Article Text

Abstract
Rationale Therapeutic thoracentesis is among the most frequently performed medical procedures. Chest discomfort is a common complication and has been associated with increasingly negative pleural pressure as fluid is withdrawn in the setting of non-expendable lung. Visual analogue scales (VASs) are commonly employed to measure changes in discomfort and dyspnoea related to pleural interventions. The minimal clinically important difference (MCID), defined as the smallest change in VAS score associated with patient report of significant change in a symptom, is required to interpret the results of studies using VAS scores and is used in clinical trial power calculations. The MCID for chest discomfort in patients undergoing pleural interventions has not been determined.
Methods Prospectively collected data from two recent randomised trials of therapeutic thoracentesis were used for this investigation. Adult patients with symptomatic pleural effusions referred for therapeutic thoracentesis were enrolled across ten US academic medical centres. Patients were asked to rate their level of chest discomfort on 100 mm VAS before, during and following thoracentesis. Patients then completed a 7-point Likert scale indicating the significance of any change in chest discomfort from preprocedure to postprocedure. The mean difference between discomfort 5 min postprocedure and discomfort just prior to the start of pleural fluid drainage was categorised by Likert scale response.
Results Data from a total of 262 thoracenteses were included in the analysis. Thirty-four of 262 patients experienced a ‘small but significant increase’ or a ‘large or moderate increase’ in discomfort following thoracentesis. The mean increase in VAS score in those reporting a ‘small but significant increase’ in chest discomfort (n=23) was 16 mm (SD 22.44, 95% CI 6.87 to 25.21).
Conclusions The MCID for thoracentesis-related chest discomfort measured by 100 mm VAS is 16 mm. This MCID specific to discomfort resulting from pleural fluid interventions can inform the design and analysis of future pleural intervention studies.
- pleural disease
- thoracentesis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
The minimal clinical important difference (MCID) for chest discomfort has been previously defined in a population of patients with trauma but not in patients undergoing pleural procedures.
What is the bottom line?
We define the MCID for chest discomfort specifically in patients undergoing large-volume pleural fluid aspiration of 16 mm on a standard 100 mm visual analogue scale.
Why read on?
This MCID specific to chest discomfort in pleural interventions establishes a standard for future clinical trial power calculations and enhances the interpretation of the clinical significance of existing pleural disease studies.
Introduction
Pleural effusion is a common diagnosis, making thoracentesis one of the most commonly performed medical procedures.1 2 Large-volume thoracentesis has been associated with several complications, including chest discomfort.3 Improvement in breathlessness is an important clinical goal for this procedure. Randomised controlled trials evaluating pleural fluid aspiration commonly use the visual analogue scale (VAS) to measure patient-centred outcomes such as dyspnoea and discomfort.4–9 A VAS for chest discomfort consists of a 100 mm long line with ‘no discomfort at all’ printed at one end and ‘worst possible discomfort’ at the other; patients are asked to make a mark through the line indicating where their current symptoms fall along that continuum, with the distance in millimetres along the line to the mark representing their numerical VAS score.
Importantly, interpretation of data derived from these scales requires a determination of the minimal clinically important difference (MCID), defined as the smallest change in VAS score perceived as clinically significant. This contrasts with the statistical significance, which may not be relevant to patient care. For example, the smallest possible between-group difference in VAS score of 1 mm could be statistically significant if a trial were very large. Knowledge of how much a score must change before a patient perceives the change as meaningful or worthwhile is necessary to interpret whether a reported difference is clinically significant. As a result, MCIDs are vital to power calculations in trials using patient-centred primary outcomes measured by VAS, as enrollment targets are selected to allow detection of a difference between study groups at the threshold of MCID.
Various methods for determining the MCID have been described.10 The most direct method involves anchoring a change in the tool being investigated to another scale that directly inquires as to whether a change of significance has occurred, such as a Likert scale.
A previously determined MCID for pain of 13 mm on 100 mm VAS derived from emergency department patients with trauma has been used for all recent studies using 100 mm VAS to measure chest discomfort related to pleural fluid aspiration.4–6 8–12 We hypothesised that acute traumatic pain may differ sufficiently from the chest discomfort associated with large-volume thoracentesis to result in a different MCID. The primary aim of this study was to determine the MCID for the VAS for chest discomfort in patients undergoing thoracentesis using a Likert scale anchor.
Methods
Data analysed for this study were obtained during two randomised controlled trials of therapeutic thoracentesis performed at 10 US academic medical centres. One randomised to manometry-guided versus symptom-guided discontinuation of pleural fluid aspiration while the other randomised to drainage by gravity versus manual aspiration; both were negative trials.4 5 Both trials enrolled adult patients with symptomatic pleural effusions of estimated volume 0.5 L or greater referred for therapeutic thoracentesis. Patients without free-flowing effusions, those unable to maintain a seated position for the procedure and those unable to provide informed consent for the procedure were excluded. All participants provided written informed consent. Thoracentesis catheters were inserted in standard fashion following instillation of local anaesthesia with 1% lidocaine without epinephrine. The institutional review boards at each participating medical centre approved these trials.4 5
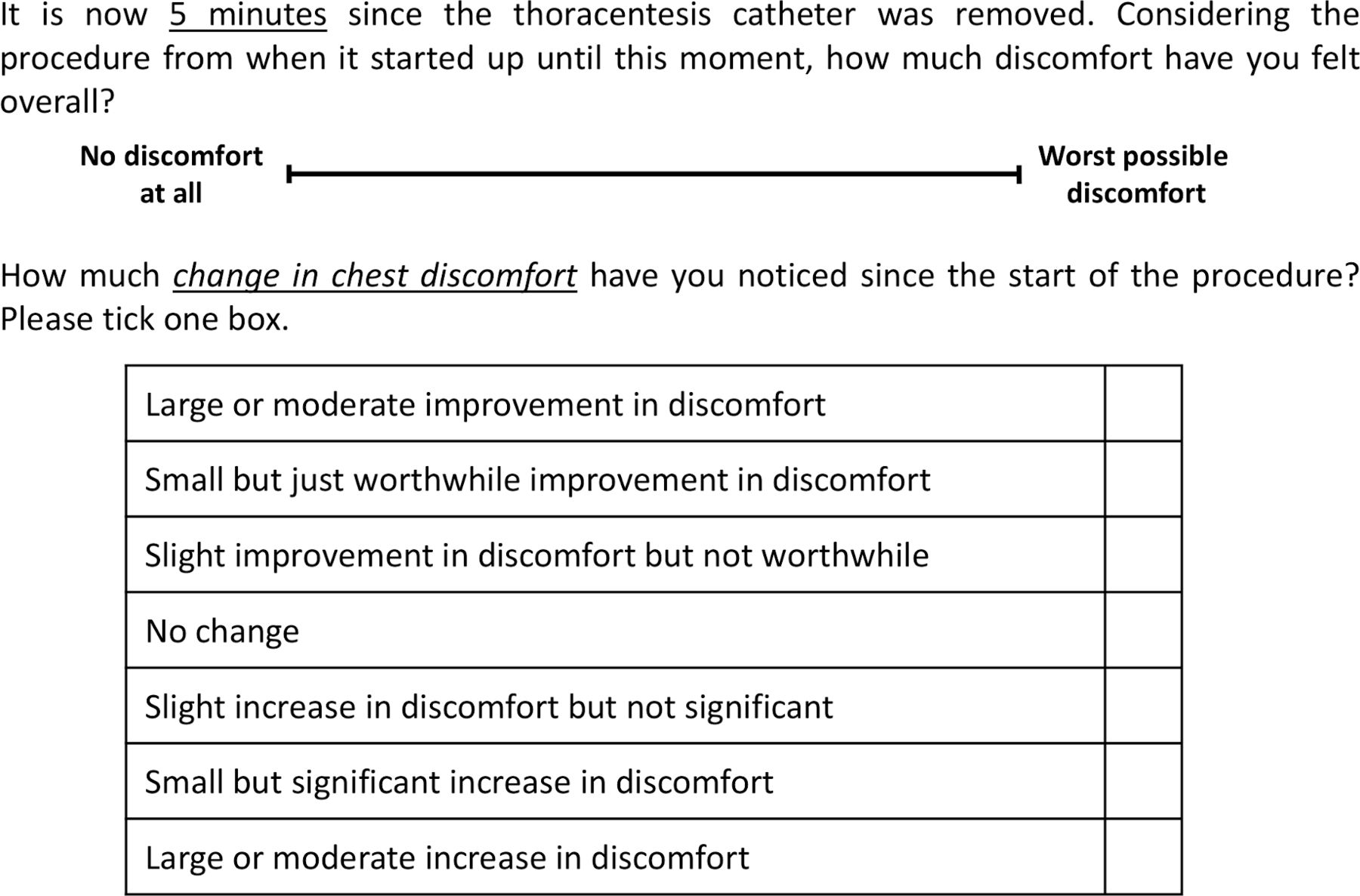
In both trials, patients were asked to indicate their degree of chest discomfort on VAS before, during and after the procedure. Five minutes after drainage catheter was removed, patients were asked to indicate their overall degree of chest discomfort on VAS from procedure start to that moment, followed by a 7-point Likert scale to indicate the degree to which their chest discomfort changed from procedure start to that moment, with the following options: large or moderate improvement, small but just worthwhile improvement, slight improvement in chest discomfort but not worthwhile, no change, slight increase in discomfort but not significant, small but significant increase in chest discomfort and large or moderate increase in discomfort. See figure 1 for the Likert scale and example of VAS scale used in these trials.

Example of visual analogue scale and Likert scale used in these trials.
Mean change in VAS scores between preaspiration and 5 min postprocedure was calculated along with interquartile ranges, stratified by response on the 7-point Likert scale. The threshold for MCID was defined by respondents indicating a ‘small but significant increase in chest discomfort’. Descriptive statistics including means and SDs for continuous variables and percentages and frequencies for categorical variables were also performed. All analyses were done with R V.3.3.1.
Patient and public involvement
The current study used existing data from two randomised trials. Our research question is highly patient centred, by seeking to better characterise the measurement tools used to document discomfort in clinical trials, which will in turn inform future clinical trials of pleural intervention and thus have lasting impact on patient outcomes.
Results
A total of 263 study thoracenteses were performed in the course of the two trials, the first enrolling March 2016 to September 2017 and the second between October 2018 and April 2019. All had complete outcome data, including preprocedure and postprocedure VAS scores and Likert scale responses. Mean age was 65 years (56–72 years), 52% were women and two-thirds had comorbid malignancy. See table 1 for additional demographic information. The most common final effusion diagnosis was malignancy, accounting for 115 effusions (60%), with additional aetiologies listed in table 2. Mean volume drained was 1150 mL. Most procedures were stopped due to discomfort (112 patients, 43%) or spontaneous cessation of flow after complete effusion evacuation (116 patients, 44%), with remaining discontinuation reasons listed in table 3.
Subject demographics
Effusion etiologies
Reasons for discontinuation of pleural fluid drainage
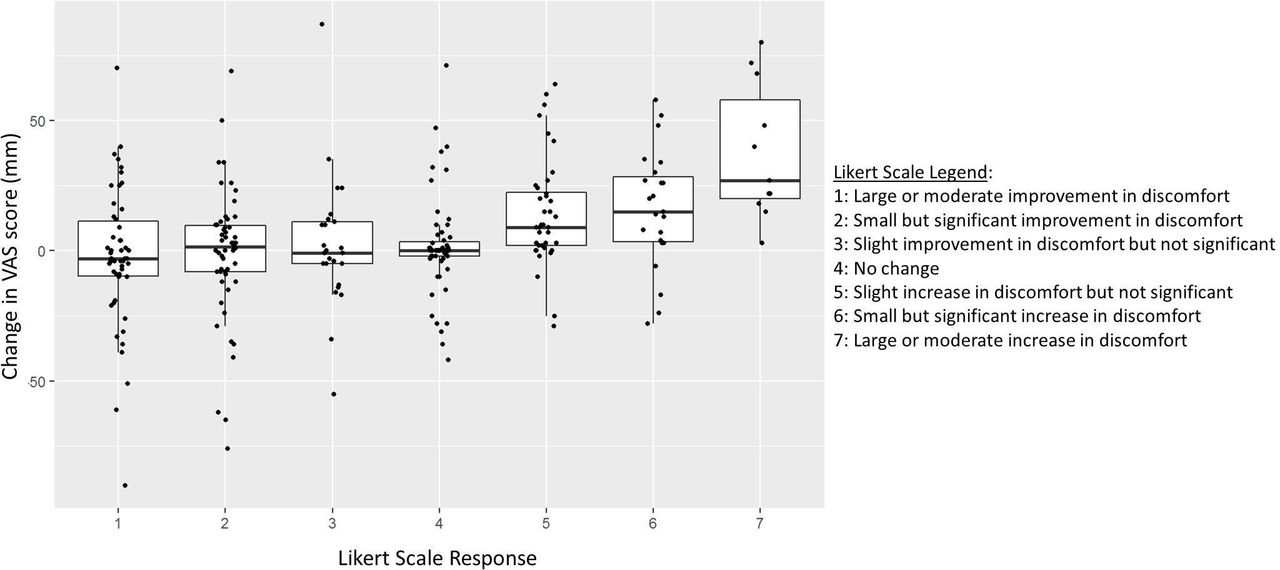
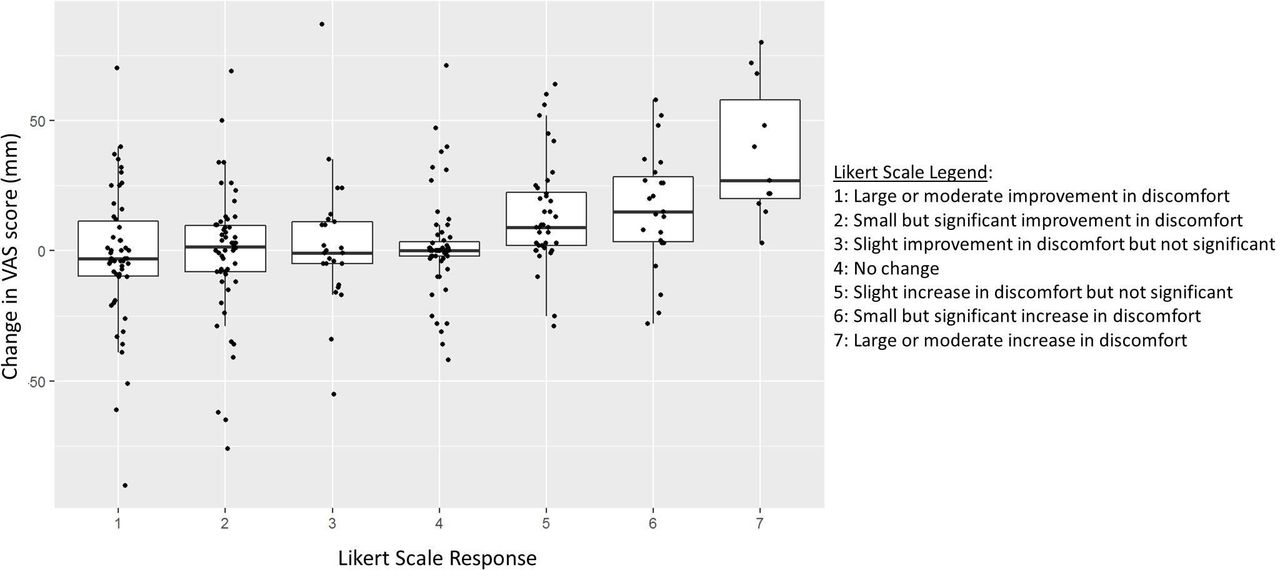
Thirty-four of 263 patients experienced a ‘small but significant increase’ or a ‘large or moderate increase’ in discomfort following thoracentesis. The mean increase in VAS score in those reporting a ‘small but significant increase’ in chest discomfort (n=23) was 16 mm (SD 22.4, 95% CI 6.9 to 25.2). Table 4 and figure 2 illustrate the trend in change in VAS score by Likert scale responses. Ninety-eight of 263 patients (37%) were using narcotic analgesics at the time of the procedure. Those taking narcotics did not differ in reported a mean overall chest discomfort score (mean difference 4.3 points higher in those on narcotics, 95% CI −1.4 to 10.0, p=0.14).
{kind=link}
{kind=link}
Preprocedure to postprocedure change in visual analogue scale discomfort score according to Likert scale response.
Likert Scale responses
Discussion
Using data from two recent multicentre randomised trials in which all patients completed VAS for discomfort preprocedure and postprocedure as well as postprocedure Likert scales, we established a VAS MCID of 16 mm for chest discomfort related to pleural fluid aspiration using the anchor method.
The VAS is widely used in pleural intervention trials as a standardised tool to translate subjective symptoms such as dyspnoea or discomfort into a numerical construct. It therefore plays a prominent role in power calculations for clinical trials related to pleural interventions. Despite its widespread use, the MCID for discomfort specific to pleural interventions has not been previously defined.
The discomfort of excessively negative pleural pressure is unlikely to be experienced in the same manner as other forms of pain or discomfort. A wide range of VAS MCIDs for pain and discomfort of different aetiologies have been described, including 10 mm in acute postoperative pain13 and pain due to endometriosis,14 13 mm for patients with acute traumatic pain in emergency department,10 11 18 mm for total hip arthroplasty15 and 22 mm for total knee arthroplasty.15 The pleural discomfort MCID of 16 mm falls within this previously described 10–22 mm range for varying kinds of discomfort. From a trial design perspective, however, the number of trial subjects required to have sufficient power to detect a difference of 10 mm between groups tends to be markedly different than that required to detect a difference of 22 mm between groups. Using the power calculation assumptions used in GRAVITAS, for example, power to detect a 10 mm difference would require 282 total subjects versus just 58 to detect a 22 mm difference.5 Knowledge of the specific VAS MCID for pleural procedures is therefore crucial for well-designed future studies intended to demonstrate significant improvement in this important patient-centred outcome. There has been a dramatic rise in clinical trials in pleural disease in the last decade, the majority of which use patient-centred primary outcomes, such as pain or dyspnoea. Our study now provides a definitive way to interpret and contextualise these subjective outcomes in future trials.
This study has several limitations. Although we had a relatively large total sample size of 263 thoracenteses, only 23 patients reported a ‘’mall but significant increase in discomfort’ on Likert scale from which the MCID can be calculated, leading to a relatively wide 95% CI and therefore somewhat less certainty in the precision of the MCID value we report. However, in a similar study which determined the VAS MCID for improvement in dyspnoea related to pleural intervention, only 20 patients registered the Likert category of interest also resulting in relatively wide confidence intervals7 but has nonetheless been used widely in the development of subsequent trials. Other prior VAS MCID study populations have demonstrated similar findings.10 Another potential limitation of this work is that it only included thoracenteses but not other pleural interventions such as tube thoracostomy. However, these procedures tend to be similar in technique and catheter size, suggesting these findings may generalise to all small-bore pleural catheter procedures. While more invasive pleural procedures, including medical thoracoscopy and large-bore chest tube placement, may result in different discomfort patterns than that described by the MCID reported here, our study provides more relevant information than previously published non-thoracic studies. Finally, the clinical trial population used for this study may not be fully generalisable to non-study-based patient populations.
In conclusion, this study determined the MCID on VAS specific to chest discomfort during pleural drainage procedures is 16 mm. Chest discomfort is an important patient-centred clinical outcome of pleural procedures; this specific MCID can be used to plan and interpret results of future pleural intervention trials.
References
Footnotes
Contributors FM, RL and OR were involved in the development of the study design. FM, RL, OR, JK, LR and CW were involved in the collection of the data and performance of procedures involved in the study. HC was contributed to statistical analysis of the data. GJD wrote the manuscript with important input from RL and FM. All authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data is available upon reasonable request from Robert Lentz, MD at robert.j.lentz@vumc.org.