Article Text

Abstract
Introduction Cardiopulmonary exercise testing (CPET) provides a series of biomarkers, such as peak oxygen uptake, which could assess the development of disease status in interstitial lung disease (ILD). However, despite use in research and clinical settings, the feasibility of CPET in this patient group has yet to be established.
Methods Twenty-six patients with ILD (19 male) were recruited to this study. Following screening for contraindications to maximal exercise, participants underwent an incremental CPET to volitional exhaustion. Feasibility of CPET was assessed by the implementation, practicality, acceptability and demand, thus providing clinical-driven and patient-driven information on this testing procedure.
Results Of the 26 recruited participants, 24 successfully completed at least one CPET, with 67/78 prospective tests being completed. Contraindications included hypertension, low resting oxygen saturation and recent pulmonary embolism. Of the CPETs undertaken, 63% successfully reached volitional exhaustion, with 31% being terminated early by clinicians due to excessive desaturation. Quantitative and qualitative feedback from participants revealed a positive experience of CPET and desire for it to be included as a future monitoring tool.
Conclusion CPET is feasible in patients with ILD. Identification of common clinical contraindications, and understanding of patient perspectives will allow for effective design of future studies utilising CPET as a monitoring procedure.
- exercise
- interstitial fibrosis
Data availability statement
Data are available on reasonable request. Please contact the corresponding author (CS).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Is cardiopulmonary exercise testing safe, practical and acceptable to patients with interstitial lung disease?
This modality of exercise testing provides novel physiological data in addition to traditional spirometry and should be considered as a future biomarker for use in this clinical population.
This study provides important clinical data on safety, and the valuable patient perspective on the acceptability, of exercise within the management of interstitial lung disease.
Introduction
Interstitial lung disease (ILD) is the collective term for a series of pulmonary disorders characterised by inflammation, interstitial and alveolar damage, and often irreversible declines in lung function, with idiopathic pulmonary fibrosis (IPF) being the most common subtype of ILD, affecting ~32 500 people and accounting for 1% of all deaths in the UK.1
Traditionally, measures of pulmonary function, including forced vital capacity (FVC) and the diffusing capacity for carbon monoxide (DLCO), have been used to monitor disease progression and evaluate the efficacy of treatments. Both variables are predictive of mortality2 and provide greater predictive power for survival over 6 months than histopathological factors alone.3 However, peak oxygen uptake (VO2peak), the primary outcome from cardiopulmonary exercise testing (CPET), is also associated with mortality4 and is therefore an important variable to consider alongside traditional resting spirometry.
For CPET to be integrated into clinical practice, it must be shown to be a feasible procedure and well tolerated by patients undergoing the test—an important consideration given its exhaustive nature. Therefore, this study (Exploring the potential of Cardio Pulmonary Exercise Testing as a biomarker in patients diagnosed with Fibrosing Lung Disease) sought to assess the feasibility of CPET, notably the implementation, practicality, acceptability and demand, in a cohort of patients with ILD.
Methods
Design and population
This feasibility study examined practicalities and safety associated with performing CPET in individuals with ILD. The study was designed to have participants perform three CPETs in a 6-month period, with 3 months separating each test.
The inclusion criteria for this study were as follows: (1) clinical diagnosis of fibrotic lung disease as determined by the Royal Devon and Exeter ILD Team; (2) 40–85 years. of age; (3) FVC >40%; (4) DLCO >25%; (5) willing and able to provide informed consent. Exclusion criteria included: (1) unable/unwilling to provide informed consent; (2) left or right ventricular ejection fraction <50%; more than mild valvular heart disease; lack of available chest CT images; (3) significant repolarisation abnormalities or arrhythmias identified by resting 12-lead ECG or untoward ECG changes and/or symptoms of ischemia during previous baseline testing of CPET; (4) significant neurological impairment (anything that prevents patients from cycling); (5) poorly controlled (symptomatic) asthma, or recent exacerbation of asthma (requiring hospitalisation or medical therapy) within the preceding 4 weeks; (6) severe cardiovascular comorbidity or other medical conditions that could contribute to dyspnoea, (7) forced expiratory volume in 1 s/FVC (FEV1/FVC) ratio <65%; (8) daytime oxygen therapy; (9) contraindications to exercise testing.
Consequently, 26 patients with ILD (19 male) were recruited. Of these 26, n=13 were currently taking antifibrotic medication (nintedanib, n=10; pirfenidone, n=3). Further patient characteristics and diagnoses are listed in table 1.
Baseline anthropometric, pulmonary and clinical data, alongside differences between sexes and antifibrotic medication status, in 26 people with interstitial lung disease
All participants provided written and informed consent on recruitment to the study.
Physiological measures
Stature and body mass were assessed using standard methods, with body mass index (BMI) subsequently calculated. Body fat percentage was assessed using air displacement plethysmography (BodPod; COSMED, Rome, Italy), with subsequent values for fat mass and fat-free mass (FFM) calculated.
Measures of FEV1, FVC and DLCO were retrospectively extracted from pulmonary function test (PFT) data from each participant’s medical records at the date closest to their CPET. Data are presented as absolute values and as a per cent of a predicted value for age, sex, and stature. In addition, composite ‘Gender-Age-Physiology’ scores,5 were also calculated for each participant.
Cardiopulmonary exercise testing
Participants performed a CPET on an electronically braked cycle ergometer (Lode Excalibur; Lode, Groningen, the Netherlands), undertaking an incremental protocol as per existing international guidelines.6 Participants performed 3 min unloaded cycling (0 W) as a warm-up, before an incremental ramp phase whereby resistance increased by 10 W/min. Participants maintained a cadence between 60 and 80 revolutions per minute (rpm) until volitional exhaustion, defined as a decrease in cadence >10 rpm for five consecutive seconds despite verbal encouragement from research staff. On exhaustion, participants returned to unloaded cycling at 0 W for a further 3 min to cool down. On cessation of unloaded cycling, participants recovered in a seated position off of the cycle ergometer for approximately 10 min. Once recovered, and with permission from the attending doctor, participants were free to leave.
Throughout CPET, pulmonary gas exchange was recorded using a metabolic cart (Medgraphics Ultima; Medical Graphics UK Ltd., Gloucester, UK). Data were measured breath-by-breath and analysed in 10 s averages. Normative values7 were utilised to present VO2peak and peak work rate (WRpeak) as a percentage of predicted.
Participant safety
Prior to CPET, all participants were clinically screened for contraindications to maximal exercise (eg, hypertension). Furthermore, all participants wore a 12-lead ECG (Welch Allyn CardioPerfect; Hillrom, Chicago, USA) and pulse oximeter (Choice MMed MD300C2; ChoiceMMed, Dusseldorf, Germany), to monitor cardiac changes and peripheral capillary oxygen saturation (SpO2), respectively. All CPETs were supervised by an exercise physiologist and medical doctor, and the CPET was terminated if either ECG (eg, arrhythmia) or SpO2 responses warranted early cessation for patient safety. In the first round of CPETs, the SpO2 limit was conservatively set at <88%, and extended to <80% in the second and third CPETs. This latter cut-off aligns with international guidelines,6 as hypoxaemia was also shown to be well tolerated in the first CPET; any adverse symptoms (should they have occurred) also provided clinicians with reasons for CPET termination in addition to desaturation.
Feasibility
Feasibility was assessed using existing guidelines,8 predominantly by focusing on ‘implementation’ (degree, and success/failure, of execution of CPET), ‘practicality’ (ability of participants to perform CPET, with focus on safety), ‘acceptability’ (perceived appropriateness of CPET), and ‘demand’ (expressed interest in use of CPET).
Each of these components were measures in differing ways:
Implementation of CPET was assessed by (A) identifying reasons, and their number, as to why participants did not undertake CPET, and (B) identifying reasons, and their number, for clinician-led termination of CPET.
Practicality was assessed by characterising the number of excessive ECG and SpO2 changes during CPET.
Acceptability and demand were established by identifying participant opinions on satisfaction with, and suitability of, CPET for future use. This was undertaken as part of an evaluation of the wider study (full questionnaire provided in online supplemental file 1 and was completed using two processes.
First, support for three brief statements, were evaluated on a 7-point Likert scale with a balanced number of positive and negative response options, whereby 1=‘strongly disagree’ and 7=‘strongly agree’. These included: (1) ‘The exercise test was too physically challenging for someone with my lung condition’, (2) ‘Based on my experience in this trial, I think CPET is feasible for lung disease patients’ and (3) ‘The idea of using exercise testing to develop individualised exercise programmes for patients does not appeal to me’. Participants were encouraged to provide additional reflections on these questions.
Second, qualitative responses from a semi-structured interview were examined, with particular focus on the question ‘How did you find the exercise test, and if you have done other exercise tests (like the shuttle walk test), which do you prefer and why?’
Supplemental material
Statistical analyses
Baseline anthropometric, pulmonary and clinical data were compared between (1) males and females, and (2) participants on antifibrotic medication and those that were not. This was undertaken using independent samples t-tests to infer any homogeneity (or heterogeneity) in the sample. Effect sizes, using existing thresholds9 were also utilised to infer trivial (<0.2), small (0.2<0.5), medium (0.5<0.8) and large (≥0.8) differences between groups. Paired samples t-tests identified changes in SpO2 in each CPET.
Pearson’s correlations were utilised to establish relationships between parameters of fitness, and nadir and change in SpO2; as well as between SpO2 values at the start and end of CPETs. Magnitudes of coefficients were described as small (0.1<0.3), medium (0.3<0.5) and large (≥0.5).9 All analyses were undertaken using SPSS V.26 (IBM), and a p<0.05 was considered significant.
Patient and public involvement
There is no patient or public involvement (PPI) to report in the design of this feasibility project, however, a questionnaire (online supplemental file 1) was used to assess experiences of participation within the trial, as previously mentioned in the ‘Feasibility’ section above.
Results
Participants
Participant characteristics are listed in table 1. Significant differences were observed between males and females for stature, absolute FEV1 and FVC, body fat percentage and FFM. Based on use of antifibrotic medication, significant differences were found for participants on antifibrotic medication who had both a lower body mass and BMI. However, there were no differences to be observed between groups for pulmonary function when normalised to percent predicted (table 1).
At baseline, mean (±SD) parameters of fitness for the n=24 to successfully complete one CPET were as follows for VO2peak; 1.32±0.40 L/min; 16.6±5.1 mL/kg/min; 26.4±6.8 mL/kgFFM/min; 76.6%±22.5%Predicted. For WRpeak, mean values were as follows: 92±37 W; 1.16±0.50 W/kg; 65.6%±23.8%Predicted.
The mean time difference between CPET and PFTs across the course of the study was 33±95 days (0.09±0.26 years), indicating that, on average, PFTs and CPET were separated by 1 month.
Feasibility: implementation
Two participants were excluded from performing CPET at their baseline visit by the attending clinician (hypertension, n=1; resting SpO2 <90%, n=1), resulting in n=24 undertaking at least one CPET. At the second visit, two further CPETs were not undertaken due to voluntary withdrawal of a participant (citing a lack of energy; n=1) and a participant experiencing a pulmonary embolism within the 4 weeks prior to study visit (n=1). At the third visit, three CPETs were not undertaken due to the aforementioned participant withdrawal (n=1), significant participant exertional desaturation (SpO2 <80%) on exertion (n=1), and one participant passed away in between study visits (n=1). Exclusions resulted in 67/78 of possible CPETs from the recruited n=26 being completed (figure 1) – an 86% completion rate.
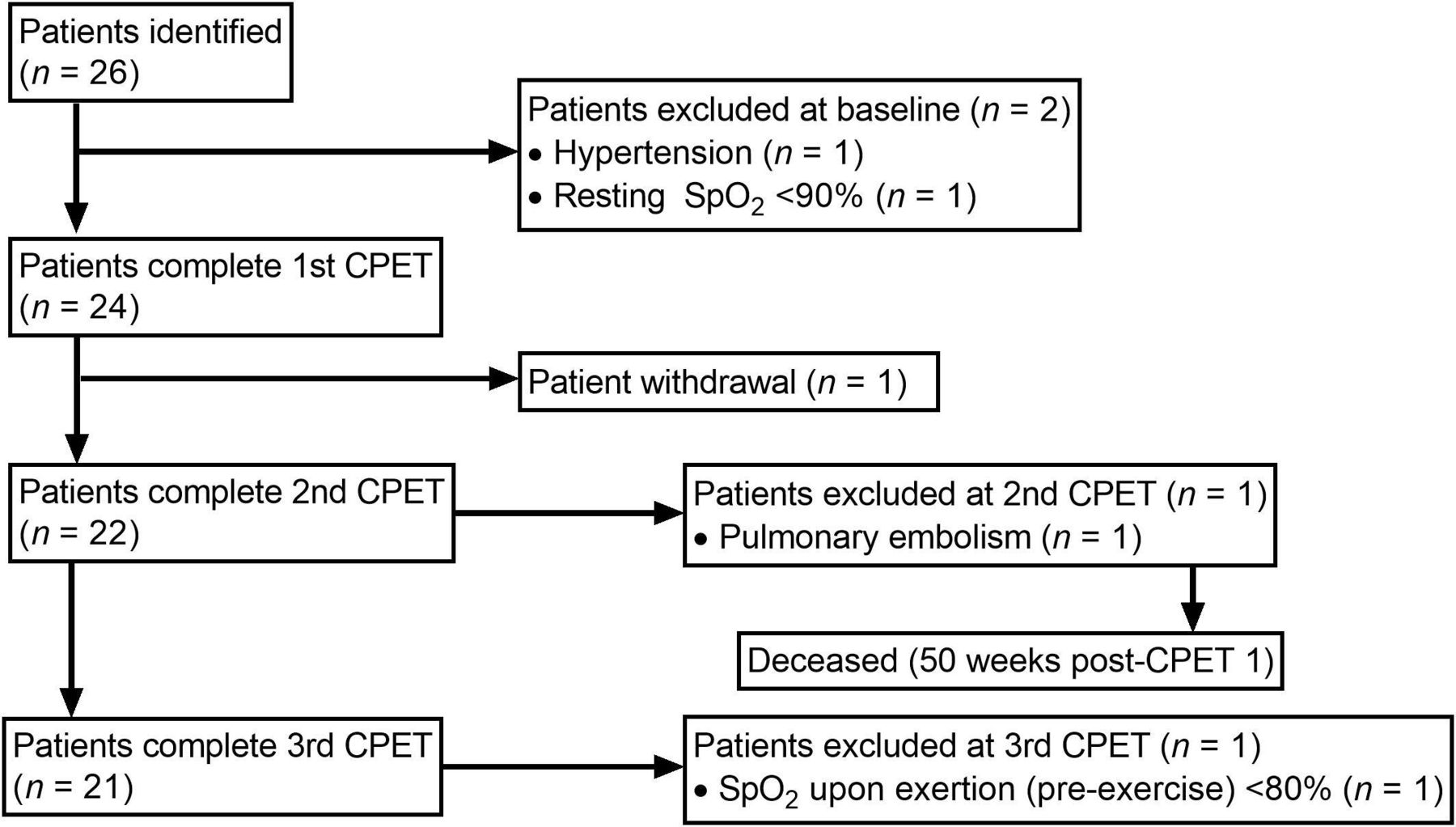
Flow chart detailing inclusion, exclusion and withdrawal of participants during study period. CPET, cardiopulmonary exercise testing; SpO2, oxygen saturation.
For n=21 participants who undertook all three CPETs, the mean duration between visits 1 and 2 was 26±12 weeks (range=12–49 weeks). Between visits 2 and 3, this mean duration was 15±5 weeks (10–28 weeks). Finally, mean duration between the first and last CPET was 41±14 weeks (23–65 weeks).
The majority of CPETs undertaken were satisfactorily completed, as patients successfully reached volitional exhaustion (n=42, 63%), compared with a number of participants who failed to reach exhaustion and tests were terminated by clinical staff. These reasons for clinical cessation included excessive desaturation (n=21, 31%), right bundle branch block (n=1, 1%) and a poor ECG trace, leading to a precautionary termination (n=1, 1%). One patient experienced excessive musculoskeletal pain (n=1, 1%) and one reason was not recorded (n=1, 1%).
Feasibility: practicality
Desaturation during exercise occurred in 63/67 CPETs, with n=3 CPETs experiencing no desaturation, and n=1 increasing SpO2 during the CPET (from 90% to 91%) as shown in figure 2. No relationship was evident between SpO2 at rest, and nadir SpO2 at termination of the CPET (figure 2). Nadir SpO2 and changes (Δ) in SpO2 held small to medium correlations with markers of fitness, as shown by relationships with WRpeak and VO2peak (table 2) when all n=67 CPETs were pooled for analysis. No significant correlations were reported when separated out by individual CPET.

{kind=link}
{kind=link}
Left: changes in peripheral capillary oxygen saturation (SpO2) from rest (pre) to end of test (post) for each CPET. Horizontal line at 80% indicates termination threshold for CPET as per American Thoracic Society (ATS)/American College of Chest Physicians (ACCP) recommendations. P value derived from repeated measures t-test. right: correlation between values of SPO2 at rest (pre) and end of CPET (post). All correlations presented as Pearson’s coefficient (r) and associated p value. PET, cardiopulmonary exercise testing.
Correlations between desaturation and parameters of fitness during cardiopulmonary exercise testing in patients with interstitial lung disease
In addition to the aforementioned right bundle branch block leading to CPET termination, ECG readings during the course of CPETs also revealed atrial fibrillation (n=1); possible atrial fibrillation (n=1); poor R-wave progression (n=1); T-wave inversion (n=1); asymptomatic widening of the QRS complex accompanied by T-wave inversion (n=1); and asymptomatic ventricular bigeminy (n=2), although these were not a cause for immediate CPET cessation. Referrals for 24-hour ECG monitoring were subsequently made by the attending clinical staff.
During exercise, all participants were able to maintain the pedalling rate as instructed, and the majority of individuals self-selected a cadence of 60–70 rpm, while two participants selected a cadence >70 rpm. Postexercise, one participant reported dizziness, although this ceased after a 5 min period and did not re-occur in subsequent CPETs. No other postexercise complications were reported.
Feasibility: acceptability and demand
A total of n=19 participants completed the post-trial evaluation. Of those to respond, participants rated their involvement in the study highly, and responded positively to the questions aimed at evaluating CPET. Responses for each question (mean±SD, range) were as follows: Q1 (1.5±0.6, 1–3), Q2 (6.7±0.5, 6–7), Q3 (1.7±1.3, 1–6). Qualitative reflections to the three questions are provided in table 3.
Selected qualitative responses to questions pertaining to exercise testing within the trial evaluation
Furthermore, in response to the semi-structured interview, participants reflected on their perspectives on the CPET, and in relation to other testing modalities. Broadly, CPET was viewed on positively:
I felt quite able and capable of doing it – the results will show but I was able to exert as much as I could and as long as I could – there must’ve been a parameter in which I was performing fairly well or they wouldn’t have allowed me to go on so long
I think the bike test is really good because it gives you so much information
For the most part, enjoyable! It obviously gets harder, but you’re allowed to stop so that’s alright
There were also some negative comments related to the testing procedures:
The bike test was OK – I was a little bit disappointed that they had to stop it [because of a right bundle block]
[the CPET] Very good – except the seat – that bicycle seat is most uncomfortable
Compared with other testing modalities, CPET was preferred to shuttle walks:
I prefer this definitely – it’s a tougher examination of your ability to move yourself and breathe. It’s a more accurate examination of your ability, more detailed. The shuttle walk test didn’t push me
I prefer the exercise bike test – the level of monitoring is much more detailed than a six min walk test
I don’t think they compare really because the shuttle walk test was very easy – it didn’t feel like a test really
The walk test is a nonsense – the bicycle test you are measuring everything, stamina, heart rate, the whole response, oxygen test, you’re doing everything. The walk test – you can choose how fast you walk – I could have gone on walking for a long time and it was up to me to choose the pace
I did the six minute walk test a lot in the trials – that always went OK. I loved doing the bike!
CPET was also preferred to spirometry:
Compared with spirometry, it’s easier – in [another hospital] I did two sorts – the one where you breathe in the mixture of gases and breathe out, one where you hold your breath out very quickly – but I thought the bike was better than that
Finally, spirometry was viewed on negatively by some:
[the spirometry] depends on who you’ve got taking it and you know what’s going to happen and it’s very hard to hold your breath when you‘ve got stuff blowing down the back of your throat; I don’t think it’s a very good indication of your health. I don’t like it at all.
The static lung function tests are very daunting and unpleasant to undergo
Patient and public involvement
While there was no PPI in the initial design of this study, general feedback from involvement in the trial revealed a desire from patients to be involved in future research and therefore a new patient-driven, research steering group was established (Exeter Patients in Collaboration for Pulmonary Fibrosis Research) in conjunction with the Royal Devon and Exeter National Health Service Foundation Trust and the College of Medicine & Health, University of Exeter. This group will be utilised to codesign trials following the outcome of this feasibility study.
Discussion
This study aimed to assess the feasibility, namely the implementation, practicality, acceptability and demand, of CPET in patients with ILD. The results have shown CPET can be feasibly undertaken in individuals with ILD, and is widely accepted by patients, therefore highlighting its prospective use as an alternative biomarker in this condition.
The feasibility of CPET was assessed with regards to clinically-driven, as well as patient-reported outcomes. First, evaluation of the implementation and practicality provides an objective assessment of whether this test could be used in a routine clinical setting, rather than a research-only environment. A successful 86% completion rate was achieved, and of the 11 tests not undertaken, six were due to immediate exclusion of participants at baseline due to contraindications, with a further two CPETs fitting this category from subsequent visits. The remaining three were accounted for by patient death and withdrawal from the study itself. These exclusions align with established absolute and relative contraindications to maximal exercise,6 although the authors are not aware of any previous studies to characterise the contraindications to exercise in ILD. Co-morbidities, including atrial fibrillation (which was also identified in our present cohort) have been reported in a previous study to use CPET, although this appears to be from a descriptive, rather than exclusionary perspective.10 This study also stated, unlike further CPET-based studies,4 11 12 that exercise was stopped by a clinician if necessary, although there is no further elaboration on any reasons if this occurred. Therefore, the present study is unique and advances our understanding in characterising clinical factors responsible for exclusion from, or cessation of, CPET in patients with ILD.
Within the current CPETs, the majority of participants desaturated, although only 31% to such an excessive extent that exercise had to be terminated, with the magnitude of desaturation in line with previous studies (eg, 87.7%±5.7%11; 90%±6%.13 Given that international recommendations propose exercise is terminated if SpO2 <80%,6 it is reassuring that our present results conform with previous studies and international guidelines, and that our patient group appears to be exercising safely within accepted norms, only prematurely stopping CPET in one-third of cases. In our sample, we noted two participants that presented with a normal pattern of desaturation, prior to a rapid drop in SpO2. For these two participants, CPET was terminated when SpO2 reached 80%, although this value continued to drop for ~5 s, resulting in two abnormally low nadir SpO2 values as seen in figure 2. This unexpected drop in SpO2 values was rare (ie, 2/67 CPETs), but it is important for clinicians to be aware of this potential risk. Future trials could consider the use of supplemental oxygen during CPET to offset this risk of desaturation (provided any equipment is technically compatible); although such hyperoxic conditions may affect the implementations of tests, and interpretation of results.14
Previous research has also suggested the degree to which patients desaturate during exercise testing is associated with baseline SpO2,15 although this does not appear to be supported in the present study as baseline and end-exercise SpO2 were not significantly correlated, even at the final CPET (figure 2), when disease severity may have progressed over the intervening period of time (up to 65 weeks for some participants). Moreover, desaturation and markers of fitness (VO2peak, WRpeak) held only small to medium correlations (table 2) – even when pooling all CPETs for increased power –indicating a level of homogeneity in the desaturation response to exercise in ILD. Thus, it is possible that disease presentation and severity has little effect on the risk of desaturation during exercise, and that alternative, non-disease related, mechanisms may be responsible and worthy of further investigation.
The prognostic value of CPET has been established previously, with VO2peak4 11 and VE/VCO212 being predictive of mortality in patients with IPF; and CPET is reported to be reproducible in restrictive lung disease.16 Therefore, this highlights the need to consider physiological measures, and not solely rely on radiological outcomes when monitoring fibrotic interstitial diseases and their subsequent change over time.3 17 Furthermore, as exercise intolerance in ILD is multifactorial,18 use of CPET can be utilised to ascertain causes of intolerance, as well as informing personalised approaches towards pulmonary rehabilitation and exercise regimens in patients.19
A personalised approach to exercise training was received with a mixed response in our cohort, with the mean score suggesting participants agreed with the principle of personalised regimens, although the qualitative responses provided contrasting views. Previous interviews of individuals with IPF show that patients feel exercise could benefit them physically and mentally, while proposing a preference for group-exercise,20 aligning with some of the perspectives put forward in the present study. Furthermore, current pulmonary rehabilitation guidelines state that personalisation is warranted to optimise such programmes.21 Therefore, CPET can be utilised to inform these processes, as the testing process itself has also been shown to be widely accepted in the present study.
Furthermore, a common theme that emerged was in relation to preference of CPET over alternative exercise tests, as well as spirometry, for which there appeared to be a dislike among this cohort of participants. While PFT are well established processes for detecting and characterising changes in disease status,22 and remain the gold-standard outcome measure in respiratory medicine, previous research reported that patients present with anxiety in relation to such tests,23 and find it difficult to translate such test results in relation to future exercise and activity ability.24 While the authors do not advocate for the removal, nor replacement of spirometry from clinical practice, a case can certainly be made for CPET to exist as an adjunct clinical measure alongside traditional PFT, for the benefit of clinicians and patients alike.
There are both strengths and limitations to be discussed with this study. Our study provides real-life data on how CPET is tolerated in this patient group, and thus provides clinicians with valuable insight into how to ingrain this modality of testing into services, and what contraindications and responses to anticipate. Moreover, the combination of quantitative and qualitative assessments not only empower the patient population and their voice within research and routine clinical assessment; but the description of physiological changes and logistical challenges associated with CPET, will prove exceptionally useful to the wider ILD community.
In contrast, we acknowledge that a sample size of 26 individuals can be interpreted as a limitation. This group is relatively homogeneous with regards to pulmonary function (as shown by lack of differences between sexes and antifibrotic usage in table 1) and can be considered mild in nature, with a sample that is composed predominantly of males with IPF. Therefore, there is a possibility this sample may not truly reflect wider patients responses to, and acceptability towards, CPET. However, previous exercise-based feasibility studies in ILD have recruited similar (or fewer) patient numbers,25 26 and thus our study is in line with such similarly designed studies. Moreover, given that IPF is the most common progressive ILD, and is more common in males,27 28 we conclude our sample is broadly reflective of the wider ILD population.
Conclusion
In conclusion, this study has shown CPET to be feasible within a clinical setting in terms of implementation and practicality, identifying reasons (and their number) for excluding patients from CPET, or stopping an exercise bout prematurely. Furthermore, CPET is acceptable by the intended user group (those with ILD). Therefore, this testing procedure should be considered for future use as an additional biomarker to evaluate prognosis and response to treatments in this patient population.
Data availability statement
Data are available on reasonable request. Please contact the corresponding author (CS).
Ethics statements
Ethics approval
Ethics approval for this study was granted by the Health Research Authority (IRAS #220189) following review by the South West (Frenchay) Research Ethics Committee (17/SW/0059).
Acknowledgments
The authors would like to acknowledge Dr Sarah Statton, Dr Tom Burden and Dr Ben Soar for assistance with CPET monitoring. Furthermore, the authors acknowledge ongoing support from staff at the Royal Devon and Exeter NHS Foundation Trust Interstitial Lung Disease Team and NIHR Exeter Clinical Research Facility.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MG, CW and CS conceived the work. OT, AD, LM, RW, BK and MG performed all testing. OT analysed data. OT, AD, LM, RW, BK, AS, MG, CW and CS interpreted data. OT, AD, LM, RW, BK, AS, MG, CW and CS drafted manuscript. OT, AD, LM, RW, BK, AS, MG, CW and CS critically reviewed manuscript and endorsed final version for submission. OT, AD, LM, RW, BK, AS, MG, CW and CS all agree to be accountable for all aspects of the work.
Funding This study was supported by an R&D grant from the Royal Devon & Exeter NHS Foundation Trust. AD was funded by the GW4 BioMed Medical Research Council Doctoral Training Partnership. RW was funded by a National Institute for Health Research (NIHR) Academic Clinical Fellowship. The NIHR Exeter Clinical Research Facility is a partnership between the University of Exeter Medical School College of Medicine and Health, and Royal Devon and Exeter NHS Foundation Trust. This project is supported by the National Institute for Health Research (NIHR) Exeter Clinical Research Facility.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Competing interests MG has received support to attend conferences and professional fees from Roche and Boehringer-Ingelheim.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.