Article Text

Abstract
Introduction Idiopathic pulmonary fibrosis (IPF) is an interstitial lung disease (ILD) with a poor prognosis. Early diagnosis and treatment of IPF may increase lifespan and preserve quality of life. Chest CT is the best test to diagnose IPF, but it is expensive and impractical as a screening test. Fine crackles on chest auscultation may be the only best to screen for IPF.
Methods We prospectively assessed the presence and type of crackles on chest auscultation in all patients referred to the ILD Clinic at the Kingston Health Sciences Center in Ontario, Canada. Clinicians with varying levels of experience recorded the presence of fine crackles, coarse crackles or both independently and unaware of the final diagnosis. We applied multinomial logistic regression to adjust for ILD severity and factors that could affect the identification of crackles.
Results We evaluated 290 patients referred to the ILD Clinic. On initial presentation, 93% of patients with IPF and 73% of patients with non-IPF ILD had fine crackles on auscultation. In patients with IPF, fine crackles were more common than cough (86%), dyspnoea (80%), low diffusing capacity (87%), total lung capacity (57%) and forced vital capacity (50%). There was 90% observer agreement in identifying fine crackles at a subsequent visit. In multiple regression analysis, the identification of fine crackles was unaffected by lung function, symptoms, emphysema, chronic obstructive pulmonary disease, obesity or clinician experience (p>0.05).
Conclusions Fine crackles on chest auscultation are a sensitive and robust screening tool that can lead to early diagnosis and treatment of patients with IPF.
- interstitial fibrosis
Data availability statement
Data are available upon reasonable request. Requests can be made to Dr. Onofre Moran-Mendoza.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the question?
Are fine crackles on chest auscultation useful in the early diagnosis of idiopathic pulmonary fibrosis (IPF) and other interstitial lung diseases?
What is the bottom line?
Early diagnosis and treatment of IPF may increase lifespan and preserve quality of life. Chest CT is the best test to screen and diagnose IPF, but it is expensive and impractical as a screening test. Fine crackles on chest auscultation may be the most practical tool to diagnose IPF early.
Why read on?
Our study shows that fine crackles on chest auscultation are a sensitive and robust screening tool that can allow for early diagnosis and treatment of patients with IPF.
Introduction
Interstitial lung diseases (ILDs) are a diverse group of diseases that cause fibrosis or inflammation of the lung parenchyma1 and differ in their aetiology but share a similar radiological and clinical pattern. Treatment and prognosis of ILD typically depend on the underlying ILD subtype, highlighting the importance of accurate classification and diagnosis. The therapeutic options for ILD vary depending on the final diagnosis and include steroids and/or immunosuppressants and antifibrotic drugs.2 3
Idiopathic pulmonary fibrosis (IPF) is a chronic, progressive, fibrosing ILD of unknown cause that usually affects people older than 60 years of age and has a poor prognosis, with a median survival of 2–3 years from the time of diagnosis.4–6 IPF should be considered in all adult patients with unexplained dyspnoea, and commonly presents with cough, bibasilar inspiratory crackles and finger clubbing.5 It has been shown that the diagnosis and initiation of treatment in IPF can be delayed by 2 years or more, resulting in increased mortality.7 There are currently two available antifibrotic drugs—nintedanib and pirfenidone—that can slow down the progression of the disease, and likely decrease mortality.8–12 Early referral of patients with suspected IPF to specialists or ILD centres can lead to earlier treatment and better prognosis.13
High-resolution chest CT is the best noninvasive test to diagnose ILD, but it is expensive and impractical to be used as a screening test. It has been suggested that the assessment of fine (Velcro) crackles by chest auscultation is currently the only realistic means to diagnose IPF earlier.14 15 However, no study, thus, far has evaluated the role of fine crackles in the early diagnosis of IPF.
The objective of our study was to assess the usefulness of fine crackles in the early diagnosis of IPF and other forms of ILD.
Methods
Study design, setting and participants
In this prospective and prolective study, we assessed the presence and type of crackles on chest auscultation in all new patients referred to the ILD Clinic at the Kingston Health Sciences Center (KHSC) in Ontario, Canada, between 2013 and 2018. New patients are referred to the KHSC ILD clinic by their family physicians because of suspected ILD based on chest CT findings. Patients included in this study had no prior diagnosis of IPF and some of them were asymptomatic and/or had normal pulmonary function tests (PFTs). Before the final diagnosis of the ILD was established, clinicians with different levels of experience and training performed the chest examination and recorded the presence and type of crackles on a standardised data collection form, blinded to the assessment of other clinicians and to the final diagnosis. Each clinician used their own stethoscope and placed it directly on the skin of the patient during their routine chest auscultation, which had to encompass the entirety of both hemithoraces anteriorly and posteriorly but was performed as per their own clinical practice. Clinicians did not require additional training on chest auscultation to take part in this study.
At the KHSC ILD clinic, we follow the recommendations of current international guidelines to diagnose IPF and other ILDs.5 6 16 ILD is defined on chest CT as per the chest radiologist diagnosis. The diagnosis of IPF was established when a usual interstitial pneumonia (UIP) or probable UIP pattern was reported by chest radiologists on CT or by a lung pathologist from a lung biopsy, after known causes of were ruled out. All patients eventually diagnosed with IPF or other ILD who had at least two clinic visits were included in this study.
Variables of interest
Main variables
The presence and type of crackles were recorded by clinicians at the initial and subsequent clinic visit on each patient as: (a) no crackles, (b) fine crackles, (c) coarse crackles and (d) both, fine and coarse crackles.
Fine crackles are nonmusical discontinuous sounds best heard on mid-to-late inspiration, unaffected by cough. They are shorter in duration and higher in pitch than coarse crackles.17 18 Because fine crackles have a sound similar to that heard when strips of Velcro are separated they are also called velcro crackles.17
For this study, participating clinicians (medical residents of different specialties, respirology fellows, ILD fellows and a respirologist attending) were asked to record crackles as ‘fine’ if they persisted after several breaths and sounded either like ‘velcro’ or like the sound produced by ‘rubbing their hair between their fingers’.
Coarse crackles have lower pitch and frequency, have a ‘popping’ quality sound and, in some conditions, can resolve after asking the patient to cough.17 19 Clinicians participating in the study were asked to record as ‘coarse’ any crackles other than fine crackles: examples of coarse crackles given to clinicians were the sound of ‘walking on ice’ or the sound produced by ‘squeezing a paper bag, a cereal bag or cellophane bag’.
Potential confounders
We assessed variables that may influence the identification of crackles on auscultation: 1. The severity of ILD was evaluated through the severity of dyspnoea as per the British Medical Research Council scale, the presence of cough and through PFTs.
PFTs were performed at the KHSC pulmonary function laboratory as per current guidelines20 21 the same week, and if unfeasible within 2–4 weeks of the initial clinic assessment. We measured forced vital capacity (FVC), forced expiratory volume in one second (FEV1), FEV1/FVC ratio, total lung capacity (TLC) and the carbon monoxide diffusing capacity (DLco) and reported them as percent of predicted for the corresponding age, gender, and height.22
The presence of emphysema on chest CT, chronic obstructive pulmonary disease (COPD), defined as postbronchodilator FEV1/FVC <0.70 in current or former smokers.
Obesity, defined as body mass index ≥30 Kg/m2.
The experience of clinicians performing chest auscultation, classified as: (a) staff respirologist, (b) ILD fellows and (c) residents, which included respirology fellows and medical residents (mostly Internal Medicine Residents).
In addition, we evaluated the agreement of the presence and type of crackles between clinicians at the initial and subsequent clinic visits.
Statistical analysis
We used frequencies to describe categorical variables and mean and SD for continuous variables. The auscultatory findings were analysed using the same categories as recorded: (a) no crackles, (b) fine crackles, (c) coarse crackles and (d) both fine and coarse crackles. The identification of crackles was stratified by diagnosis (IPF vs non-IPF), as well as by patient and clinician characteristics that could affect the identification of crackles (potential confounders above).
The association between the auscultation of crackles and patient and clinician characteristics was analysed with the χ2 test; and we applied Bonferroni’s adjustment for multiple comparisons at a nominal p value of 0.05. We used multinomial logistic regression to assess the usefulness of crackles in diagnosing IPF, adjusting for patient and clinician characteristics, introducing all the characteristics in the model simultaneously as well as by backward and forward stepwise. We assessed independently for patients with IPF and non-IPF, the interaction between the presence and type of crackles and all the potential confounders.
To evaluate the agreement of clinicians identifying fine and coarse crackles between the initial and the subsequent clinic visits, we used percent agreement, and the kappa test was used to correct for agreement expected by chance.23 All statistical analyses were performed with SPSS Statistics V.25.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research.
Role of the funding source
There was no funding source for this study. All authors had full access to all the data in the study.
Results
Study population
We included a total of 290 patients with ILD in this study, which encompassed all incident cases assessed in the ILD clinic during the study period. Fifty-eight per cent of patients were men, 27% had emphysema on chest CT, 10% had COPD and 47% were obese. On presentation, 23% of our patients had no dyspnoea, 20% had no cough and 9% had neither dyspnoea nor cough: the reason for referral of these patients was incidental interstitial lung abnormalities on chest or abdominal CT done for other reasons (66%), crackles heard on chest auscultation by the family physician (17%) and dyspnoea or cough that had resolved at time of assessment in the ILD clinic (17%). At the initial clinic visit, 54% of patients with ILD had normal FVC, 50% had normal TLC and 16% had normal DLco.
After completing all assessments, 129 of the 290 patients (45%) were eventually diagnosed with IPF and the remaining 55% were diagnosed with other types of ILD: 17% with connective tissue disease (CTD), 13% with hypersensitivity pneumonitis, 7% with idiopathic nonspecific interstitial pneumonia (NSIP) and the rest (18%) with other types of ILD (table 1).
Characteristics of patients with interstitial lung disease at the time of initial clinic visit (n=290)
There was no significant difference in FVC, TLC or DLco between patients with IPF and non-IPF ILD (table 2).
Pulmonary function test results at the time of initial clinic visit according to type of interstitial lung disease
Auscultation of crackles
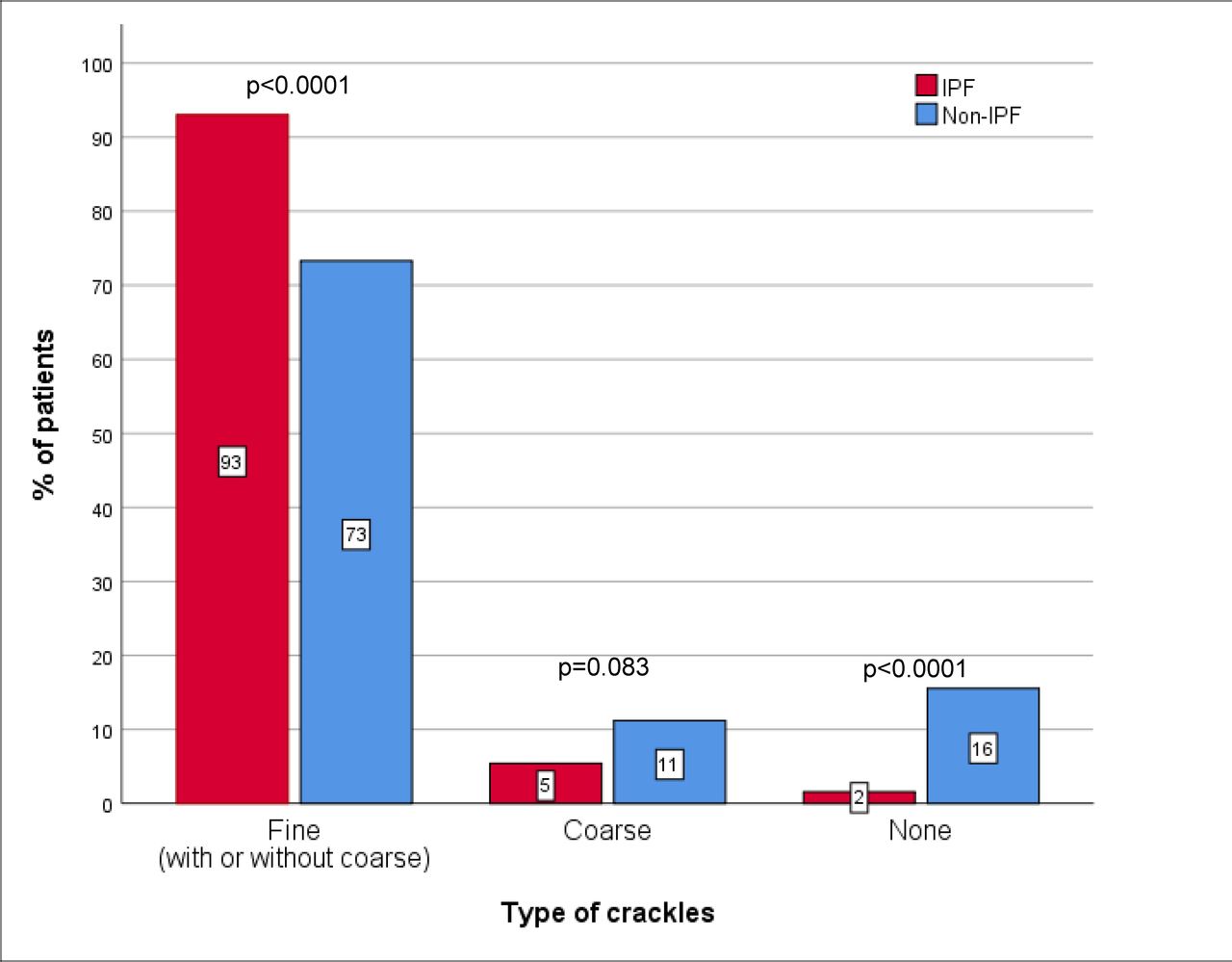
A total of 21 clinicians, including medical residents, respirology fellows, ILD fellows and an attending respirologist, recorded independently the presence and type of crackles identified. On initial presentation, 93% of patients with IPF had fine crackles on chest auscultation, alone or combined with coarse crackles, compared with 73% of patients with non-IPF ILD (p<0.001); and 98% of patients with IPF had some types of crackles on auscultation (figure 1 and table 3).
{kind=link}
Frequency of crackles during chest exam at the time of initial clinic visit according to IPF and non-IPF diagnosis at initial clinic visit. P values obtained from Pearson χ2 test. IPF, idiopathic pulmonary fibrosis.
Auscultation of crackles on chest exam at the initial clinic visit according to type of interstitial lung disease (n=290)
The presence of fine crackles alone or combined with coarse crackles varied among different non-IPF ILDs, ranging from 37.5% in smoking-related ILD to ≥80% in unclassifiable ILD, CTD-related ILD and NSIP (table 3).
In the 129 patients with IPF, the presence of fine crackles on auscultation (93%) was more common than cough (86%), dyspnoea (80%), low diffusing capacity (87%), low TLC (57%) and low FVC (50%).
The presence or absence of symptoms was not associated with the presence or type of crackles identified on auscultation in patients with IPF (p>0.21) or with non-IPF ILD (p>0.42). Having normal or abnormal lung function was unrelated with the presence or type of crackles identified in patients with IPF or non-IPF (p>0.05), as shown in table 4.
Auscultation of crackles at the initial clinic visit in patients according to symptoms (n=290) and lung function*
Neither emphysema (p≥0.10), COPD (p≥0.54) nor obesity (p≥0.78) was associated with the presence or type of crackles. Similarly, the experience of clinicians did not influence the identification of crackles on auscultation (p≥0.10), as shown in table 5.
Auscultation of crackles at the initial clinic visit according to patient and clinician characteristics (n=290)
Agreement between clinic visits
There were 171 patients who had the presence and type of crackles assessed at a subsequent clinic visit, of whom 47% had IPF and 53% had non-IPF ILD. The mean time between the initial and subsequent visits was 23 weeks (SD 4.7 weeks). As shown in table 6, 90% of patients with fine crackles—with or without coarse crackles— and 40% of those with coarse crackles on the initial clinic visit had the same type of crackles identified on the subsequent visit (overall agreement 84%; kappa 0.421; p<0.001). Clinicians assessing the presence and type of crackles between the initial and subsequent visit were different in 50% of cases.
Agreement in presence and type crackles on auscultation between initial and subsequent clinic visits
Multinomial logistic regression
After adjusting for potential confounding variables (cough, dyspnoea, FVC, TLC, Dlco, emphysema on chest CT, COPD, obesity and experience of the clinician performing the chest auscultation), the odds of finding fine crackles—alone or in combination with coarse crackles—were significantly higher in patients with IPF than in patients with non-IPF ILD (OR 12.6; 95% CI 2.9 to 55; p<0.001). The odds of finding fine crackles on auscultation were not associated with any of the potential confounding variables. The results were unchanged whether all variables were entered simultaneously or through forward or backward stepwise in the logistic regression model.
None of the interactions between the presence and type of crackles (no crackles, fine crackles, coarse crackles or both) and patient and clinician characteristics were statistically significant for patients with IPF or non-IPF. Thus, the proper identification of crackles was not affected by the presence or absence of cough, dyspnoea, emphysema, COPD, obesity, the experience of clinicians or normal/abnormal FVC, TLC or DLco.
Discussion
We found that fine crackles were present in almost all (93%) patients with IPF and in the majority (70%) of patients with non-IPF ILD; and that almost all patients (98%) with IPF had either fine or coarse crackles on auscultation. Also, we found that the identification of fine crackles in IPF was not influenced by variables that could affect their identification: normal or abnormal lung function, symptoms, emphysema, COPD, obesity or the experience of the clinician performing the chest auscultation. As such, our results suggest that fine crackles are a robust marker of IPF and other ILD across patients with different clinical phenotypes.
Fine crackles on chest auscultation have been described typically in IPF,17 and their prevalence has been reported from 18% in patients with sarcoidosis to 60% in patients with ‘usual interstitial pneumonia’ and in patients with asbestosis.24–26
However, to our knowledge, the present study is the first to assess the diagnostic value of fine crackles on chest auscultation in patients with IPF and other forms of ILD. Our study is also the first to assess the presence of fine crackles at the initial clinic visit, before a diagnosis of an ILD was established, and adjusting for potential confounders that could affect the identification of crackles.
Sellares et al27 reported that 100% of their patients with IPF had ‘velcro crackles’ on auscultation; however, they included only 17 patients with IPF in their study, a very small number to draw robust conclusions. In addition, the authors did not assess the role of potential confounders that could have influenced the identification of crackles.
Fine crackles appear to be the most sensitive finding for the diagnosis of IPF, and perhaps other forms of ILD as well. We found fine crackles in 93% of our patients with IPF, more commonly than dyspnoea or cough (up to 86% of patients); and more common than a restrictive pattern on PFTs or a low diffusing capacity.
In our study, after controlling for variables affecting auscultatory findings, we found that fine crackles are as likely to be found in early as in advanced IPF; hence, they can be a very useful screening or diagnostic test at any stage of the disease. Neither having emphysema, COPD nor obesity—which could decrease the transmission of sounds through the chest—affected the proper identification of fine crackles by clinicians. We had 21 clinicians with different levels of training and experience performing the chest auscultation. The level of education or experience did not influence the ability of the clinician to identify fine crackles; thus, our results suggest that significant training is not required to differentiate between fine and coarse crackles as long as proper description to identify them is provided to clinicians.
We asked clinicians to perform the chest auscultation as per their own clinical practice, rather than using specific auscultatory landmarks, to make our study results more generalisable to diverse clinical practices.
On the other hand, almost all patients (~90%) with ILD who had fine crackles on the initial visit also had fine crackles identified on the subsequent visit, even though half of clinicians performing the chest examination on the second visit were different, which supports that fine crackles on auscultation are a robust finding in patients with ILD. Previous investigations have reported high reliability of crackles during auscultation in patients with asbestosis,28 but to our knowledge, no study has previously reported the reliability of fine crackles in patients with IPF.
Fine crackles can be explained by the presence of interstitial lung fibrosis, but some of our patients with IPF also had coarse crackles, likely explained by the presence of airway secretions due to concomitant chronic bronchitis or an airway process.17
Electronic/digital analyses of lung sounds are a promising diagnostic tool in the identification of ILD. A study reported that the digital analyses of lung sounds had a sensitivity of 93% and a specificity of 77% in identifying ‘velcro crackles’ in a small sample of patients with rheumatoid arthritis and ILD,29 while others found them useful to predict the presence of reticulation and honeycombing on HRCT in patients with fibrotic lung diseases30 31 and even to differentiate crackles due to IPF from crackles due to congestive heart failure and pneumonia.32 However, digital analyses of lung sounds require further validation before they can be incorporated in routine clinical practice for the diagnosis of ILD.
The present study has a number of limitations: the clinicians performing chest auscultation were medical residents, respirology fellows, ILD fellows and an attending respirologist; however, we did not include primary care physicians; therefore, the findings may not apply to them.
Clinicians participating in the study were asked to perform the chest auscultation as they normally do during their clinical assessments, using their own stethoscopes, and to report ‘fine crackles’ if they sounded either like ‘velcro’ or like the sound produced by ‘rubbing your hair between your fingers’. Lack of standardisation of a diagnostic test could decrease the internal validity of the results; despite this, in the present study, clinicians reported the presence of fine crackles in >90% of patients regardless of their level of training or experience. Similarly, almost 90% of patients who had fine crackles on the initial clinic visit also had them at the subsequent visit, even though half of clinicians were different, supporting the external validity of our results. Our study was performed in a single centre in Canada, which could limit the generalisability of the results, but the clinicians participating in our study were trained in different medical schools in North America, Europe and the Middle East, which would also increase the external validity of our results.
It is possible that clinicians performing the chest auscultation in our study were more likely to report crackles by assessing patients attending an ILD clinic; yet this would not explain the significantly higher prevalence of fine crackles in patients with IPF compared with patients with non-IPF ILD, particularly when clinicians were unaware of the final diagnosis at the time of initial assessment. Conversely, the final ILD diagnosis was not influenced by the presence or type of crackles on chest examination at the initial clinic visit because the diagnosis of the ILD in our clinic follows current guidelines, which do not incorporate auscultatory findings in the diagnosis.5 6 16
Finally, in theory, a population-based screening study would be ideal to identify patients with ILD early in their disease; however, this would be ethically unfeasible due to the risk of exposing large numbers of asymptomatic individuals to radiation by performing chest HCRT in a population. However, our study is the closest to a population-based study, because at the KHSC ILD clinic, we frequently assess patients with no symptoms and found incidentally to have ILD on imaging studies done for other reasons. This unique advantage of our ILD clinic allowed us to include patients diagnosed in the very early stages of their disease, as would occur in a screening study.
Conclusion
Our study shows that fine crackles are present in almost all patients with IPF, including asymptomatic patients and patients with normal PFTs, and can be properly identified regardless of patients having emphysema, COPD, obesity or the experience of the clinician performing the chest auscultation. Therefore, our results suggest that fine crackles on chest auscultation are a sensitive, robust and useful screening tool that can lead to early diagnosis and treatment of patients with IPF, and likely other ILDs. This is particularly important given the current availability of antifibrotic drugs that can slow down the progression of IPF and other progressing fibrotic lung diseases.
Data availability statement
Data are available upon reasonable request. Requests can be made to Dr. Onofre Moran-Mendoza.
Ethics statements
Ethics approval
The study was approved by the Queen’s University Health Research Ethics Board (TRAQ number 6023960).
Acknowledgments
We acknowledge the contributions of our former Fellows at the Interstitial Lung Diseases Program at Queen’s University, Dr Muhanad Hawari, Dr Sami Alyami, Dr Sharina Aldhaheri and Dr Bader Alharthi, as well as all the residents rotating in the Division of Respiratory and Sleep Medicine at Queen’s University who participated in this study identifying and recording the presence and type of crackles on chest auscultation. The main author acknowledges Mrs Geraldine MacDonald for the review of the manuscript.
References
Footnotes
Contributors OM-M accepts full responsibility for data integrity and analysis in this manuscript. OM-M designed the research study. All authors participated in data collection data analysis, and manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests OM-M has received consulting and speaking honoraria from Boehringer Ingelheim and F. Hoffmann-La Roche, none influencing this work. TR and SA declare no conflict of interest.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.