Article Text

Abstract
There is a rising burden of chronic obstructive pulmonary disease (COPD) in India. Pulmonary rehabilitation (PR), is a universally recommended multidisciplinary therapeutic strategy for the management of COPD; however, its needs are unmet. The diversity in the healthcare systems, availability of PR specialists and sociocultural multiformity requires contextualised and innovative PR models. Culturally sensitive elements, such as yoga, have some evidence of a positive impact in the management of COPD. Yoga and PR are based on similar principles with a holistic approach of involving physical activities, behaviour change techniques and psychological support to improve disease outcomes. Arguably the principles of PR and yoga are complementary but there are some important differences in the intensities of activities, exercise types and inclusion of mindfulness in components that must be considered. Components of PR enable aerobic capacity building, strengthening of muscles of the upper and lower extremities and building awareness towards disease management. Yoga, on the other hand, primarily can focus on core strengthening, breathing control, mindfulness and self-awareness. We discuss the potential of integrating the sociocultural appeal of yoga with PR delivered at international standards, and how an integrated approach may lead to optimal referral, uptake and completion.
- exercise
- complementary medicine
- pulmonary rehabilitation
- COPD pathology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction to pulmonary rehabilitation and yoga
Pulmonary rehabilitation (PR) is a multidisciplinary therapeutic strategy with clearly defined objectives, structure and assessment measures, that is internationally recommended for people living with chronic respiratory diseases.1–3 Considering the huge burden across the globe and progressive nature of chronic obstructive pulmonary disease (COPD), access and availability of PR services are essential but in reality the needs remain unmet.4–6 Given the global diversity in healthcare systems, availability of services and trained PR personnel, patient demographics and sociocultural multiformity, PR models require relevant adaptations to improve its uptake and delivery.7 8 These issues have caught attention of the PR stakeholders who are in strong agreement on the need to develop novel PR models that are not only locally relevant but also efficacious and effective.6 8–12 Keeping the sanctity of evidence-based PR intact, contextualised models integrated with more culturally relevant elements like regional dance forms or meditation and exercise techniques like yoga, Qui Gong or Tai Chi are worth exploring.11 13–15 There is some evidence of the positive impact of yoga in the management of COPD.16–18 Yoga and PR are from different therapeutic approaches but are complementary to each other and may have an additive effect with the inclusion of the appropriate yoga components to PR.
Yoga is an ancient prevedic science and an integral part of the Indian culture, practiced even today by many. Although yoga originated in India, it has received advocacy from global platforms like the United Nations observing International day for yoga.19 Yoga in its true sense means union of body and mind, a communion with the universe signifying its expanse beyond just physical health. Yoga philosophy considers physical, physiological, mental and spiritual well-being for optimal functioning of the body and mind. Yoga is based on eight limbs or dimensions called the Ashtanga yoga (Ashta—eight; Anga—dimensions) as described in table 1.20 21 Yoga is traditionally known as a psychosomatic practice for general well-being. The therapeutic potential of yoga is being studied in management of several diseases for the last five decades, with evidence of its health promoting benefits.22 23 However, the challenge with these studies is understanding precisely the components of yoga that are tested as part of scientific trials. It can be argued that yoga is itself a complex intervention, and to replicate the interventions effectively the details of the intervention should be described in a standardised format.
Ashtang yoga: eight dimensions or limbs of yoga practice
Emerging evidence on yoga for COPD
Yoga has been shown to have a range of health benefits for people living with COPD. A systematic review that included 10 randomised and non-randomised controlled trails, suggested improvements in 6-min walk distance (mean difference (MD): 22 m; 95% CI 10 to 34) which falls just below the minimum clinically important difference of 30 m post-PR and St George Respiratory Questionnaire (n=105) (MD: −3.81 points; 95% CI −6.65 to −0.97 points) among yoga group in comparison to groups with no rehabilitation-based interventions.24–27 Improvements in FEV1, FEV1 % predicted, PaCO2 have also been noted with yoga interventions.24 28 Another systematic review with 16 studies exploring yoga, Tai Chi and Qui gong when compared with control group, showed benefits in dyspnoea, lung functions, exercise capacity and quality of life.18 There are some weak links with yoga to reduction in airway inflammation as suggested by changes in FeNo and TNFα.29 A meta-analysis with eleven studies focusing on the risks and benefits of yoga interventions for COPD did not report safety issues distinctively in this population, however the variability in the interventions, and outcome reported, clearly indicates the need for clear reporting, standardisation of protocols and use of appropriate outcome measures to understand the mechanisms of action that are still unclear.28 30 This challenge extends across experimental designs.
The objectives and outcome measures of yoga therapy in COPD studies were similar to the core structure and assessment measures of conventional PR programmes. Yoga is clearly a multifaceted, complex intervention and the components are not well defined, for example, few studies tested yoga postures (Asana),31 32 some involved only breathing techniques (Pranayama),33–36 while other studies added more components such as education sessions, relaxation techniques and meditation (Dhyana).29 30 37–45 Furthermore the intervention ranged from 4 to 12 weeks, once or twice a week and varying 30–90 min each session alongside home exercise regimes. All of this variability (outcomes, components and delivery) strongly highlights the need for clear reporting, and standardisation of protocols.
Integrating yoga with PR
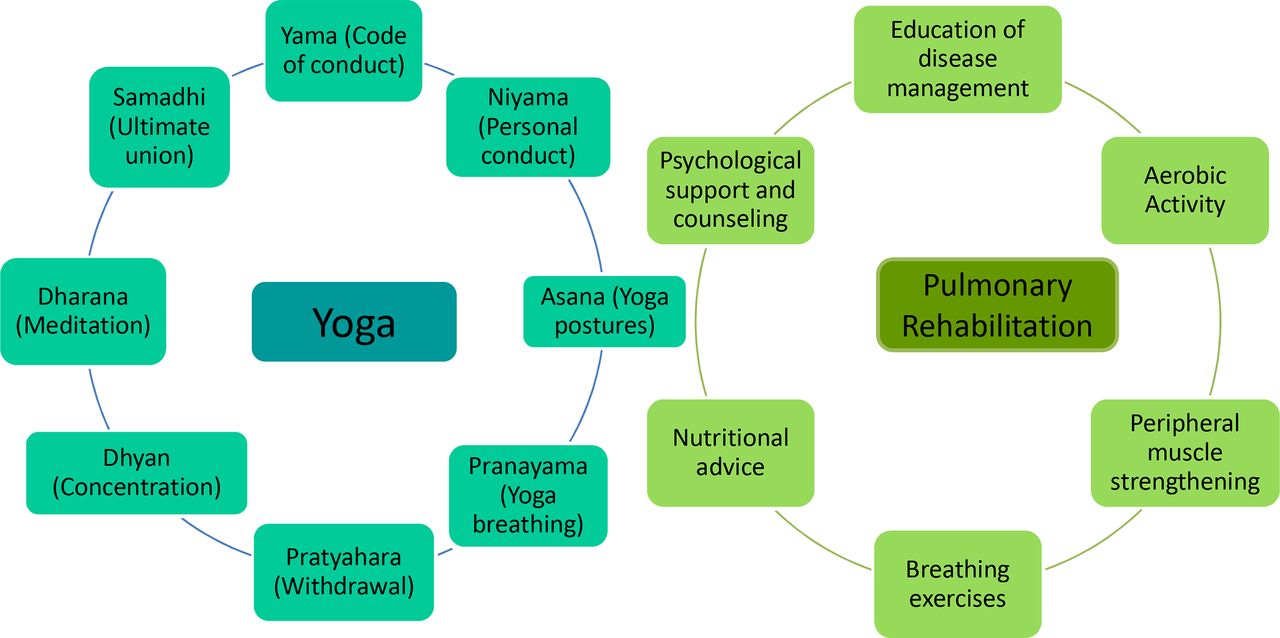
Yoga and PR are based on similar principles that are complementary to each other and can facilitate integration (figure 1). Both these systems of care are multi-dimensional involving physical activities, behaviour change techniques and psychological support to improve disease outcomes. However, there are some important differences that may optimise the appeal and effectiveness of PR with integration of yoga.

Components of yoga and Pulmonary rehabilitation.
Although physical exercises are common to PR and yoga, there are significant differences in their form or type. The main component of physical exercises in PR are the aerobic activities that utilise bigger muscle groups in a repetitive manner, such as walking or cycling, to build cardio-respiratory fitness. This form is not conventionally included in yoga where the focus is on stationary postures. These are lower in intensity than aerobic or resistive exercises.11 46 47 Given this emphasis on low intensity exercise and its form, integrating yoga into PR could address the following challenges:
The combination of low and high intensity activities may provide an opportunity to better tailor the programme to the ‘good and bad days’ typically reported by patients.
Facilitate gradual progressions in exercise prescription as part of PR, from lower intensity exercise to medium and high exercise intensities and add variety to the types of exercises in people may engage with.
Yoga requires less space and equipment in comparison to walking or cycling; and can also be performed indoors making it favourable to maintain participation even with extreme weather changes.
Practice of yoga postures is very methodical and involves the following three phases: (1) attaining the pose; (2) holding and (3) releasing the pose.48 The holding of the pose constitutes for an Asana which literally translates to being at ease or to be stable.48 Holding of the pose causes isometric, isotonic contractions and static stretching of the muscles resultantly improving strength and flexibility.49 Resistance training in PR incorporates open kinetic chain movements with properties like hand-held weights. Whereas in yoga, certain poses like the Cobra pose (Torso extension in prone lying) involve close kinetic chain movements that engage more muscle groups at a time and utilise body weight as resistance for strengthening of upper girdle musculature while stretching some portions of the torso which may help in improving breathing patterns among patients wth COPD. Poses like the Tree-pose (single-leg stance) also help with improvement in proprioception and balance,48–50 which can be crucial for maintaining the functional status of the elderly population living with COPD which may be valuable on being added to PR as a component.
Incorporating yoga poses along with other forms of exercises in PR may help improve flexibility, strength, stability and functional movement patterns.
Yoga poses are least dependent on props for exercising which may make it more convenient for participants to practice.
Yoga is a psychosomatic practice, and its effects are beyond physical attributes. While performing the posture, the focus is on being aware of the movement, the stability, synchronised breathing, which is the basis of mindfulness in yoga. According to the earliest Yoga scripture, Yoga Sutras of Patanjali, yoga postures were described as positions for meditation signifying further the emphasis on mindfulness. Yoga breathing techniques (Pranayama; where Prana means life, synonymously used with breath whereas Ayama means control) also incorporate mindfulness. The breathing techniques range from slow relaxed breathing to more intense exhalations. The awareness of every breath instils a perception of control over breathing which is vital for adults living with COPD who encounter breathlessness leading to functional disability and anxiety.8 Bumblebee breathing (Bhramari) creates a humming sound during exhalation and instils calmness helping with stress regulation and emotional control.39 Kaminsky et al33 demonstrated that practice of Dirgha breathing (three part breathing with extended exhalation) alone can reduce gas trapping and improve resting hyperinflation resulting in improved exercise capacity among patients with COPD. Similar to breathing exercises in PR, yoga deep breathing techniques with chest wall expansions improve thoraco-abdominal movement.51
Another important aspect in PR is supporting people with common mood disorders like depression and anxiety. Yoga interventions have shown improvements in anxiety and depression among patients with COPD.30 However, yoga considers mental well-being imperative irrespective of any underlying mood or mental disorder. Apart from the physical activities that contribute to mindfulness, Yoga involves meditation and relaxation techniques. Each yoga session completes with meditation followed by prayers or affirmations for positive thinking for enhanced self-worth and stress regulation.52 The physiological changes attributable to meditation can be summarised as modulation of autonomic nervous tone and consequent reduction in sympathetic tone, activation of antagonistic neuromuscular systems, which may increase the relaxation response in the neuromuscular system, and stimulation of the limbic system primarily by meditation.53 The key contribution from yoga as a psychosomatic practice is its ability for emotion regulation through physical activity, breathing and meditation, when practiced alongside PR can enhance the health-related quality of life of adults living with COPD. Yoga breathing techniques (Pranayama) can help instil a sense of control over breathing, potentially reducing dyspnoea and improve pulmonary functions.
All the components in yoga are based on mindfulness which may add value for all participants irrespective of any co-morbid mood disorders.
Inclusion of varied breathing techniques in the integrated PR programme can have an overarching benefit on dyspnoea, exercise capacity and emotional control for patients with COPD.33 36 42 45 54
The educational component is an important element in the foundation of PR programme to improve awareness, knowledge and enable patients to manage their disease better. Education sessions as suggested in PR guidelines,1 2 include information about the disease, its management strategies, ergonomic advice, appropriate nutrition, airway clearance techniques and maintenance. The education sessions conducted during yoga intervention for COPD are not as well-reported and do not necessarily follow the structure and content of the PR education component.55
In the integrated PR model, including the sessions on yoga philosophy and importance of each yoga component in addition to the PR education sessions may help patients get a better understanding of the protocol.
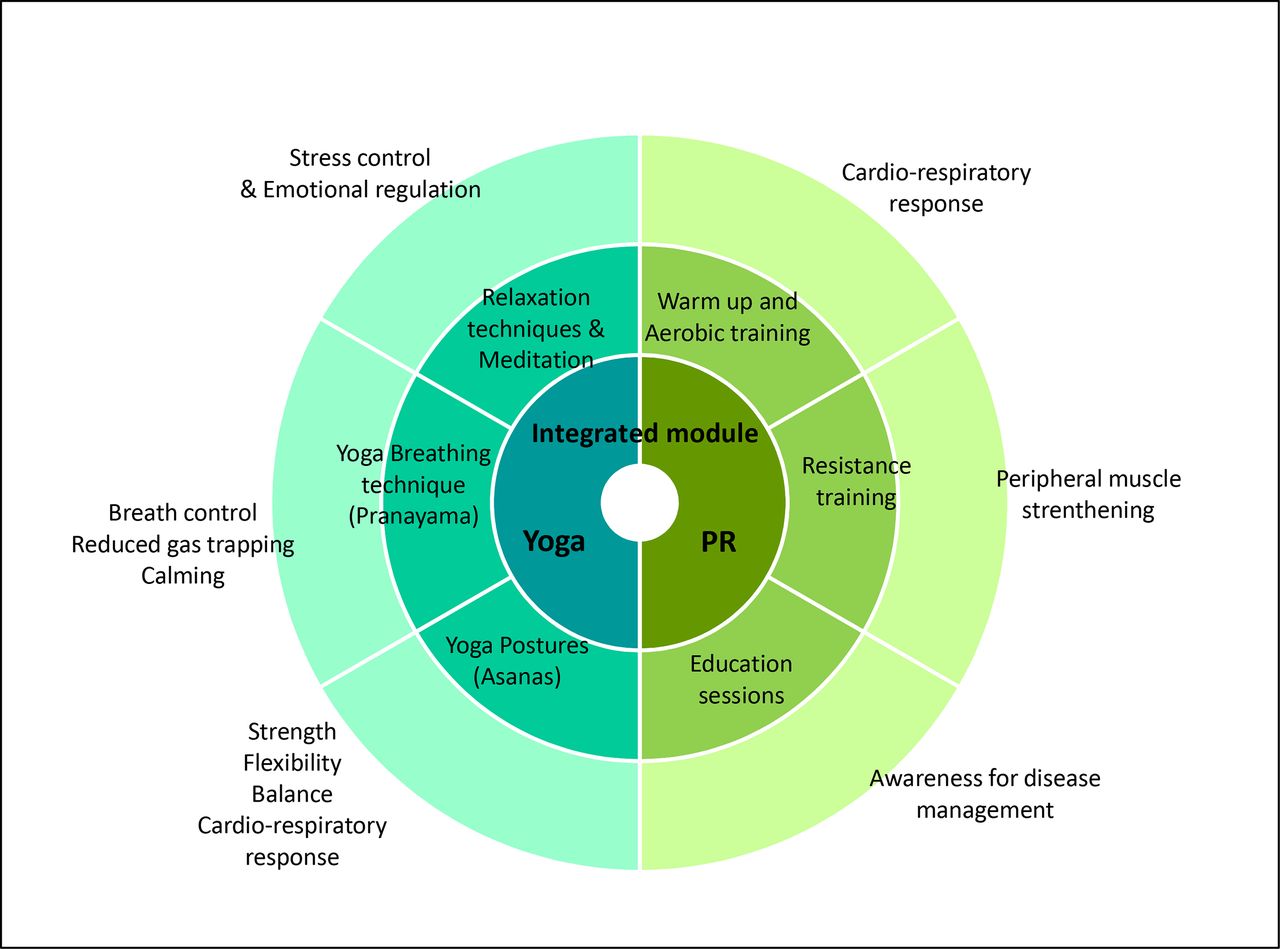
It is important to identify the contributions from yoga and conventional PR as appropriate so as to integrate them with minimum overlapping and maximise synergy (figure 2). Components of PR enable aerobic capacity building, strengthening of muscles of the upper and lower extremities, and building the knowledge and awareness to empower patients to manage their health condition. Yoga, on the other hand, primarily can focus on core strengthening, breathing control, mindfulness and self-awareness. However, the biggest value addition from an integrated PR–yoga programme comes from the socio-cultural appeal of yoga alongside the efficacy of conventional PR. Effectiveness of a long-term non-pharmacological, behaviour change intervention like PR is determined by the adherence of participants. A three-arm randomised controlled trial over a period of 6 months among apparently healthy elderly participants suggested that the adherence rate among the participants in the yoga arm was better than the exercise group and waitlist control group.56 Patients may have a better connect culturally with the integrated model that may help improve programme adherence and disease outcomes.

{kind=link}
{kind=link}
Conceptual framework of PR–yoga integrated module.
Framework for reporting an integrated PR–yoga programme
The descriptions of the intervention programmes are crucial for reproducibility, understanding of efficacy and effectiveness of the interventions and its applicability in the clinical settings.57 We propose a framework to report the yoga component of the integrated programme alongside the conventional PR components (table 2).
Reporting framework of the yoga component of the integrated yoga-PR programme
1. Yoga intervention: Physical activities in PR follow the standard reporting format based on Frequency, Intensity, Type and Time principle. Alongside PR components, yoga poses, breathing techniques and meditation techniques need to be illustrated in terms of number of repetitions and duration of hold wherever applicable. It is necessary to specify the style of yoga used, as the intensities and methods of performance vary significantly and resultantly can impact the outcomes. Also, yoga practice follows a certain sequence beginning from the physical activities followed by breathing control followed by session completion with mental and spiritual components of education, meditation and relaxation techniques. This sequence needs to be captured so as to follow standardisation and observe the effects.
2. Programme delivery: Yoga and PR are complex techniques that require knowledge and experience in conducting sessions for patients. Trained personnel ensure safety of participants, efficacy and effectiveness of the intervention.57 It is thus crucial to report the details of the programme personnel. Reporting of programme location or settings, and whether it is a cohort or rolling programme gives an important perspective on the logistics and operations necessary of programme delivery. Also, apart from the recommended clinical outcome measures, it is important to report the adherence levels, dropouts, and acceptability of the PR–yoga integrated programme. The safety measures to identify and overcome adverse events like exacerbations, injuries or falls should be documented.2 17 58 Patient testimonials, paper diaries can be used to track the reverberations of the intervention. Non-clinical outcome measures may provide valuable inputs to improve, tailor and reproduce the integrated PR–yoga programme.
Challenges of integrated yoga–PR programme
Yoga originated from the Indian subcontinent with its philosophy, components and practices closely associating with the Indian culture. This may make it seem complicated and less feasible for participants from other parts of the world. However, the literature shows that yoga protocols for COPD have been studied successfully in different countries including India, Australia, United States, and Oman, and among varied populations. Also, additional supporting media like pamphlets or videos in regional languages on how to perform the yoga postures or breathing techniques may be helpful in reinforcing the correct ways of practicing the techniques. Furthermore, to integrate yoga with PR, expert consultation and patient feedback can help overcome feasibility concerns. Another challenge that may be faced in western populations is to find sufficient expertise in yoga. However, there is evidence that PR delivery team including physiotherapists can be trained by expert yoga trainers to deliver yoga-based PR programme effectively.37 Managing the session duration of integrated PR and yoga classes must be considered. While yoga may make PR more appealing, the possible longer sessions and intervention durations may risk patient dropouts. It is thus important to make these sessions more engaging by incorporating innovative ways like more group activities, dissemination of clear objectives of each session so the patients know what to look forward to, planning and monitoring home activities, handing out reading material and exercise steps for home practice. To optimise the session duration, different combinations of components can be suggested to the patients. For instance, if the patients are recommended resistance training for 3 days a week, the rest of the 3–4 days can be allocated for yoga postures and breathing techniques, meditation and walking can be 5–6 days a week. Further studies will be needed to understand what combinations are most effective and can be delivered in optimised durations.
Conclusion
With the unmet need of PR globally, novel culturally appropriate PR models are the need of the hour to improve acceptability, feasibility and adherence. Culturally acceptable adaptations can provide better opportunity for patients to internalise and adhere to the PR programmes. Yoga has therapeutic effects on various pathological conditions and there is a strong evidence of effectiveness of yoga in management of COPD. Yoga is a holistic approach with aims, components and outcome measures complementary to those of PR. With all the overarching benefits and the sociocultural appeal of yoga in many parts of the world, when combined with the efficacy of PR delivered to international standards, an integrated PR with yoga intervention may lead to optimal referral, uptake and completion rates. This innovative approach should be tested where yoga resonates with people.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @shrutids31
Contributors SSah and SSal constructed the concept. SSi planned, reviewed literature, constructed primary drafts and revised the drafts of the article. SSah also supported with supervision, reviewing and editing the article. SSah, MO along with AJ supervised, edited and reviewed all manuscript drafts. GT reviewed the concept and helped with editing the drafts of the manuscript.
Funding This research was funded by the National Institute for Health Research (NIHR) (17/63/20) using UK aid from the UK Government to support global health research.
Disclaimer The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.