Article Text

Abstract
Objective To explore the existence and trends of social inequalities related to pneumonia mortality in Colombian adults using educational level as a proxy of socioeconomic status.
Methods We obtained individual and anonymised registries from death certificates due to pneumonia for 1998–2015. Educational level data were gathered from microdata of the Colombian Demography Health Surveys. Rate ratios (RR) were estimated by using Poisson regression models, comparing mortality of educational groups with mortality in the highest education group. Relative index of inequality (RII) was measured to assess changes in disparities, regressing mortality on the midpoint of the cumulative distribution of education, thereby considering the size of each educational group.
Results For adults 25+ years, the risk of dying was significantly higher among lower educated. The RRs depict increased risks of dying comparing lower and highest education level, and this tendency was stronger in woman than in men (RR for primary education=2.34 (95% CI 2.32 to 2.36), RR for secondary education=1.77 (95% CI 1.75 to 1.78) versus RR for primary education=1.83 (95% CI 1.81 to 1.85), RR for secondary education=1.51 (95% CI 1.50 to 1.53)). According to age groups, young adults (25–44 years) showed the largest inequality in terms of educational level; RRs for pneumonia mortality regarding the tertiary educated groups show increased mortality in the lower and secondary educated, and these differences decreased with ages. RII in pneumonia mortality among adult men was 2.01 (95% CI 2.00 to 2.03) and in women 2.46 (95% CI 2.43 to 2.48). The RII was greatest at young ages, for both sexes. Time trends showed steadily significant increases for RII in both men and women (estimated annual percentage change (EAPC)men=3.8; EAPCwomen=2.6).
Conclusion A significant increase on the educational inequalities in mortality due to pneumonia during all period was found among men and women. Efforts to reduce pneumonia mortality in adults improving population health by raising education levels should be strengthened with policies that assure widespread access to economic and social opportunities.
- pneumonia
- respiratory infection
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
How unequal is the mortality in adults from pneumonia in Colombia?
What is the bottom line?
A significant increase on the educational inequalities in mortality due to pneumonia during all period was found among men and women.
Why read on?
To study social inequalities related to pneumonia mortality trends in Colombian adults using educational level as a proxy of socioeconomic status.
Introduction
Lower respiratory tract infections, including pneumonia, are the fourth leading cause of death globally, remaining as the most deadly communicable disease, triggering 3.0 million deaths worldwide in 2016.1–3 Pneumonia is a leading cause of morbidity and mortality, especially in elder patients and patients with comorbidities.4 5 The annual incidence of pneumonia was estimated at 1.07–1.2 cases per 1000 persons per year in Europe and 16.9 cases per 1000 persons per year in Asia.5 In Latin American adults, the annual incidence rates in Argentina, Chile and Brazil in 2010 were 120 000, 170 000 and 920 000 cases, respectively.6 In Colombia, the annual incidence of all-agents pneumonias has been estimated in 1023.1 per 100 000 (95% CI 797.6 to 1435.0).7 8
Preventive measures had shown to be useful to prevent pneumonia among adults, as the immunisation against pneumococcus, Haemophilus influenzae type b and influenza.9 In particular, pneumococcal polysaccharide vaccines have shown high effectiveness for reducing mortality due to pneumonia among adults in high-income countries.10–13 In addition, antibiotic treatments are available for bacterial pneumonia in children and adults.14 15 The incidence, but overall, the lethality of the illness is highly conditioned to timely access to these measures.
Pneumonia is an interesting health outcome in terms of health equity, while most of deaths by this cause take place in low-income and middle-income countries (LMIC).16–18 Particularly in adults, pneumonia also represents a significant disease and economic burden owing to increases in healthcare use among elderly.19 20 Despite this, studies about the toll of socioeconomic conditions and pneumonia in LMIC are scarce.
Differences in health status and outcomes among populations could be explained by the contribution of social determinants of health, including socioeconomic status (SES) and education.20 SES has been traditionally recognised as a principal cause of health disparities and as a tracer of morbidity and mortality patterns, inclusive in infectious diseases as pneumonia among children and adults.20 21 Several researches has documented this graded relationship.22–27
Educational level is a good proxy for SES and has certain advantages over income as a marker of SES, since it is established early in life and is not subject to the same fluctuations over the lifespan, mostly in old age.27–29 Some works have described the inverse association between adult mortality risk and education level.30–32 The educational gradient in mortality is a long-established concern of researchers, stakeholders and public health establishments.33
Colombia is one of the countries with the highest income inequality around the world, and the second in Latin American and Caribbean (Gini index 2016: Guatemala 0.53, Colombia 0.52).34 Large inequalities in Colombia have been observed in the prevalence of infectious diseases, particularly among children.35–39 Nevertheless, to the best of our knowledge, studies on how infectious diseases as pneumonia are socially distributed in adult population and how this distribution evolves along time are scarce in LMIC, particularly in Colombia. Therefore, we aimed to explore the existence and trends of social inequalities related to pneumonia mortality in Colombian adults using education as a proxy of SES.
Methods
Methods used in this paper were almost identical to previous studies40 41 in order to ensure suitable comparability for potential further analyses of inequalities among different causes of death.
Data
Deaths
We obtained individual and anonymised registries from death certificates due to pneumonia for the period 1998–2015. In Colombia, vital statistics are collected by the Colombian National Agency of Statistics (DANE, for its acronym in Spanish). For this analysis, we used deaths from International Classification of Diseases-10 codes J12-J16; J18. We aggregated cases by sex, year and educational level, with age at death at least 25 years.
Colombian death certificates include information on educational level of the deceased since 1998. Similar to the previous studies, we categorised educational level as follows: primary education (those who accessed to elementary educational attainment or less); secondary education (high school) and tertiary education (post-secondary level: technical, technological and university education).
Data on five demographic variables (year, sex, 5 years age group, department and urban/rural residence) were available for almost 100% of all deaths, while data on educational level were missing for 24.079 of 86.677 deaths (27.8%). The proportion of deaths with missing information on education were reasonably stable along the period. We used multiple imputation methods42 implemented in SAS through the IMPUTE procedure to impute educational level for these cases.43 In short, this procedure fits a sequence of regression models and draws values from the corresponding predictive distributions. The sequential regression procedure was applied based on a model that imputed educational level, healthcare insurance scheme and marital status based on the demographic variables mentioned above as covariates, excluding few cases which had at least one missing value. We obtained five databases, each one including five iterations. Results were virtually equal for the five resulting databases. Details of this method are explained elsewhere.42
Population (denominators)
Estimates of population size are available through DANE—based on demographic projections derived from the 2005 census. However, these estimates do not contain information on numbers by educational level. Therefore, we directly obtained mid-year population counts by age, sex and educational level from microdata of the Colombian Demography Health Surveys44 that are collected for each 5-year period (1995, 2000, 2005, 2010 and 2015). We chose age 25 as lower limit for educational level, considering that almost all individuals will have accessed their highest educational level at this age. In order to calculate the population size in each educational group, we obtained population counts for the educational levels by year, sex, and 5-year age groups and sex according the factors of expansion provided in the metadata of each survey. Subsequently, we calculated proportions for the educational levels year, sex and 5-year age groups and multiplied these with the total population provided by DANE by year, sex and 5-year age groups.45 Finally, we made demographic projections to obtain population counts for the years in between each lustrum of the surveys using the demographic Population Analysis Spreadsheets (PAS) provided by US Census Bureau which interpolates and soft the trends.46
Analysis
We carried out all the analyses with the five multiple databases generated by the multiple imputation procedure. We used standard techniques as implemented in the PROC MIANALYZE procedure in SAS to combine estimates from all databases and adjust SEs to account for uncertainty in the imputation.47 All analyses were conducted in SAS V.9.2.
In order to adjust both rates and SEs for age at death, we first used the world population according to WHO 1997 as standard population,21 resulting in Age Standardised Mortality Rates (ASMR) expressed per 100 000 person-years.
Annual trends in ASMR by sex and educational level were quantified by calculating the estimated annual percentage change (EAPC), which measures the average rate of change in the mortality rate per year (negative EAPC: decreasing trend, positive EAPC: increasing trend). To test whether an apparent change in mortality trends was statistically significant, we used joinpoint regression, which fits a series of joined straight lines to age-adjusted rates using a Monte Carlo Permutation method to identify the best-fitting point (called joinpoint, the year in which a significant change in the mortality trend occurred), where the rate of increase or decrease changes significantly.48 Joinpoint regression has been proved to adequately assess ecological risk by identifying changes in the population structure based on time series, as well as identify when this change occurs, allowing an accurate and complete understanding of population dynamics.49 EAPC and joinpoints were determined based on the log-transformed ASMRs and their SEs.50
We also implemented Poisson regression models with number of deaths as dependent variable and the natural log of person-years as offset variable, incorporating age and educational level as independent variables. We estimated rate ratios (RR by educational level) by using these Poisson regression models, comparing mortality of all educational groups with mortality in the highest education group. In order to obtain relative measures of inequality (RR and relative index of inequality (RII)), log-linear models have been used that assume a Poisson distribution of mortality, that is, generalised linear models with Poisson distribution. Changes in the RR over time result from changes in both risks and the distribution of educational level.51 To assess changes in disparities ‘controlling’ for changes in the educational distribution, we estimated the RII, regressing mortality on the midpoint of the cumulative distribution of education, thereby taking into account the size of each educational group.52 53 Values >1.00 indicate educational inequalities favouring the higher educated. We also calculated how RII evolved during the studied through joinpoint regressions. Deviance and Wald tests in our models show that the models fit reasonably well and that the explanatory variables employed in the model are significant towards the explained variable.
Patient and public involvement
Patients were not involved in any way in this manuscript.
Results
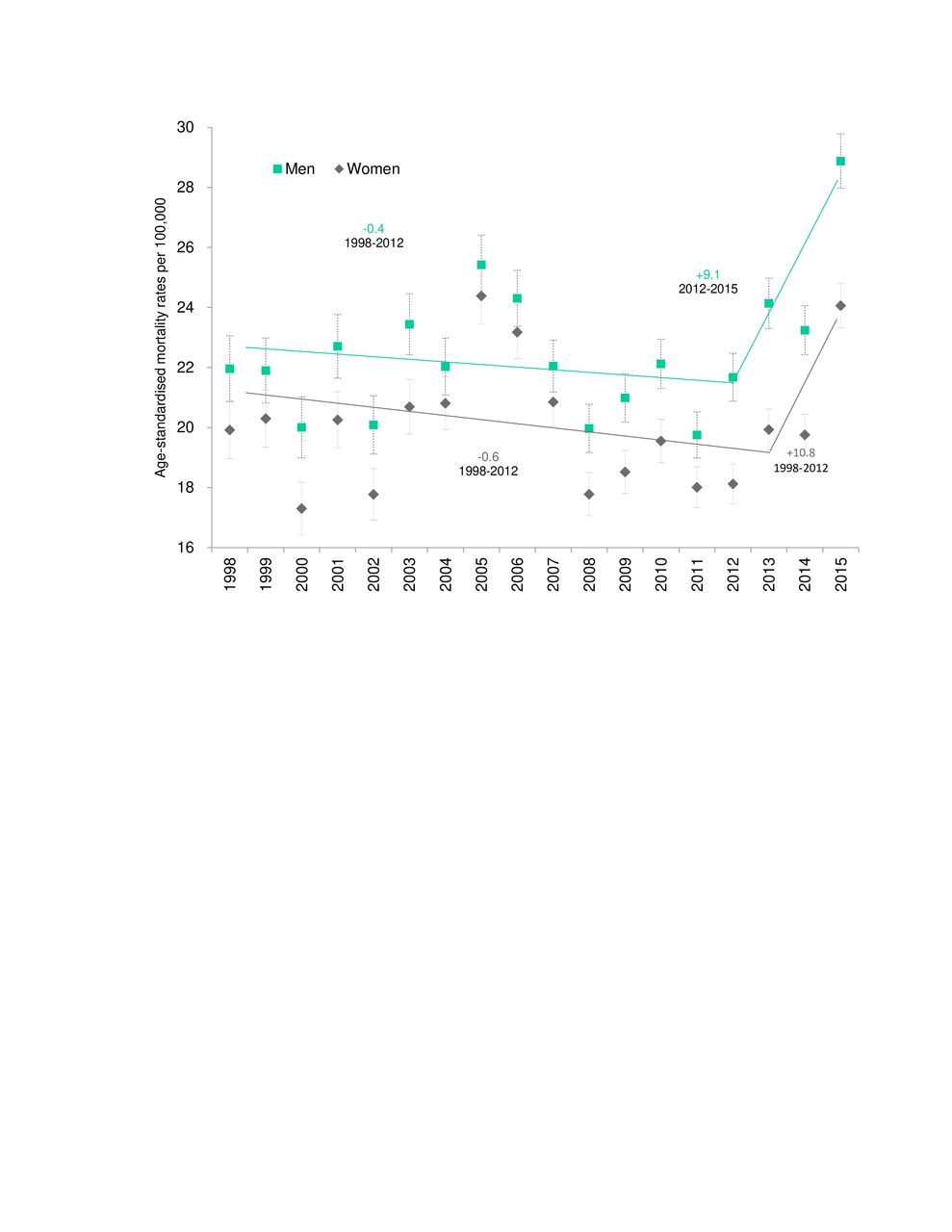
Table 1 shows overall descriptive and analytical information about adult mortality for pneumonia along the period 1998–2015 in Colombia. Out of the total pneumonia deaths, 78.2% occurs at senior ages (65 years and more). ASMR are almost 10 and 16 times higher among senior than middle aged adults among men and women, respectively, and even much more if compared with young adults. All estimated mortality rates were higher in men than in women. Figure 1 shows how mortality in pneumonia among adults remained stable from 1998 but with a non-significant but strong increase from 2012/2013 (men/women). By age groups, we do not find statistically significant changes in mortality trends by pneumonia, except a significant and strong increase at the very end of the period among senior men (EAPC=11.2%, 95% CI 9.9% to 12.5%) and women (EAPC=11.7%, 95% CI 10.4% to 13.0%) (figure 2).

Age standardised mortality rates by pneumonia (deaths by 100 000 population) among adult (25+ years) men and women, 1998-2015.

Age-standardised mortality rates (ASMR) by pneumonia separately by age groups and sex, Colombia, 1998–2015.
Counts (deaths, population), age standardised mortality rates (ASMR), rate ratios (RR) and relative index of inequality (RII) of pneumonia mortality among Colombian adults, estimated separately by age groups and educational level (1998–2015)
Mortality rates by pneumonia among adults aged 25+ years were consistently higher among less educated for all sex and age groups. In addition, RR comparing mortality at lower educational levels with those with tertiary educational attainment were found to be larger among younger groups and by comparing woman with men (RR for primary education=2.34 (95% CI 2.32 to 2.36), RR for secondary education=1.77 (95% CI 1.75 to 1.78) versus RR for primary education=1.83 (95% CI 1.81 to 1.85), RR for secondary education=1.51 (95% CI 1.50 to 1.53)) (table 1). Moreover, we found among men and women with primary education a steady growing trend (significant among men), while both men and women with tertiary education showed a significant reduction (3.4% and 5.8%, respectively) with an inflexion point in 2013 when mortality rates show a non-significant increase up to the end of the period (figure 3).

Age-standardised mortality rates (ASMR) by pneumonia separately by educational level and sex, Colombia, 1998–2015.
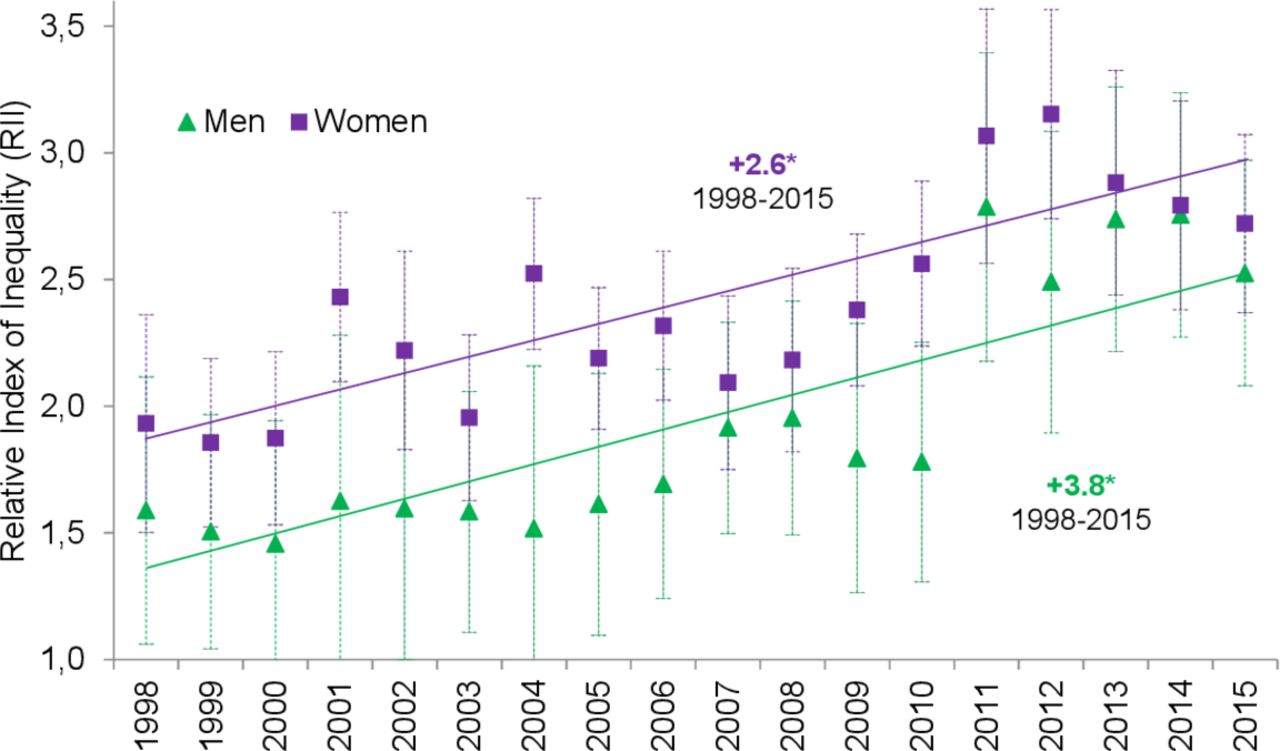
The RII in pneumonia mortality among adult men was 2.01 (95% CI 2.00 to 2.03) and in women 2.46 (95% CI 2.43 to 2.48). Also, RII was greatest at young ages, for both sexes (table 1). Time trends showed steadily significant increases for RII in both men and women (EAPCmen=3.8, 95% CI 3.6 to 4.0; EAPCwomen=2.6, 95% CI 2.4 to 2.8) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relative index of inequalities (RII) trends for pneumonia mortality for aged 25+ years, including annual percentage change (APC) based on joinpoint models, Colombia, 1998–2015.
Discussion
Educational inequality in pneumonia mortality in Colombia is on the rise. Age-standardised mortality rates by pneumonia in Colombia (1998–2015) were found to be larger among men than in women; much larger in senior compared with younger ages; and consistently higher among those less educated. We found relatively stable trends of mortality by pneumonia in both sexes with a strong rise during the last years due to an alarming increase in mortality among senior men and women from 2012/2013, respectively. By educational level, the final peak from 2013 was found only among those with tertiary education, but not significant. We found significant increases in pneumonia mortality rates among those with primary education, along the whole period. However, those with tertiary education strong and steadily decreased mortality up to 2013. Consequently, a significant steady increase in the RII during all period was found among men and women.
Pneumonia mortality rates in Colombia evidenced a clear age-dependency, with lowest rates for young adults and much higher rates for senior adults. In less than two decades, mortality due to pneumonia among 25+ years showed a worrying increase for women and men. Our results are consistent with the Global Burden of Disease study, where deaths occurred in adults with 50–69 years and in older than 70 due to lower respiratory infections increased 26.5% (95% CI 23.2 to 29.7) and 33.6% (95% CI 31.2 to 36.1) from 2007 to 2017, respectively. Additionally, among adults older than 70 years, deaths increased from pneumococcal pneumonia (60.4% (95% CI 39.7 to 79.9)), influenza (91.1% (95% CI 82.3 to 99.6)) and respiratory syncytial virus pneumonia (100.3% (95% CI 92.4 to 108.6)) between 1990 and 2017.54 A positive evolution that took place in this timeframe is the decrement of mortality rates among young adults, however this was not a substantial one.
In our analysis, differences between the lowest and highest educated are reflected in the RRs estimates finding much higher risk of dying from pneumonia in adults with low education level. Our results are consistent with the findings reported by Huisman et al in a mortality inequalities analysis conducted in eight western European populations. They calculated a RR of 1.45 (95% CI 1.37 to 1.54) between the pneumonia mortality rate in low-educational groups ≥45 years as a proportion of mortality rate in high educational groups.55 Therefore, they found that RRs among pneumonia mortality rates were diminishing as age increases, as we found in our analyses.55
ASMR were higher in lower educated, showing how low education could be a good proxy for conditions of vulnerability,56 in which the risk of death from pneumonia is increased. This evidence is very important for policymakers in avoidable mortality. Our results could be linked with previous analyses that show how low educational level is associated with mortality, likely contributing to lower access to healthcare as well as diminished awareness and adoption of policy measures planned by public health stakeholders, which increases risk of poor clinical outcomes and mortality.57–59
Other authors have used similar tools to study educational differences in mortality due to chronic diseases, for example, Manor et al, in Israel, studied educational differentials in mortality from cardiovascular disease among men and women.59 In other study, Mackenbach et al studied inequalities in lung cancer mortality by the educational level in 10 European populations during the 1990s.58 Similarly, Stirbu et al compared the magnitude and the contribution of educational inequalities in mortality avoidable by medical care in 16 European countries.60 And, in Colombia de Vires et al, have studied inequalities in cervical cancer mortality by educational level in Colombia.40 41
Given that the impact of inequalities in educational level on mortality is evident, the explanations of this probable association could be related to how healthcare providers, both preventive and curative, deliver information to patients without considering the diverse cultural contexts as educational differentials. According to pneumonia deaths, having high levels of education would allow us a better understanding about preventive measures such as vaccination. In 1997, the Advisory Committee on Immunisation Practices updated the recommendations to vaccinate the entire population over ≥65 years.61 In Colombia, immunisation in those aged ≥60 years against pneumococcus is included at the expanded immunisation programme. Similarly, we can have more knowledge about signs and symptoms of alarm, and therefore, seek timely attention. And, after receiving care, you can be more adherent to the treatments and recommendations of health professionals.
Immunisation in older adults has been promoted during the last decade in Colombia. However, the reported vaccination rates remain low. For example, Cano et al in 2012 conducted a cross-sectional survey in a sample of 2000 population in a survey in Bogota. The results reported coverage for vaccination among individuals of 60 years and older is 73.0% for influenza, 57.8% for pneumococcus and 47.6% for tetanus.62 However, these coverages are surely lesser in other Colombian territories. There is enough evidence regarding the association between educational status and vaccination. A Colombian study found that a mother completing high school or above was associated with a 16% higher odds of being immunised.63 Then, vaccination campaigns in older adults should be strengthened to increase vaccination coverage, especially in groups more vulnerable, in order to reduce mortality rates due to pneumonia.
Despite several strengths, our work has some limitations that should be considered. First, data on mortality were obtained from mortality registries of DANE vital statistics, while data on the population distribution by education were obtained from censuses and demographic projections. The latest may have led to the so-called numerator/denominator bias, which usually results in an overestimation of disparities.43 Furthermore, for some years, data on population size were obtained from demographic projections combined with distributions of education from surveys. To assess the impact of this potential bias, we experimented with different education distributions from multiple data sources, showing that the overall trends in our study were robust to different assumptions on the distribution of education.40 64 Additionally, despite the joinpoint regression did not identify this oscillation, a peak for pneumonia is visible in 2005–2006 for senior men and women. To the best of our knowledge, no previous evidence exists explaining that peak, and further retrospective research must be necessary to be addressed that change in morbidity and/or lethality of pneumonia during that period. A better knowledge of this fluctuation will potentially contribute to understand strong oscillations of infectious diseases and the vulnerability of the senior population to better address epidemics of endemic severe respiratory infections.
The rise in education levels during the last decades has contributed to improve population well-being, longevity and health.65 However, these improvements have been achieved unequally, especially in LMIC. In conclusion, a significant increase on the educational inequalities in mortality due to pneumonia during all period was found among men and women. This shows deficiencies in educational policy in terms of equity. Efforts to reduce pneumonia mortality in adults improving population health by raising education levels should be strengthened with policies that assure widespread access to economic and social opportunities. Reducing exposure to pneumonia risk factors in low-educational populations should be developed and implemented through efficient interventions like vaccination in elders. Further research is needed to enhance the understanding of inequalities in infectious disease mortality, including older populations and other pathologies.
References
Footnotes
Contributors All authors (NJA-Z, IA, CC-O, FDLH-R, NA-G) contributed to planning, conduct, reporting, conception and design, analysis and interpretation of data for this manuscript.
Funding Regular budget of the Observatorio Nacional de Salud, Instituto Nacional de Salud of Colombia.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article. All data used in this paper are public. Data used are available on reasonable request.