease seems to have increased the participation rate.32 This may have increased the prevalence of individuals with symptoms and CAL in the examined population. The prevalence of ever-smokers, 53%, is also slightly higher in our sample compared with other general population studies.33 The latter suggests that there might be some selection bias in relation to smoking habits. However, our main results are based on analyses of never-smokers, a group with lesser risk for COPD and cardiovascular diseases. Hence, we conclude that despite the possibility of a selection bias in our study, we suggest that the threshold values obtained among never-smokers would only have been marginally affected.
Our study also has evident strengths. We used a large general population-based sample comprising ever-smokers as well as lifelong never-smokers. This is an advantage as there is a need for data from never-smoking general population-based samples. Furthermore, spirometry was performed after bronchodilator administration to assess true CAL. Importantly, when comparing the obtained prevalence figures with results from other studies, it should be considered that many of them used prebronchodilator values, and prebronchodilator values may misclassify and overestimate the prevalence of CALGOLD.34
In conclusion, a substantial and clinically important difference was found between never-smokers and ever-smokers with regard to COPD-related respiratory symptoms. When using GLI≥25 as the reference category, our results seem to support a percentile cut-off of 10 for percentiles of FEV1:FVC among never-smokers and an even higher percentile for ever-smokers. Of importance, the relation between different percentiles of FEV1:FVC and the different symptoms was a smooth function without obvious thresholds.
References
Footnotes
Contributors The following are members of SCAPIS National Steering Committee and therefore responsible for design, funding, planning and execution of SCAPIS: AB, GB, JE, CMS, KT, CJÖ and EL. Responsible for the conception and design of the analyses included in the specific manuscript and first draft: KT, LS, AL and AM. Data collection: AA, AFB, KC, ME, VH, CJ, ÅJ, DK, AL, HLP, CMS, JES, HAT, JV and PW. Statistical analysis: LS. All authors were involved in the planning and data interpretation and revision of manuscript drafts for important intellectual content, and approval of the version to be submitted.
Funding The main funding body of the Swedish CArdioPulmonary bioImage Study (SCAPIS) is the Swedish Heart and Lung Foundation. The study is also funded by the Knut and Alice Wallenberg Foundation, the Swedish Research Council and VINNOVA (Sweden’s innovation agency), the University of Gothenburg and Sahlgrenska University Hospital, Karolinska Institutet and Karolinska University Hospital, Linköping University and University Hospital, Lund University and Skåne University Hospital, Umeå University and University Hospital, and Uppsala University and University Hospital. There was also individual research support from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement.
Competing interests AA reports personal fees from Novartis and AstraZeneca, outside this work. AL reports personal fees from Boehringer Ingelheim, AstraZeneca, Novartis and Active Care, outside the submitted work. JV reports personal fees from Boehringer Ingelheim, outside the submitted work. PW reports personal fees from AstraZeneca and Chiesi Pharmaceuticals, outside the submitted work. CMS reports personal fees from Boehringer Ingelheim, GlaxoSmithKline, Novartis, AstraZeneca, Roche and Genzyme, outside the submitted work. PW has a patent device and method for pulmonary capacity measurements issued. MS reports personal fees from AstraZeneca, outside the submitted work.
Patient consent for publication Not required.
Ethics approval The study was approved by the Regional Ethical Review Board at Umeå University (nr: 2010- 228-31 M), and all participants provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. A prerequisite is an approval from a Swedish ethical board.