Article Text

Abstract
Background The majority of patients with SARS-CoV-2 infection are diagnosed and managed as outpatients; however, little is known about the burden of pulmonary disease in this setting. Lung ultrasound (LUS) is a convenient tool for detection of COVID-19 pneumonia. Identifying SARS-CoV-2 infected outpatients with pulmonary disease may be important for early risk stratification.
Objectives To investigate the prevalence, natural history and clinical significance of pulmonary disease in outpatients with SARS-CoV-2.
Methods SARS-CoV-2 PCR positive outpatients (CV(+)) were assessed with LUS to identify the presence of interstitial pneumonia. Studies were considered positive based on the presence of B-lines, pleural irregularity and consolidations. A subset of patients underwent longitudinal examinations. Correlations between LUS findings and patient symptoms, demographics, comorbidities and clinical outcomes over 8 weeks were evaluated.
Results 102 CV(+) patients underwent LUS with 42 (41%) demonstrating pulmonary involvement. Baseline LUS severity scores correlated with shortness of breath on multivariate analysis. Of the CV(+) patients followed longitudinally, a majority showed improvement or resolution in LUS findings after 1–2 weeks. Only one patient in the CV(+) cohort was briefly hospitalised, and no patient died or required mechanical ventilation.
Conclusion We found a high prevalence of LUS findings in outpatients with SARS-CoV-2 infection. Given the pervasiveness of pulmonary disease across a broad spectrum of LUS severity scores and lack of adverse outcomes, our findings suggest that LUS may not be a useful as a risk stratification tool in SARS-CoV-2 in the general outpatient population.
- COVID-19
- imaging/CT MRI etc
- pneumonia
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data relevant to the study are included in the article and supplementary information. Additional deidentified participant data is available on reasonable request to the corresponding author, Robert Fairchild (rfairchi@stanford.edu).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
The high prevalence of pulmonary disease by LUS in SARS-CoV-2 infected outpatients (41%), and the absence of clinical outcome correlatives, suggests limited utility of this technique for risk stratification and surveillance in the outpatient setting.
This is the first study to investigate the prevalence of pulmonary findings in outpatients with SARS-CoV-2 infection using LUS and the largest outpatient COVID-19 study of the general population to date. It provides longitudinal data on a subset of patients and describes the natural evolution of COVID-19 by LUS.
Introduction
SARS-CoV-2 infection presents heterogeneously, ranging from asymptomatic to severe, with an estimated mortality rate of 2.3%.1 2 The majority of cases are mild or asymptomatic, but a significant proportion requires hospitalisation or ICU admission.1 While increased age, male gender and specific comorbidities are associated with higher rates of hospitalisation and mortality, individualised risk stratification of patients early in the disease course remains a challenge, especially in the outpatient setting.3
Given the lack of radiation, ease of use, portability and low cost,4 ultrasound may be a useful tool in the management of COVID-19. COVID-19 pneumonia is commonly located in a subpleural, peripheral and basilar distribution on CT imaging,5–8 which makes it amenable to detection by lung ultrasound (LUS). Protocols targeting the posterior and lateral aspects of lungs allow detection of the disease and maximise provider safety.9–11 Ultrasound has been used for triage in the emergency department (ED)12–15 and for risk stratification and disease monitoring in the hospital, reducing personnel and equipment needed for lung monitoring on hospital wards,16 in the ICU4 16 17 and in postacute rehabilitation.18
Typical LUS findings associated with COVID-19 pneumonia include B-lines, pleural irregularity and consolidations.19 Although LUS has utility in caring for hospitalised patients, it has not been widely studied in the outpatient setting. As mild cases of COVID-19 are not routinely evaluated with imaging, the prevalence and significance of lung pathology in this cohort of patients is not well characterised. Previous work has demonstrated an association between subpleural consolidations on LUS and dyspnoea in symptomatic healthcare workers, but these patients were not followed longitudinally.20 A study of patients referred to the ED from a primary care office following LUS demonstrated an association between coalescent B-lines and hospital admission.21 None of these studies adequately addressed the utility of LUS for risk stratification of outpatients.
In light of prior work and our experience using LUS to identify interstitial lung disease in systemic sclerosis,22 we conducted this study using LUS to assess the burden, natural history and clinical significance of pulmonary disease in consecutive SARS-CoV-2 PCR positive outpatients, in order to better understand the potential role of LUS in the outpatient management of SARS-CoV-2 infection.
Methods
Study population
This is a prospective cohort study conducted at an academic, tertiary care centre. Patients were identified using the STAnford medicine Research data Repository, an informatics platform that allows for real-time cohort discovery and chart review. Adult English and Spanish speaking patients with a positive SARS-CoV-2 PCR in the past 14 days (CV(+)) underwent an initial screening via chart review. Patients with a history of parenchymal lung disease, hospitalisation for any cause in the past month, previous CV(+) outside of the 14-day window, current pregnancy or who had recently used corticosteroids or any investigational medication for COVID-19 in the setting of a clinical trial were excluded. Participants underwent informed consent and initial ultrasound evaluation at the Stanford CROWN clinic—a dedicated outpatient clinic for COVID-19 patients. During this visit, demographics, baseline symptoms and resting oxygen saturation were collected.
Control participants were enrolled from a convenience sample of age-balanced and sex-balanced community members who had a negative SARS-CoV-2 PCR test (CV(-)) in the prior 14 days. Exclusion criteria included history of parenchymal lung disease, current pregnancy, prior known SARS-CoV-2 infection and any potential COVID-19 associated symptoms that prompted testing.
Patient involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
LUS examination
LUS examination was based on a modification of previously published methods,10 focusing on six posterior lung zones: bilateral posterolateral, subscapular and paravertebral. Patients were positioned sitting upright with their lower to mid back exposed to the ultrasonographer. At each lung zone, an area spanning from the inferior margin of the lung up to the level of the inferior scapula was interrogated, and a single 4 s movie clip was acquired at the area of maximal pathology for each of the six lung zones. LUS examinations were performed in B-mode using a GE Logiq E using a medium frequency linear probe. Ultrasound frequency was typically 12 MHz, with downward adjustment as needed to improve signal penetration. All LUS examinations were performed or supervised by an experienced ultrasonographer (RMF), who has performed over 400 LUS examinations over the last 5 years. All equipment and clinical space was thoroughly disinfected after each patient encounter using alcohol-free quaternary ammonia disinfecting wipes as per infection control and the Centers for Disease Control and Prevention guidelines.
To identify patients for follow-up LUS imaging, and for ethical considerations, LUS examinations were preliminarily screened positive or negative at the time of acquisition according to previously published methods.9 23 All patients were offered the option of follow-up LUS examination.
LUS severity scoring
LUS videos were randomised and scored independently by two experienced sonographers (RMF and AH) on completion of the study. For each patient, the severity of B-lines (artefactual hyperechoic rays extending from the pleural surface), pleural irregularity and consolidations were determined for each of the six lung zones: B-lines (quantity of B-lines; 0=none; 1=1–2; 2=3 or more; 3=confluent), pleural irregularity (quantity of discontinuities or irregularities in the pleural surface; 0=none; 1=1–2; 2=several; 3=diffuse) and consolidations (0=none; 2=small (<50% of the field of view); 3=large (>50% of the field of view)). Consensus scores for discordant reads were obtained by discussion in all cases. The single highest feature score (0–3) from each of the six lung zones were summed to obtain an overall severity score ranging from 0 (normal) to 18 (most severe). For all analyses, patients with positive lung ultrasound (LUS(+)) refer to severity scores>0 while negative lung ultrasound (LUS(−)) refer to severity scores=0. In the group that underwent longitudinal exams, a severity score difference of >1 point was used to define improvement or worsening between exams.
Data collection and outcomes
Additional baseline, longitudinal and outcomes data were obtained by participant surveys at baseline and 8-week follow-up and by review of the electronic medical record whenever possible. Data collected included baseline symptoms, longitudinal symptoms, smoking status, body mass index (BMI), glucocorticoid use, CT imaging data, and outcomes of hospitalisation, need for mechanical ventilation and death.
Statistical analysis
Baseline characteristics of patients receiving LUS examination were described. The proportion of LUS(+) patients between the CV(+) and CV(−) groups was compared using the two-sample test for equality of proportions with continuity correction. Inter-rater reliability was calculated for the three components of the ultrasound severity score (B-lines, pleural irregularity and consolidations scored semiquantitatively from 0 to 3) by calculating the Cohen’s kappa statistic. CV(+) patients with persistent or worsening LUS at follow-up were compared with patients with improvement in LUS using the two-sample Wilcoxon test for continuous variables and the Fisher’s exact test for categorical variables. Patients that were CV(+)/LUS(+) and those that were CV(+)/LUS(−) at baseline were compared using the Pearson’s χ2 test for categorical variables. Multivariable logistic regression was used in the CV(+) cohort to assess the association between baseline symptoms of fever, cough or shortness of breath (SOB) with the total LUS severity score, adjusting for age, sex, African American and Hispanic race/ethnicity, smoking status and BMI.
CV(+) patients with missing 8-week follow-up survey data were excluded from longitudinal analyses (13 patients). We assessed significance at the 0.05 level. All statistical analyses were performed using R statistical software. This study was approved by our institutional review board.
Results
Patient cohort
Patients from June 2020 to October 2020 were screened and enrolled (online supplemental figure 1). Of 2371 patients who underwent initial screening, 1598 patients did not meet inclusion criteria due to lack of a provider at our institution (57%), lack of interest in participating in research (17%), hospitalisation within the past month (10%) and additional CV(+) testing outside the 14-day window of this study (6%). Of the remaining 773 patients, further screening and contact eligibility criteria reduced the pool to 596 patients. Of these patients, 311 were contacted for potential enrolment, 120 agreed to participate and 102 were enrolled (online supplemental figure 1). Eight-week follow-up surveys were completed in 89 patients, with 13 non-respondents. Longitudinal LUS exams were performed on 30 patients (29%).
Supplemental material
Of the 102 CV(+) patients enrolled, the mean age was 43.6 years and 52% were female, with diverse racial and ethnic backgrounds (table 1). The mean BMI was 26.7 kg/m2, 6% of patients were current smokers and 20% were prior smokers. The most common symptoms at baseline were headache (76%), cough (70%), myalgia (68%) and loss of smell or taste (64%). We enrolled 14 healthy control CV(−) patients with a mean age of 43.8, of whom 71% were female. At the time of LUS examination, all enrollees presented with oxygen saturations greater than 94%.
Baseline patient characteristics and symptoms of SARS-CoV-2 positive (CV(+)) patients.
LUS examinations
A total of 158 LUS examinations were performed, including 102 baseline and 42 follow-up examinations in CV(+) patients, and 14 baseline LUS examinations in CV(−) control patients. The median time between CV(+) testing and baseline LUS was 6.8 days (IQR 5.8–8.8, range 2–14 days). Baseline LUS severity scores, obtained by summing the highest LUS feature score in each of the six lung zones (maximum=18), ranged from 0 to 14. In the CV(+) subjects, 42 (41%) were LUS(+) and 60 (59%) were LUS(−) (figure 1). In comparison, 14 (100%) of the CV(−) control patients were LUS(−), with a significant difference in the proportion of negative LUS between CV(+) and CV(−) patients (p=0.003). Because our study was focused on an outpatient cohort, only two patients had CT imaging of the chest around the time of baseline LUS, and both CT scans showed concordance with LUS findings (figure 2).
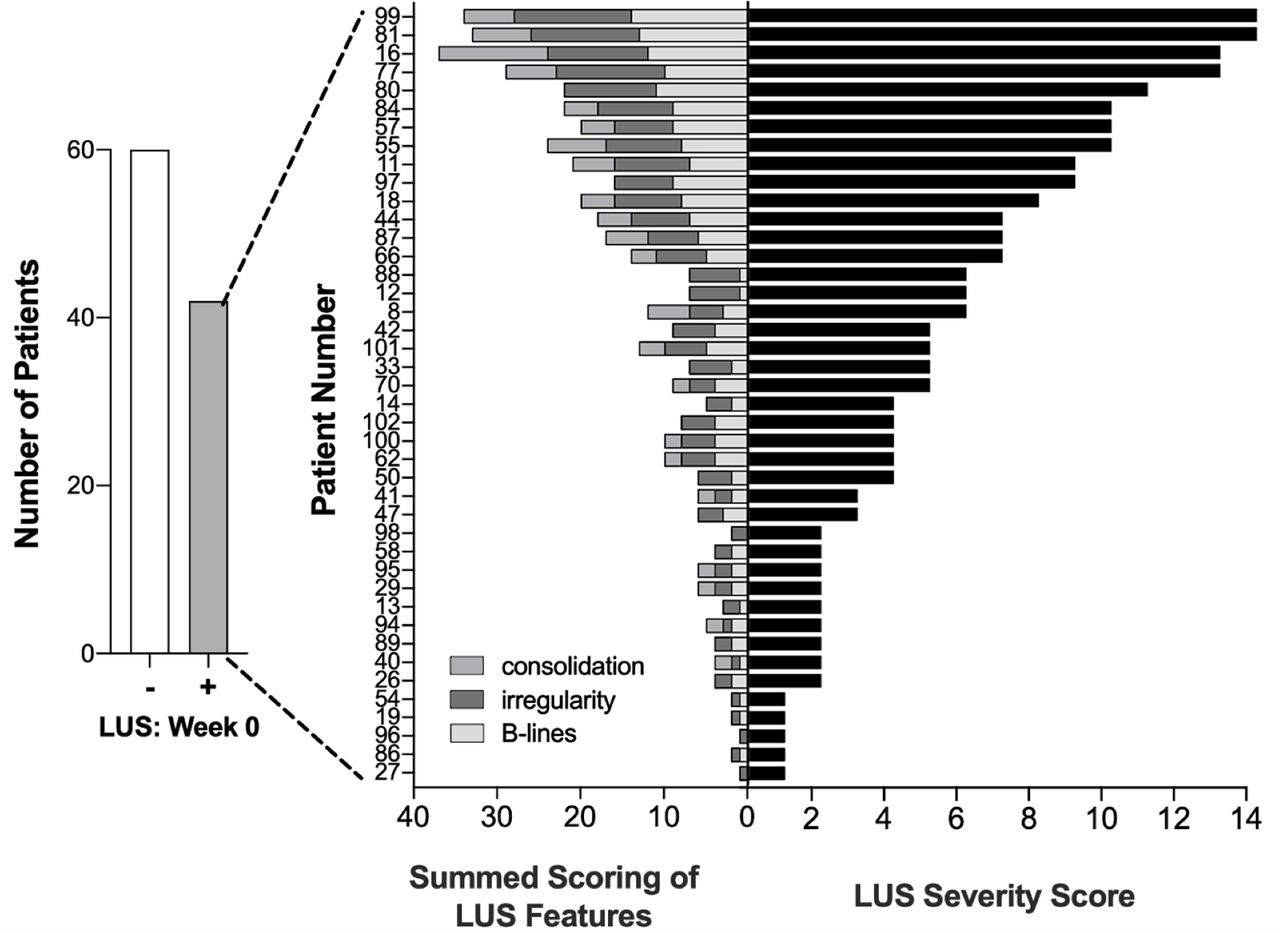
Baseline lung ultrasound results, features and severity for SARS-CoV-2 PCR positive patients.

(A) LUS of a healthy individual showing ribs (r) and pleural surface (p). (B) LUS (left panel) and CT imaging (right panel) of the left lung in a CV(+) outpatient at follow-up (patient 16) showing B-lines (arrows) and pleural irregularity (dotted circle) and location of LUS findings on corresponding CT imaging (black arrowhead) with corresponding reticulation and mild ground-glass reflecting mild fibrosis. This was ultimately felt to be due to pre-existing interstitial lung abnormality versus postpneumonia sequelae from SARS-CoV-2 infection (C) LUS (left and middle panels) and CT imaging (right panel) of the left lung in a CV(+) outpatient (patient 87) at baseline showing small subpleural consolidations (grey arrowheads) and corresponding peripheral ground-glass and consolidations typical for SARS-CoV-2 pneumonia on CT imaging (black arrowhead). CV(+), SARS-CoV-2 PCR positive; LUS, lung ultrasound.
Across the spectrum of CV(+)/LUS(+) patients at baseline, LUS findings were slightly more common in the paravertebral and subscapular regions compared with the posterolateral zones, with no clinically meaningful difference in findings between right and left lungs (online supplemental table 1). Among the 2844 individual scores for B-lines, pleural irregularity and consolidations across the six lung zones, only 47 scores were discordant between readers (kappa=0.966).
Supplemental material
Longitudinal LUS assessment
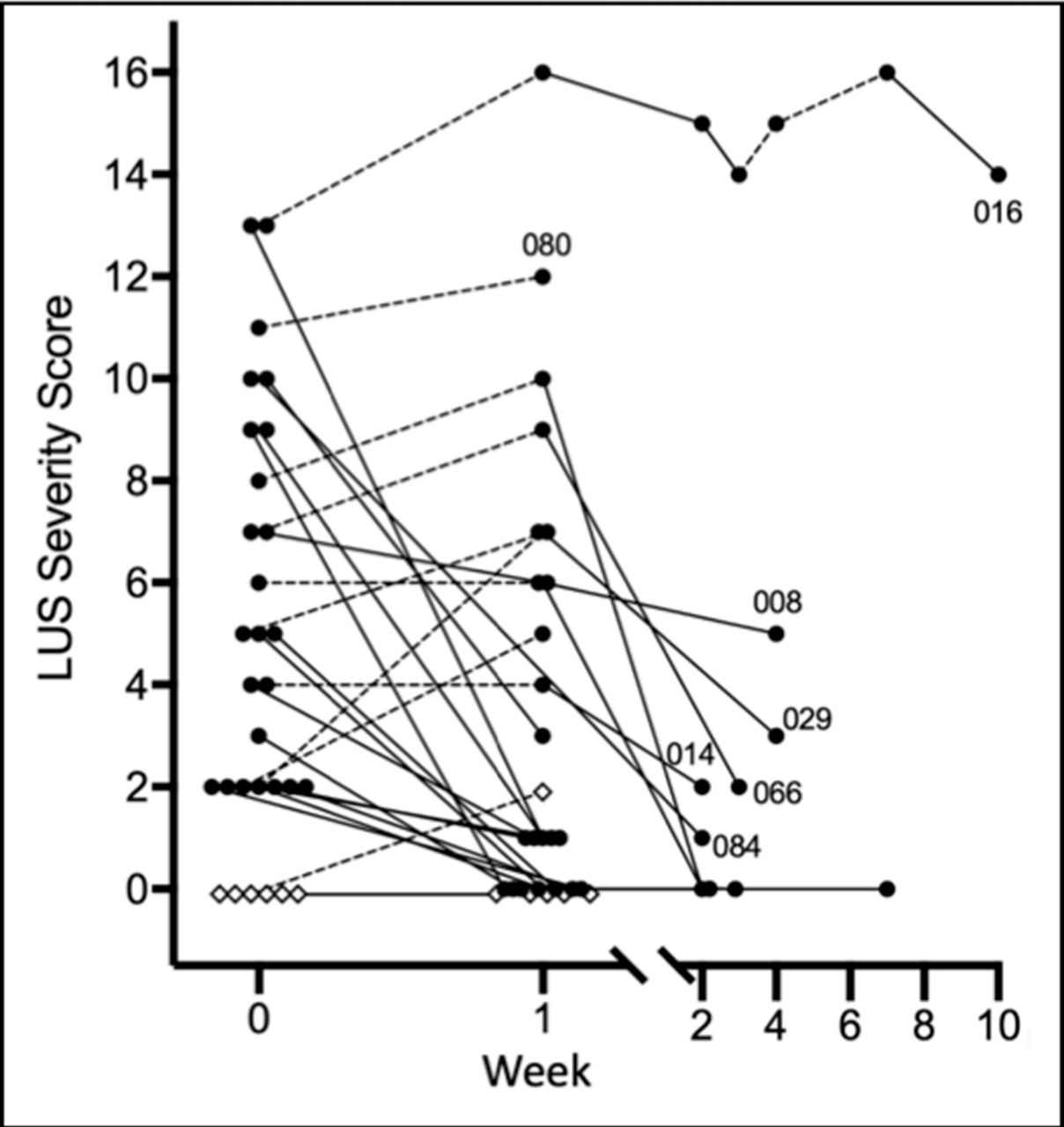
Twenty-four of the CV(+)/LUS(+) group and six of the CV(+)/LUS(−) group underwent follow-up LUS examinations (figure 3). At 1-week follow-up, 9 (37%) CV(+)/LUS(+) patients worsened (equal or higher severity score) and 15 (63%) subjects improved (lower severity score). Those who worsened were older, with a mean age of 54.9 compared with 41.3 in the group that improved (p=0.032) (online supplemental table 2). Patients who worsened were also more likely to report persistent symptoms of cough and/or SOB at 1-week follow-up (67% vs 27%, p=0.067). LUS findings improved in most patients by 1 or 2 weeks from their baseline LUS exam; however, several individuals had persistent LUS severity scores of >2 (figure 3). Follow-up LUS examinations for the six patients who were CV(+)/LUS(−) at baseline demonstrated negative LUS exams at 1 week for all but one individual who became LUS(+) with an overall severity score of 2. Of the 10 patients with follow-up LUS beyond week 1, four reported persistence of clinically relevant symptoms, three of which were LUS(−) at that time.
Supplemental material
{kind=link}
{kind=link}
{kind=link}
This figure includes only patients with follow-up LUS evaluations. Patient number is shown for select patients. Open diamond=baseline LUS severity score 0; closed circle=baseline LUS severity score >0; dotted line=increasing or same score at follow-up examination; solid line=improved score at follow-up examination. LUS, lung ultrasound.
Positive LUS risk factors
Comparing baseline CV(+)/LUS(+) and CV(+)/LUS(−) patients, LUS(+) patients had a higher mean age (47.4 years vs 41.0 years, p=0.038), were more likely to be female (67% female vs 33% male, p=0.022) and had a lower BMI (25.2 vs 27.8, p=0.009) (table 2). No significant differences were seen between CV(+)/LUS(+) and CV(+)/LUS(−) patients for baseline symptoms of cough, SOB or fevers. In a multivariate analysis, after adjusting for patient age, sex, African-American and Hispanic race/ethnicity, smoking status and BMI, the LUS severity score was significantly associated with SOB (p=0.041) but not fever or cough.
Baseline characteristics of patients with negative and positive lung ultrasound examinations
Clinical outcomes
Among CV(+) patients who responded to the 8-week survey (87%), only one individual was hospitalised overnight for fever and SOB, which occurred 2 days after baseline LUS examination (patient 62, LUS(+), severity score 6, figure 1). Through 8 weeks of follow-up, no patients required mechanical ventilation or died. Of the 13 patients in the CV(+) cohort who did not respond to the 8-week survey, 11 were LUS(−) at baseline, with the remaining two having low severity scores of 1 and 2. Nine of these non-respondents were reached by telephone after 8 weeks and declined to answer the survey at that time and subsequently failed to complete the 8-week survey online. Electronic health record review for these patients showed no hospitalisations or deaths.
In light of persistent LUS findings and CT findings, patient 16 (figures 1–3) was referred to pulmonology for evaluation. They had no history of diagnosed lung disease or chest CT prior to baseline LUS examination. They noted only mild fatigue and malaise initially, which resolved by week 4 onwards even though their LUS examinations were persistently abnormal. Pulmonary function testing was normal. A working diagnosis of ‘unclassifiable interstitial lung disease’ was given, with a differential that included pre-existing interstitial lung abnormality and possible postpneumonia sequelae from SARS-CoV-2 infection.24
Discussion
In this study, we found 41% of outpatients infected with SARS-CoV-2 had positive pulmonary findings by LUS. Our cohort was well balanced between men and women and racially and ethnically diverse. Patients presented with a broad range of symptoms, similar to that described in prior studies.25
Despite the high prevalence of positive LUS examinations, no patients in our study developed severe COVID-19 requiring mechanical ventilation or resulting in death through 8 weeks of follow-up. Only one patient required a brief overnight hospitalisation for SOB and fever. This suggests that the presence of pulmonary disease detectable by LUS at baseline is not a specific predictor of worse long-term clinical outcomes in this cohort of outpatients. This is in line with a study that looked at 30-day outcomes in 27 non-critical ER patients undergoing LUS, which did not find LUS to be prognostic of mortality or short-term complications but did predict likelihood of admission despite noncritical symptoms.26 Similarly, Colombi et al27 showed that while LUS sensitivity for COVID-19 pneumonia was similar to CT in emergency department patients, there was limited prognostic value. This is in contrast to studies that have shown LUS to be useful in hospitalised patients in predicting ICU admission, ventilation and mortality.28–30
Compared with CV(+)/LUS(−) patients, CV(+)/LUS(+) patients were older, more likely to be female, with a lower BMI. Given that the opposite (ie, male sex and increased BMI) are associated with more severe COVID-19, this further supports the notion that positive LUS findings early in the course of the disease likely do not portend worse outcomes. We did find increased and persistent pulmonary involvement with age, which parallels reports of more severe pulmonary disease in older patients with COVID-19.31–33
Although having a positive LUS was not a useful prognosticator, it did appear clinically meaningful. A higher LUS severity score was significantly associated with baseline SOB, after adjusting for patient age, sex, African-American and Hispanic race/ethnicity, smoking status and BMI. This suggests that disease detectable by LUS translates into relevant clinical symptoms.
Through longitudinal assessment of 24 CV(+)/LUS(+) patients, we demonstrated that the majority of patients had improvement in their LUS severity score at 1-week follow-up. Furthermore, nine patients had worsening LUS severity scores at follow-up, and yet still had favourable clinical outcomes, without developing severe illness. Notably, the patients with worse LUS scores at 1-week follow-up were significantly older than those who improved and had increased persistence of symptoms of cough and SOB. For longitudinal follow-up beyond 1 week, there was no relationship between persistent or resolved LUS findings and symptoms, providing no support for persistent LUS findings as a predictor of chronic COVID-19. An important unanswered question that remains is whether persistent LUS findings may ultimately predict long-term parenchymal lung disease.
This study has several limitations. First, patients with increased BMI were less likely to have a positive LUS, and this may reflect a decreased sensitivity of LUS technique due to reduced tissue penetration. Second, a subset of potential outpatient enrollees declined participation specifically because they felt too ill to participate (14 of 311 contacted patients, 5%), resulting in a potential selection bias. We imagine that including these patients would likely result in the prevalence of lung disease detected by LUS being higher than what we report here. Third, we were unable to determine the exact date of infection and its relationship to our baseline LUS examinations. The heterogeneity in the time between infection and LUS examination could theoretically lead to LUS findings resolving by the time of baseline examination, or LUS findings developing after baseline examination. We attempted to keep the time between SARS-CoV-2 testing and baseline LUS as short as possible but were limited by result turnaround time, time to patient being informed, and screening and scheduling factors. Taking into account our longitudinal LUS results, only one LUS(−) patient at baseline went on to develop LUS findings at week 1. Conversely, numerous LUS(+) patients had persistent findings at longitudinal follow-up. This suggests that the impact of variability in time between infection and baseline LUS examination is likely to be small. Fourth, we chose to perform only posterior LUS evaluations to minimise infection risks associated with the study. Dedicated studies assessing the sensitivity of posterior assessment compared with posterior and anterior assessment are not available; however, COVID-19 lung involvement is commonly found in the posterior and lateral aspects of the lungs.8 9 Lastly, patients did not undergo CT imaging for confirmation of LUS findings as part of the study, although two patients did have CT scans for clinical evaluation and those studies were concordant with their LUS. As recent studies have confirmed high sensitivity of LUS for COVID-19 pneumonia, this limitation unlikely has significant impact on disease prevalence, although we acknowledge that severity score concordance between CT and LUS vary.8
This study also has several strengths. This was the first study to investigate the prevalence of pulmonary findings in outpatients with SARS-CoV-2 infection using LUS, and the largest outpatient COVID-19 study of the general population to date. Our cohort was diverse and representative of the geographic region. While several LUS scoring systems have been outlined for COVID-19, none have been robustly validated. We developed a scoring system combining component severity and distribution throughout the lung zones, which resulted in a wide range of scores and excellent inter-rater reliability. In addition, we included 14 control CV(−) subjects, which were all read as LUS(−). Finally, we were able to provide longitudinal data on a subset of patients and describe the natural evolution of COVID-19 by LUS.
Conclusion
Our cohort of 102 CV(+) outpatients showed a prevalence of 41% for positive LUS without any adverse clinical outcomes occurring through 8 weeks of follow-up. While prior studies have shown utility in the acute care setting for predicting hospital course, our results suggest LUS screening in the general outpatient CV(+) population may provide little benefit for prognostication and surveillance.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Data relevant to the study are included in the article and supplementary information. Additional deidentified participant data is available on reasonable request to the corresponding author, Robert Fairchild (rfairchi@stanford.edu).
Ethics statements
Ethics approval
This study was approved by the Stanford University Institutional Review Board (#IRB- 56807).
Acknowledgments
We would like to thank John and Jacque Jarve for their generous support. We also thank Dr Linda Barman and her team at the Stanford CROWN clinic for their assistance on this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RMF and AH contributed equally.
Contributors Study conception and design: RMF, AH, DAM and MCB; data collection: RMF, AH, DAM and GRT; data scoring: RMF and AH; data analysis and interpretation: RL, DL, HHG, RMF, AH, DAM, GRT and MCB; first draft of manuscript: RMF, AH and DAM; all authors critically reviewed and approved the final version of the manuscript.
Funding MCB received support for this work from the NIH R25 AI 147369.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.