Article Text

Abstract
Objectives While there is an extensive body of literature surrounding the decision to insert, and methods for inserting, a tracheostomy, the optimal management of tracheostomies within the intensive care unit (ICU) from after insertion until ICU discharge is not well understood. The objective was to identify and map the key concepts relating to, and identify research priorities for, postinsertion management of adult patients with tracheostomies in the ICU.
Design Scoping review of the literature.
Data sources PubMed, Embase and Cumulative Index to Nursing and Allied Health Literature were searched from inception to 3 October 2019. Additional sources were searched for published and unpublished literature.
Eligibility criteria We included studies of any methodology that addressed the a priori key questions relating to tracheostomy management in the ICU. No restrictions were placed on language or year of publication.
Data extraction and synthesis Titles and abstracts were screened by two reviewers. Studies that met inclusion criteria were reviewed in full by two reviewers, with discrepancies resolved by a third. Data were extracted for included studies, and results mapped along the prespecified research questions.
Results 6132 articles were screened, and 102 articles were included for detailed analysis. Protocolised weaning was found to be successful in liberating patients from the ventilator in several cohort studies. Observational studies showed that strategies that use T-pieces and high-flow oxygen delivery improve weaning success. Several lines of evidence, including one clinical trial, support early cuff deflation as a safe and effective strategy as it results in a reduced time to wean, shorter ICU stays and fewer complications. Early tracheostomy downsizing and/or switching to cuffless tubes was found to be of benefit in one study. A substantial body of evidence supports the use of speaking valves to facilitate communication. While this does not influence time to wean or incidence of complications, it is associated with a major benefit in patient satisfaction and experience. Use of care bundles and multidisciplinary team approaches have been associated with reduced complications and improved outcomes in several observational studies.
Conclusions The limited body of evidence supports use of weaning protocols, early cuff deflation, use of speaking valves and multidisciplinary approaches. Clinical trials examining post-tracheostomy management strategies in ICUs are a priority.
- not applicable
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
What evidence exists regarding postinsertion tracheostomy management in the ICU, and where are the gaps in the evidence?
What is the bottom line?
There is a lack of quality research on this topic, with significant variations in practice primarily driven by clinician experience and local preferences.
Why read on?
This review scopes and summarises all available literature on this topic and identifies priority areas for future studies regarding tracheostomy management.
Tracheostomy is performed in approximately 10%–15% of patients who are admitted to intensive care units (ICU).1 This procedure, which involves either percutaneous or surgical placement of a tube across the anterior neck into the airway, may be indicated for relief of airway obstruction, facilitation of pulmonary toilet and for facilitation of wean from mechanical ventilation.2 In addition, tracheostomy may allow a reduction of sedation, improve patient safety and comfort, and reduce overall costs of care.3 4 There is a vast body of literature published on the indications, timing and technique of tracheostomy insertion, including several meta-analyses.5–9 Likewise, there are a number of systematic reviews, surveys and expert guidelines on the timing and act of decannulation, or removal of the tracheostomy.10 11
While there is extensive research on tracheostomy insertion and decannulation, their optimal management in ICUs between the time of insertion and ICU discharge has received little attention. Management aspects such as optimal cuff management, tracheostomy changes or downsizing, and weaning approaches are typically directed by individual expertise, anecdotal experience and local preferences.
The objective of this study was to conduct a scoping review to systematically explore and map the key concepts and gaps in the literature, in order to identify research priorities relating to the management of intensive care patients with tracheostomies from after insertion of the tracheostomy to the time of ICU discharge. Scoping reviews are used to determine the scope or coverage of a body of literature on an emerging topic and aims to identify and map the available evidence to provide an overview that may guide further research.12 13 While a systematic review can answer a single precise question to inform clinical practice, a scoping review addresses the extent, range and nature of the evidence, and identifies common concepts or gaps. Given the limited volume and heterogeneous nature of the literature published on this topic, the scoping review methodology was most suited to the objectives of this review. It is our hope that this review may subsequently guide future high-level research, such as clinical trials and systematic reviews to answer more precise questions and address research priorities that have been identified.
Methods
The study protocol was established a priori and was developed as outlined by the members of the Joanna Briggs Institute and members of the Joanna Briggs Collaborating Centres.12 The specific research questions were, ‘What evidence exists regarding the ideal strategies to:
liberate patients from the ventilator?
manage cuff inflation and deflation?
manage tracheostomy change and revision?
optimise speech and communication?
optimise swallowing and oral intake?’
Eligibility criteria
Studies of any methodology that addressed one or more of the research questions were considered. Clinical studies were selected for inclusion if:
the study subjects were adults (age ≥18 years) admitted to medical, general surgical or specialty surgical ICUs;
a tracheostomy was inserted during the current hospital admission;
the study related to a period after insertion of the tracheostomy and prior to ICU discharge; and
the subjects had respiratory failure requiring mechanical ventilation.
Studies that met all inclusion criteria but did not address one of the prespecified research questions were included. This approach was taken to enable this review to address concepts that emerged during the review and had not previously been considered.
Studies that focused on patients who had chronic tracheostomies or who had a tracheostomy placed prior to ICU admission for reasons other than for acute respiratory failure (eg, elective upper airway surgery) were excluded. Studies that focused on the indications for, timing of, and performance of the tracheostomy insertion procedure were excluded. Studies that did not involve patients as subjects (eg, studies relating to medical devices not tested in a live patient population) were only included if they addressed research questions relevant to the patient population in the inclusion criteria. Review articles and editorials that did not contain novel information were excluded.
Search methodology
An initial electronic search was conducted of three key databases (PubMed, Embase and Cumulative Index to Nursing and Allied Health Literature) from inception through to 3 October 2019. The keywords used were “ICU” or “intensive care unit” and “tracheostomy”. The study strategy is available in as an electronic supplement (e-supplementary file 1) The search was not limited by design, language or year of study. The reference lists of included articles, review articles and editorials were searched for additional potential studies.
Supplemental material
Titles and abstracts were screened independently by two authors (KAW and KBL) for potential inclusion. Articles that met inclusion criteria based on title and abstract review were included for full text review. Full-text articles were retrieved and reviewed independently by two authors (KAW and SCT) to assess whether they met the inclusion criteria. Discrepancies between the two reviewers were resolved by a third. Following the compilation of a list of articles for inclusion, data were extracted by one of the authors (KAW), discussed and reviewed by all authors, and results mapped along the prespecified research questions. Data extracted included first author’s surname, year of publication, setting, country of origin, aims or objectives, study population and size (if applicable), study design, duration of intervention (if applicable) and key findings. Analysis was descriptive.
Patient and public involvement
This review includes studies that consider the patient experience of tracheostomy management in the intensive care, including qualitative or phenomenological studies. Patients and the public were not involved in the completion of this review.
Results
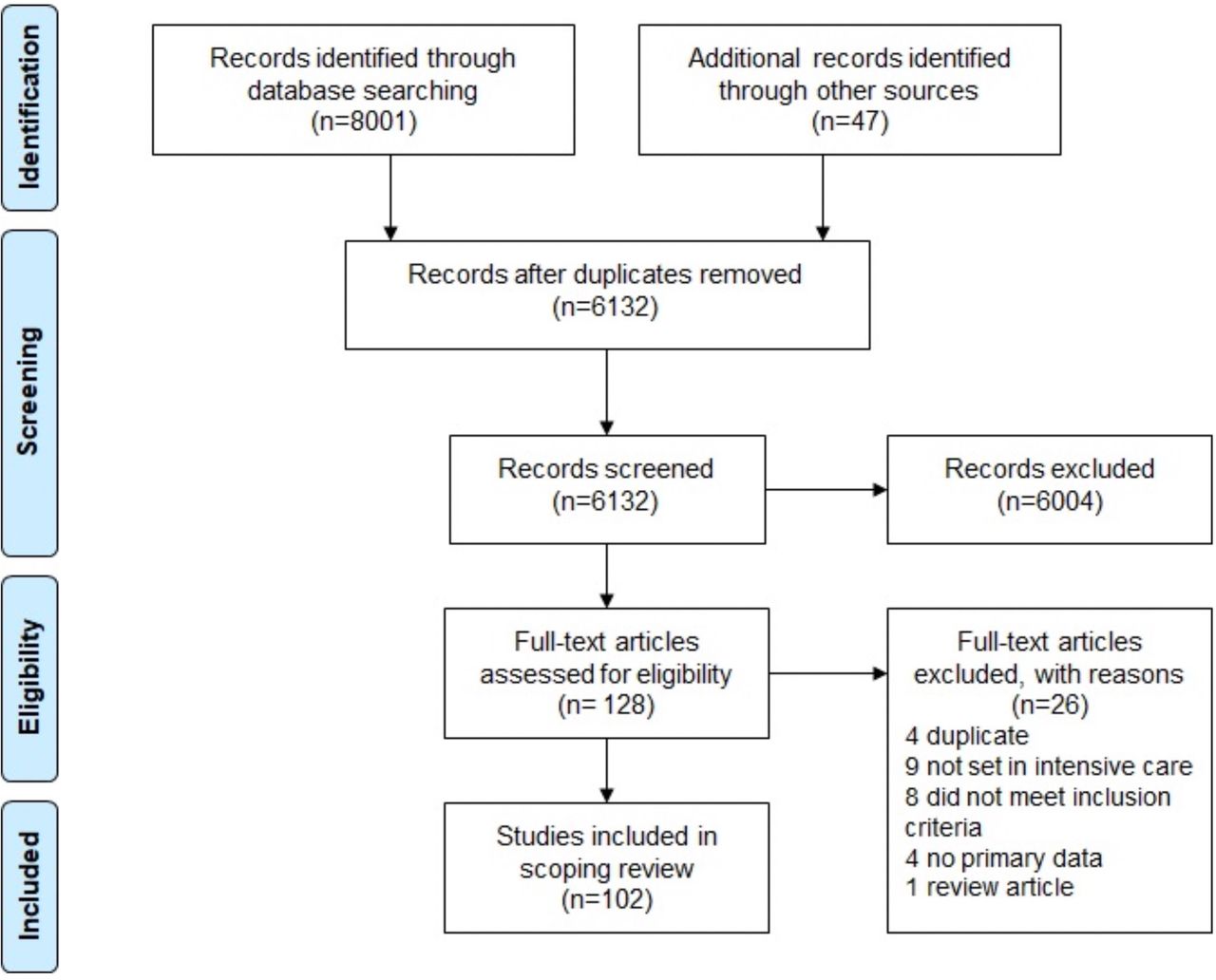
Electronic searches conducted retrieved 8801 citations across the PubMed (2198), Embase (5805) and Cumulative Index to Nursing and Allied Health Literature (798) databases. An additional 47 citations were identified from other sources, including from hand-searched reference lists, guidelines and resources published by professional bodies, online searches and conference abstracts. Following the removal of duplicates and the application of study inclusion and exclusion criteria, 102 articles were included in the final review, as detailed in figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for study identification and inclusion.
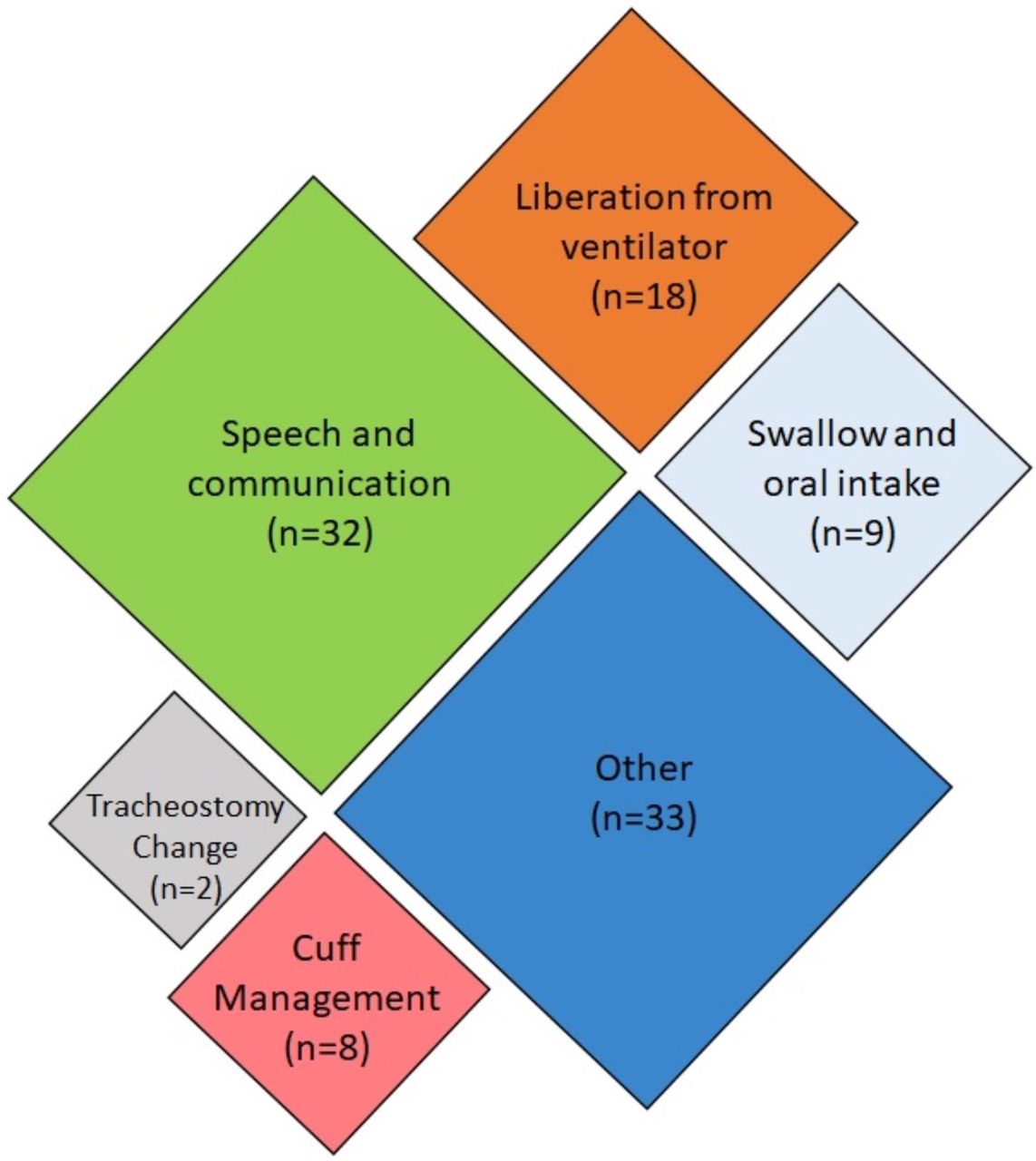
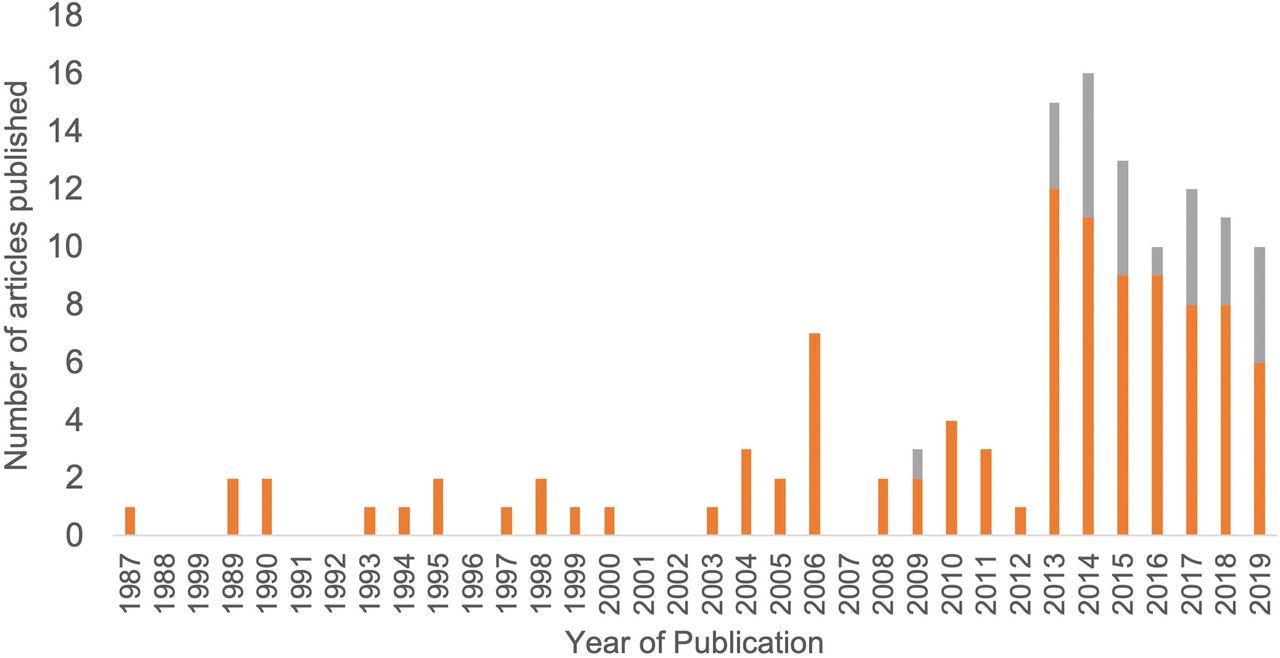
Of the 102 articles included, 25 were only available as abstracts published in conference proceedings. Given that the objective of this review was to map all available evidence, these abstracts were included. Care should be taken in the interpretation of such results; therefore, abstract-only publications have been noted as such throughout this review. Articles included in this review were published between 1987 and 2019, with the majority published since 2013, as shown in figure 2. Studies were conducted in 21 different countries, with the most common being the USA (n=22), the UK (n=16) and Australia (n=15). The remaining 48 studies originated from Europe (n=31), Asia (n=7), South America (n=5), Africa (n=2) and North America (n=1). The country of origin was not specified in three cases. Most (n=69) of the identified articles addressed one or more of the five research questions, as mapped in figure 3. Studies that addressed more than one key question were categorised based on the question that was most extensively addressed. Thirty-three articles addressed other topics and have been included in a separate ‘Other’ category. The results of the studies are summarised in the electronic supplement e-supplementary file 2. The key findings, categorised by theme, have been summarised in table 1.
Supplemental material
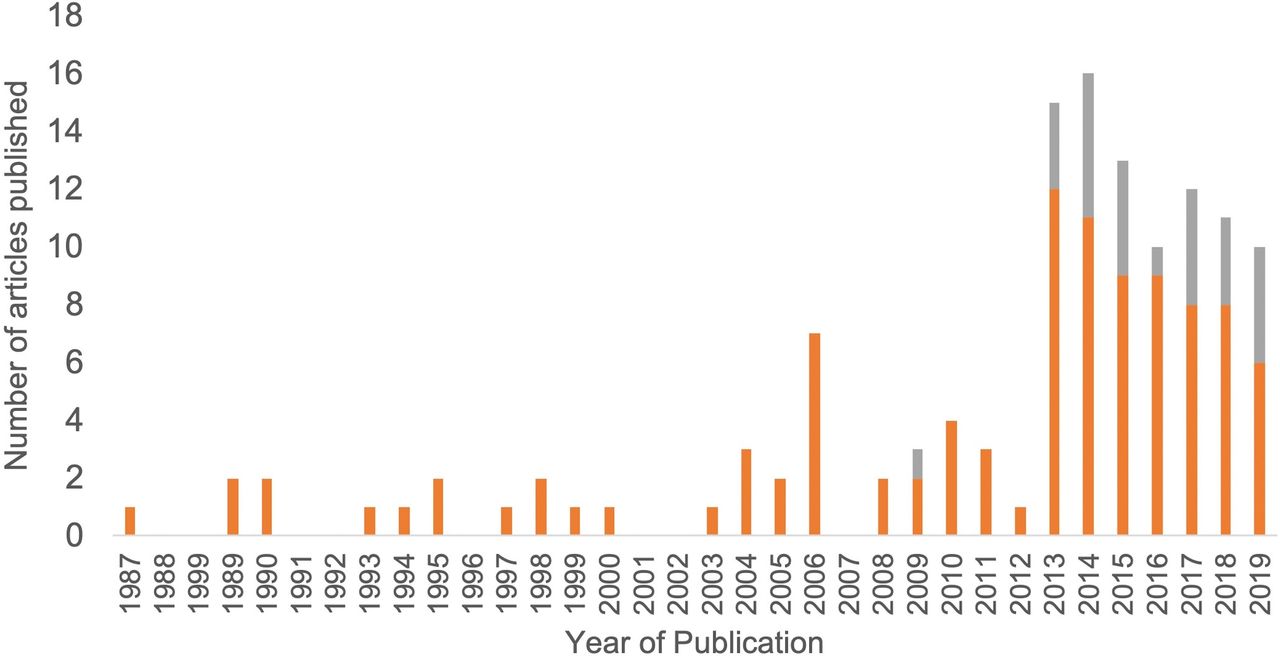
Annual publications investigating postinsertion tracheostomy management strategies for patients admitted to intensive care units.
{kind=link}
{kind=link}
{kind=link}
Mapping of included articles based on key research question addressed.
Key findings
Liberation from ventilator
Twenty studies investigated topics related to weaning from mechanical ventilation. Five studies compared protocolised weaning models and reported successful weaning in 77%–89% of patients. Those studies reported that the use of protocols resulted in no difference in the time to weaning, length of stay, rates of emergent reintubation or readmission to the ICU.14–18 Two studies addressed nurse-led and protocolised weaning. One randomised trial compared nurse-led protocolised weaning and physician-led weaning, and found that patients were more likely to be weaned prior to ICU discharge in the nurse-led group (77% protocolised vs 45% physician led, p=0.031).14 16 A prospective study involving 192 patients found that there was no difference in weaning outcomes when medical management was provided by an attending physician and either a unit-based nurse practitioner, or a critical care rotational fellow.16
Three studies evaluated predictors of successful weaning outcomes or decannulation. Two studies found that weaning or decannulation success was more likely in patients that were able to increase the force-generating capacity of the diaphragm.19 20 An observational study of 49 patients found that the ability to generate peak cough flows of greater than 160 L/min was predictive of successful decannulation.19 In a retrospective audit of 129 patients in a Dutch medical-surgical ICU, patients whose primary pathology was neurosurgical or cardiopulmonary were statistically more likely to have shorter weaning times (3–7 days) when compared with medical (9 days) or surgical (8 days) patients.17
An observational study of 25 patients compared T-piece ventilation and continuous positive pressure ventilation during weaning and found that T-piece ventilation resulted in improved arterial and central venous oxygenation.21 One letter reported that configuring the mixing tube between the T-piece and Venturi mask connector improved oxygenation.22 Three articles, including a case report and an abstract, discussed the use of high-flow oxygen during weaning.23–25 One of these studies, a randomised cross-over trial, found that during cuff deflation, the use of high-flow oxygen improved oxygenation when compared with T-piece ventilation alone (p<0.02).23 Two studies evaluated different types of humidification systems and concluded that heat-moisture-exchange systems and heated humidifiers provided adequate humidification, and that cold humidifiers provided inadequate humidification in 50% of patients.26 27
Two studies addressed aspects of respiratory physiology during weaning. A clinical trial of 10 patients found that tracheostomy tube-related additional work of breathing was highest in continuous positive airway pressure and was reduced most effectively in automatic tube compensation mode.28 An observational study of 24 patients found that the dead-space and airway resistance of tracheostomy tubes were comparable to endotracheal tubes, contrary to common perception.29
Management of the cuff
Eight studies addressed issues related to cuff inflation management. One was an anecdotal case series30 and another was an abstract aimed at optimising adherence to cuff inflation pressures between 20 mm Hg and 30 mm Hg.31 Three studies investigated the impact of cuff deflation on respiratory parameters during positive pressure ventilation or weaning.32–34 One measured airway pressure in 16 patients and found clinically insignificant decreases in end-expiratory pressure with cuff deflation; however, all patients could vocalise and three quarters (n=12) could swallow effectively.32 In a report of a series of long-term wean patients, most (99/104; 95%) were found to be managed safely with either deflated cuffs or cuffless tubes.33 Another investigation with T-piece trials among 13 patients found that diaphragmatic effort was significantly lower with cuff deflation as compared with inflation.34
One retrospective review of 113 patients found that 95% (n=107) of patients tolerated cuff deflation on first attempt and that clinical stability and aspirated above-cuff secretions≤1 mL/h were highly predictive of success.35 Another retrospective audit found that among 30 patients, use of an early cuff deflation strategy resulted in a decreased ICU length of stay (28 vs 45 days) and mean number of tracheostomy days (16 vs 38) compared with historical controls.36 Hernandez et al conducted a clinical trial comparing cuff deflation and inflation during spontaneous breathing trials.37 They found that cuff deflation resulted in a significantly shorter wean time (3 vs 8 days, p<0.01) with an associated significantly lower incidence of respiratory infection (20 vs 36%, p=0.02).
Tracheostomy change and revision
Two studies investigated tracheostomy changes or revision. In an observational study of 130 stable respiratory care unit patients, tracheostomy changes before 7 days were associated with earlier liberation from the ventilator (2.2 vs 3.9 days), use of speaking valves (7 vs 12 days), oral intake (10 vs 20 days) and discharge from the ICU (11 vs 17 days).38 It may be argued that this population is more likely to have a better prognosis and that outcomes may not be directly related to early tracheostomy change. A survey of Dutch ICUs found that 59% of units (n=26) did not routinely change the tracheostomy.39 One phenomenological study explored the patient experience of tracheostomy changes, and identified four key themes including physical sensation, psychological preparation, essentialness of communication and trust and competence.40
Optimisation of speech and communication
Twenty-eight articles investigated the optimisation of speech and communication. One-way speaking valves are widely used and were found to safely achieve successful phonation in most patients who were fit for cuff deflation, with adverse effects rare.41 A 1993 prospective study found that one-way speaking valves can be used to facilitate communication during positive pressure ventilation; however, this method has largely been superseded by newer adjuncts.42
Studies suggest that in-line speaking valves can significantly hasten time to phonation in patients who are unable to tolerate cuff deflation.43–45 A randomised clinical trial of 30 ventilated patients found that, compared with cuff deflation with one-way speaking valves, early speech interventions with in-line speaking valves reduced time to phonation (7 vs 18 days, p=0.001), with no increase in time to decannulation, time of ventilation, length of stay or adverse events.44 Further, Sutt et al used electrical impedance tomography to demonstrate that in-line speaking valves can improve gas distribution and alveolar recruitment.46
There were mixed findings on the role of fenestrated tubes; however, both studies that considered this topic were low-quality evidence studies including one abstract.47 48
Several studies evaluated tracheostomy ‘talk tubes’.49–53 In those studies, 90%–100% of patients were able to achieve phonation, with 78%–100% adequately intelligible for effective communication.49–53 Excessive secretions and cough were the most common adverse effects.49–51 There was no demonstrated significant air leak when using the devices, even at higher pressures, and no mucosal injuries on bronchoscopy.50 An interventional study of 20 patients found that patients using Portex ‘Talk’ tubes had shorter time to phonation compared with Communi-Trach I tubes (2.1 vs 5.6 days, p<0.001).52
A feasibility study of above-cuff vocalisation involving 10 patients found that this technique resulted in phonation in eight patients, with 72% (66/91) of attempts resulting in audible speech.45
Three articles addressed the use of augmentative and alternative communication devices, with all finding statistically significant improvements in a patient’s ability to communicate. One prospective pilot study involving 12 patients found 50% (n=6) reported frustration with the use of these devices.54 Two studies also included communication skills training of doctors and nurses caring for patients uses the devices, and found this resulted in significant improvements in their ability to communicate with patients.55 56
Eight studies evaluated patient experience or quality of life relating to speech or communication. The participants highlighted that feelings of powerlessness, being misunderstood and physical discomfort impacted on their quality of life. Patients also acknowledged the importance of non-verbal communication.57–59 One study interviewed both patients and nurses and identified mutual experiences of frustration and powerlessness attributable to communication difficulties.59 One randomised controlled trial used talk tubes and found significant improvements in voice-related quality of life.53 Another used in-line speaking valves and favoured the use of in-line valves over one-way speaking valve but found that the improvement in quality of life was not statistically significant.44
Optimisation of swallow
Nine studies considered the optimisation of swallowing and oral intake. The incidence of swallowing dysfunction in tracheostomised patients has been reported as between 30% and 70%; however, several factors can increase this risk, including pre-existing swallowing impairment, neurological disorders, age, sedation and hypercarbia.60–63 In a study excluding patients with neurological disorders, 38% (15/40) had swallowing dysfunction, suggesting that previous studies may have overestimated incidence based on this patient group.62
Two Australian studies found almost 80% of tracheostomised patients were seen by speech-language pathologists.60 64 While the majority (86%; 108/126) of patients will commence oral intake with a tracheostomy in situ, only 43% (54/126) of patients had commenced oral intake in the ICU.60 A prospective study of 14 patients evaluated a swallowing rehabilitation programme administered by speech-language pathologists and an otorhinolaryngologist.65 Ten of the 14 patients (71%) were able to receive oral intake, with 6 (42%) having complete resolution of dysphagia, and 2 (14%) experiencing partial improvement.
There are multiple methods for assessing swallow in the tracheostomised patient.64 One abstract found the Evans Blue Dye Test had a sensitivity of 84% and specificity of 100% when compared with fibreoptic endoscopic evaluation of swallow.66 A prospective study involving 35 patients found 12 patients (34%) had a swallowing abnormality on bedside assessment. Of those 12 patients, and a further 7 patients with a high index of suspicion, 83% had abnormal swallow on videofluoroscopy.63
Three studies considered specific elements of swallow physiology, including the impact of cuff pressure and subglottic insufflation, finding that increased cuff pressure influences both the sensory and motor components of the swallow reflex.67 68 A prospective cross-over randomised and physiological study of 16 patients investigated the impact of meals on respiratory mechanics.69 While there was a significant increase in respiratory rate, tidal volume and subjective dyspnoea, this was not associated with desaturation or cardiovascular instability.69
Other
Several articles were included that did not directly fit within the a priori themes according to the research questions posed.
Three articles addressed stomal care and complications, including the dressing choice, wound granulation and pressure injuries.70–72 The most common complications relating to stoma care in the acute phase are bleeding, infection and granulation; however, their incidence varies between sources from 4% to 40%.70 73 74 In an academic poster that assessed 23 possible risk factors for pressure injuries, percutaneous tracheostomy was the only factor that reached statistical significance in univariate analysis.71 A randomised trial found no difference in the incidence of stomal infection when using gauze dressings compared with absorbent foam (17.5% v 10%, p=0.051).70
Nine articles addressed the topic of tracheostomy bacterial colonisation, and tracheostomy-associated and ventilator-associated pneumonia. Oral care bundles with surveillance and auditing protocols were found to significantly reduce the incidence of tracheostomy-associated or ventilator-associated pneumonia.75 76 Studies also found that suction-above-the-cuff in tracheostomised patients reduced infection and microbial quantity.77–79 A randomised controlled trial (abstract) of 19 patients found the use of speaking valves during weaning reduced the incidence of nosocomial respiratory infection and may reduce time to decannulation.80
One cohort study (abstract) found that 89% (67/75) of tracheostomised patients in ICU reported trouble falling asleep.81 Studies found that sleep time and efficiency were poor, and that sleep time was not improved by melatonin (240 vs 243 min, p=0.68 for melatonin vs placebo).82 83 Patients ventilated with mechanical ventilation compared with spontaneously ventilating had a significantly longer total sleep time (183 vs 132 min, p=0.04); however, there was no improvement in rapid eye movement sleep or sleep fragmentation.83 An observational study found that after insertion of a tracheostomy, there was a significant reduction in sedative drug requirements and time spent ‘heavily sedated’ which was reduced from 7 hours per day to one.84
Four studies (including three abstracts) evaluated the impact of multidisciplinary tracheostomy teams, finding they resulted in reduced time to first oral intake, first tube change and decannulation, and reduced length of stay and complication rates.85–88 Reduced time to weaning and decannulation were noted in three of the four studies.85 87 88
Three studies including one abstract addressed quality of life or stressful experiences, with patients reporting that psychosocial discomfort, sleeplessness, physical symptoms of thirst and pain, fear and relationships had a significant impact on their experience.81 89 90
Four studies (including three abstracts) were observational audits,91–94 three (including two abstracts) surveyed participants’ knowledge on an aspect of tracheostomy care95–97 and two were surveys regarding standards of practice.39 98 There was one clinical consensus statement published by the American Academy of Otolaryngology-Head and Neck Surgery Foundation, using a Delphi process.99
Discussion
In this scoping review, we identified and explored five main themes related to the management of patients with a tracheostomy from time post insertion to ICU discharge. Despite slow-growing interest in this area, research remains limited. There were a significant number of low-quality studies and abstracts published only in conference proceedings without progression to peer-reviewed publication, and a lack of clinical trials.
Weaning from the ventilator is an integral part of practice in critical care medicine. In our review, we found that there is support for the use of protocols, including nurse-led protocols; that T-piece and high-flow oxygen delivery may be used during weaning to improve oxygenation; and that diaphragmatic strengthening may improve weaning success.21 23–25
Personal experience and anecdotal surveys of intensivists have revealed vast practice variation in cuff management both within and between countries.39 60 64 Some clinicians view cuff deflation as a late step in the weaning process, while others view cuff deflation, tube downsizing and exchange to cuffless tubes, as the standard practice. The former view may, in part, be related to an erroneous belief that cuff inflation during weaning reduces aspiration and associated pneumonia.60 61 100 The available evidence indicates that early cuff deflation is widely tolerated by patients during weaning, can be reliably predicted based on clinical assessment, facilitates speech and oral intake, reduces time to weaning and decannulation, and can reduce rates of respiratory infections.32–37 While data are limited, there is potential benefit from early tracheostomy downsizing or switching to cuffless tubes.38 60 88
There is a significant body of literature that supports the optimisation of speech and communication as it is important from a rehabilitative and psychoemotional point of view.44 53 57 101 Many of the strategies for enhancing communication that were considered in the included articles have been demonstrated as safe, simple to use and improving both communication and quality of life.43–46 58 102 Speech adjuncts, used alongside strategies for early cuff deflation, may lead to earlier weaning, fewer complications and improved patient experience, and may also lead to earlier oral intake, with its associated benefits.43 44 53
In the course of this review, we have identified several areas of clinical importance that have not been adequately explored in the literature. While not an exhaustive list, we believe the 10 topics listed in table 2 should be considered as priorities for further research.
Research priorities related to tracheostomy care in intensive care
There are some methodological aspects of our study that merit discussion. Our report benefits from the use of a structured, predefined scoping review methodology, as outlined by The Joanna Briggs Institute.12 As the objective was to map the evidence rather than conduct a critical appraisal, and as is recommended for the scoping review methodology, we made no further attempts to grade the quality of the included reports.12 13 We recognised in advance of our study that there may be a small body of literature and therefore used broad search terms with the resulting need to screen more than 6000 citations. However, we limited our search to the three most widely used citations databases and therefore may have missed articles not included within these. Finally, it should be recognised that we limited our scope of review to the stay in ICU. As such, there may be other management issues that could arise post-ICU discharge that are not included in our investigative themes.
Conclusion
In summary, this scoping review addresses an area of the critical care literature that, while of major clinical importance, has garnered relatively little attention. While major efforts have been expended to investigate the optimal decision-making for, and timing and insertion of, tracheostomies in critically ill patients, the body of knowledge surrounding management of tracheostomies in intensive care is limited by low-quality and non-peer reviewed research. While there has been an increase in research in this area (figure 2), it is evident that there needs to be a shift in our research focus from the conduct of the procedure itself to optimising the management of the tracheostomised patients within our ICUs.
References
Footnotes
Contributors KBL takes responsibility for the content of the manuscript including data and analysis, as the guarantor. KBL and KAW made substantial contribution to the conception and design of the work. All authors were involved in the acquisition, analysis and interpretation of data. All authors were involved in drafting and revising the manuscript and approved the version to be published. All authors agreed to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.