Article Text

Abstract
Introduction Massive haemoptysis is a life-threatening event in advanced cystic fibrosis (CF) lung disease with bronchial artery embolisation (BAE) as standard of care treatment. The aim of our study was to scrutinise short-term and long-term outcomes of patients with CF and haemoptysis after BAE using coils.
Methods We carried out a retrospective cohort study of 34 adult patients treated for massive haemoptysis with super selective bronchial artery coil embolisation (ssBACE) between January 2008 and February 2015. Embolisation protocol was restricted to the culprit vessel(s) and three lobes maximum. Demographic data, functional end-expiratory volume in 1 s in % predicted (FEV1% pred.) and body mass index before and after ssBACE, sputum colonisation, procedural data, time to transplant and time to death were documented.
Results Patients treated with ssBACE showed significant improvement of FEV1% pred. after embolisation (p=0.004) with 72.8% alive 5 years post-ssBACE. Mean age of the patients was 29.9 years (±7.7). Mean FEV1% pred. was 45.7% (±20.1). Median survival to follow-up was 75 months (0–125). Severe complication rate was 0%, recanalisation rate 8.8% and 5-year-reintervention rate 58.8%. Chronic infection with Pseudomonas aeruginosa was found in 79.4%, Staphylococcus areus in 50% and Aspergillus fumigatus in 47.1%.
Discussion ssBACE is a safe and effective treatment for massive haemoptysis in patients with CF with good results for controlling haemostasis and excellent short-term and long-term survival, especially in severely affected patients with FEV<40% pred. We think the data of our study support the use of coils and a protocol of careful and prudent embolisation.
- cystic fibrosis
- massive haemoptysis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Key question of this study is short-term and long-term outcome of patients with cystic fibrosis (CF) and massive haemoptysis using coils for bronchial artery embolisation.
Super selective bronchial artery coil embolisation is safe, has good short-term and long-term outcomes, and significantly improves FEV1% predicted.
Data of this study merit rethinking of overall aim and treatment of massive haemoptysis in patients with CF, especially as life expectancy but also concomitant complications like haemoptysis are rising.
Introduction
Survival of patients with cystic fibrosis (CF) has risen from merely a few months in the 1950s1 to a median age of survival of more than 40 years in developed countries today.2 Patients born in the 21st century have an estimated life expectancy of over 50 years. As the number of adult patients with CF is estimated to increase by 72%–78% until 2025 in high-income countries, concomitant rise of complications associated with advanced lung disease is likely.3 Functional end-expiratory volume in 1 s in % predicted (FEV1% pred.) serves as the main outcome parameter to monitor CF.
Massive life-threatening haemoptysis occurs frequently in older patients and in severe disease with an average annual incidence of 0.87%. Of all patients with CF, 1%–4.1% experience at least one episode of massive haemoptysis during their lifetime.4 5 The process of chronic neutrophilic inflammation in CF lung disease is understood to cause bronchial and non-bronchial systemic arteries (NBSAs) to undergo major hypertrophy over time.5 6 Prevailing theories for the development of haemoptysis suggest combined inflammatory and mechanical stress weakening the walls of hypertrophied and friable submucosal bronchial arteries, which then erode and bleed into airways.5 If left untreated, mortality rates for massive haemoptysis in CF are as high as 75%.7 Mortality is not attributed to massive blood loss but rather to asphyxia through alveolar tamponade.
Beyond the acute life-threatening event, haemoptysis in patients with CF has been associated with faster decline in lung function, accelerated need for lung transplant and increased mortality.5 8–10
The relative risk of dying for patients with massive haemoptysis and FEV1 >50% pred. was 7.4 compared with those with similar pulmonary impairment but without massive haemoptysis.5 Today, endovascular embolisation of hypertrophied bronchial arteries (bronchial artery embolisation (BAE)) is standard of care treatment in life-threatening haemoptysis according to the CF Foundation guidelines.6 11–17 In most studies, absorbable and non-absorbable embolisation materials such as gelfoam particles, polyvinyl alcohol (PVA) or N-butyl-2-cyanoacrylate had been used,6 8 12–20 but there are little data concerning coil embolisation.21
Although BAE can be life-saving, patients with CF who have undergone BAE with microsphere particles (m-BAE) for haemoptysis are at much higher risk of respiratory function aggravation, death and need for lung transplant. They are more likely to die or to undergo lung transplant than to present with recurrent major haemoptysis.22 Patients with CF who underwent BAE with blood-dependent materials had a higher mortality than matched controls without haemoptysis and without BAE.23
We report on patients with CF with massive haemoptysis treated with super selective bronchial artery coil embolisation (ssBACE) of hypertrophied bronchial arteries. The aim of our study was to scrutinise long-term clinical outcome in patients with CF embolised with metallic coils alone.
Methods
Patients
We performed a retrospective cohort study with chart review and pseudonymous analysis of a total of 34 consecutive patients with CF lung disease and massive haemoptysis who received at least one ssBACE in our institution between January 2008 and February 2015. All patients were referred to our hospital with severe life-threatening and/or repetitive haemoptysis in which conservative treatment had failed. Massive haemoptysis was defined as >240 mL in 24 hours or recurrent bleeding of substantial volume (>100 mL/day) for a few days or weeks.13 24 Indication for ssBACE was defined following the criteria set by the Cystic Fibrosis Consensus Committee on Pulmonary Complications of Cystic Fibrosis: (1) major haemoptysis as previously defined, (2) mild or chronic haemoptysis that interferes with lifestyle and (3) haemoptysis that interferes significantly with airway clearance manoeuvres.13 Demographic data, FEV1% pred. and body mass index (BMI) before and after ssBACE, sputum colonisation, procedural data, time to transplant and time to death were documented.
Patients or public were not involved in the design, conduct, reporting or dissemination plans of our research.
Embolisation
After two cases of lobar necrosis and lobectomy after use of microparticles in the 1990s, our centre returned to the use of coils in BAE. This enabled us to achieve haemostasis yet ensuring preservation of vital lung tissue.
All ssBACEs were carried out in the same institution by the same interventionalist (MJM) with a 20-year experience and 633 bronchial artery coil embolisations. ssBACE was performed with local anaesthesia at the puncture site in all but two patients who arrived intubated and ventilated at our institution. Localisation of bleeding site was mainly based on patient perception and on angiography findings of hypertrophied bronchial arteries and NBSA as the active bleeding site could not be detected. Successfully obtained haemostasis confirmed embolisation of the correct thus culprit vessel. Thirty-three patients arrived with external CT scan 0–16 months prior to intervention; 24 of these scans were contrast enhanced. If possible, CT scans were used to identify hypertrophied bronchial arteries and, if recent enough, bleeding site.
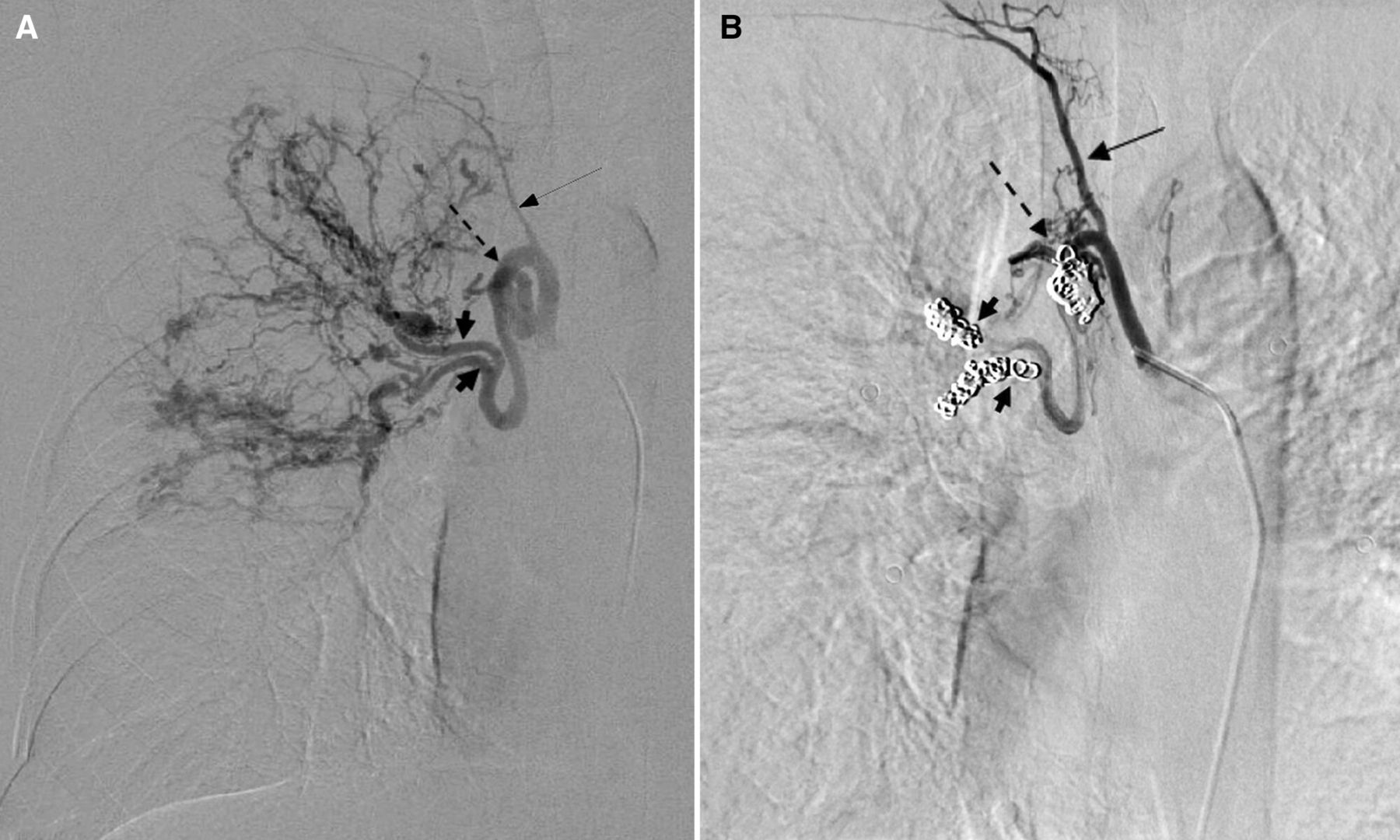
All interventions were carried out as ssBACE with platinum coils. Aortography was performed using Cobra or Headhunter catheters via a femoral access and 4-French catheters with coaxial microcatheters for selective bronchial arteriography. Bronchial arteries >2 mm in diameter were defined as hypertrophied.25 26 ssBACE of target vessels was carried out with pushable coils using target fibred coils (2/10–4/40 mm) or Guglielmi detachable coils (3/6–3/30 mm). Coils were placed as distally as possible and in addition in a central position (shown in figure 1). When all abnormal bronchial arteries supplying the region of interest were embolised, the procedure was terminated. Hypertrophied bronchial arteries and NBSA which did not lead to the culprit segment were not occluded. A maximum of three lobes was treated per intervention. Procedural data were documented. Complications of intervention were defined according to the Society of Interventional Radiology.27 Transient intraprocedural minor thoracic pain not necessitating treatment and transient mild coughing during intervention were not counted as complications. Pseudoaneurysm but not haematoma at the puncture site were included as complications. Recanalisation rate was based on angiography findings at the time of reintervention in the same lobe.
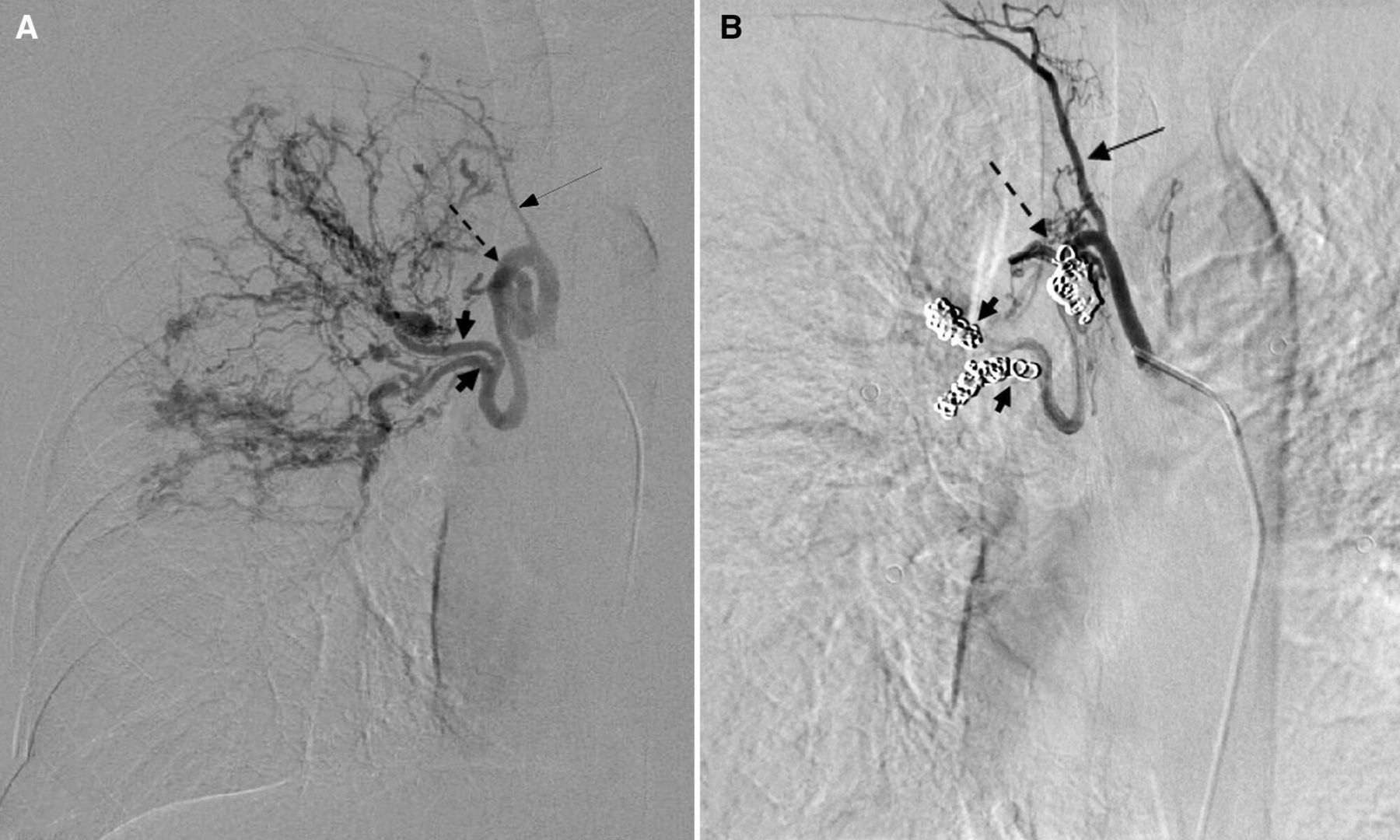
(A) Angiography of hypertrophied bronchial arteries. Fat arrows and perforated arrows in image (A) represent the position of coil material placed in image (B). The slim arrow shows a bronchial artery without hypertrophy supplying the same lobe in (A). Coils were placed in a peripheral (fat arrows) and in a central position (perforated arrow). (B) Control angiography 4 years after embolisation. The embolised arteries remain occluded. Hypertrophy of a formerly minor vessel (slim arrow) has occurred.
Statistics
All data were tested for normal distribution by Kolmogorov-Smirnov test. Normally distributed data were presented as mean±SD, and difference was calculated by applying the paired t-test. Not normally distributed data are presented as median (minimum–maximum), and difference was calculated using the Wilcoxon ranked test. A p value of <0.05 was considered statistically significant. Software programme IBM SPSS Statistics V.26 was used.
Results
Patients
A total of 36 patients underwent at least one ssBACE between January 2008 and February 2015. Two patients were excluded, one as the causative artery could not be detected and the other as the patient was lost to follow-up directly after the embolisation. All 34 included patients had a history of massive haemoptysis and/or severe recurrent haemoptysis. All but two patients arrived at our hospital in stable condition, and embolisation could be carried out with patients fully awake. Patient data were extracted from patient charts in 10 different hospitals Germany-wide. In two patients who had received earlier bronchial artery interventions outside our hospital, data referred to the first intervention in our institution.
Observation interval after first coil embolisation for all patients alive in May 2020 was 66 months minimum with a median interval of 89.9 months (66–125) and 20 of 32 patients alive in May 2020. Twelve patients died during the study period; of these, 6 died during the 5-year-observation interval 0, 2, 10, 11, 32 and 45 months after ssBACE. Five patients died of respiratory failure; three died after lung transplant; one died with uncontrollable massive haemoptysis; and three patients died of other causes.
Pulmonary impairment according to FEV1% pred. before intervention was mild in 2 patients, moderate in 19 and severe in 13. During 2-year observation interval, two patients underwent lung transplant and four patients died. One patient died 2 weeks after embolisation with uncontrollable haemoptysis. Two patients were lost to follow-up 34 and 70 months after intervention, respectively. Therefore, 33 patients were included in FEV1% pred. and BMI estimates; 34 were included in 1-year survival analyses; and 33 patients were included in 5-year survival analyses.
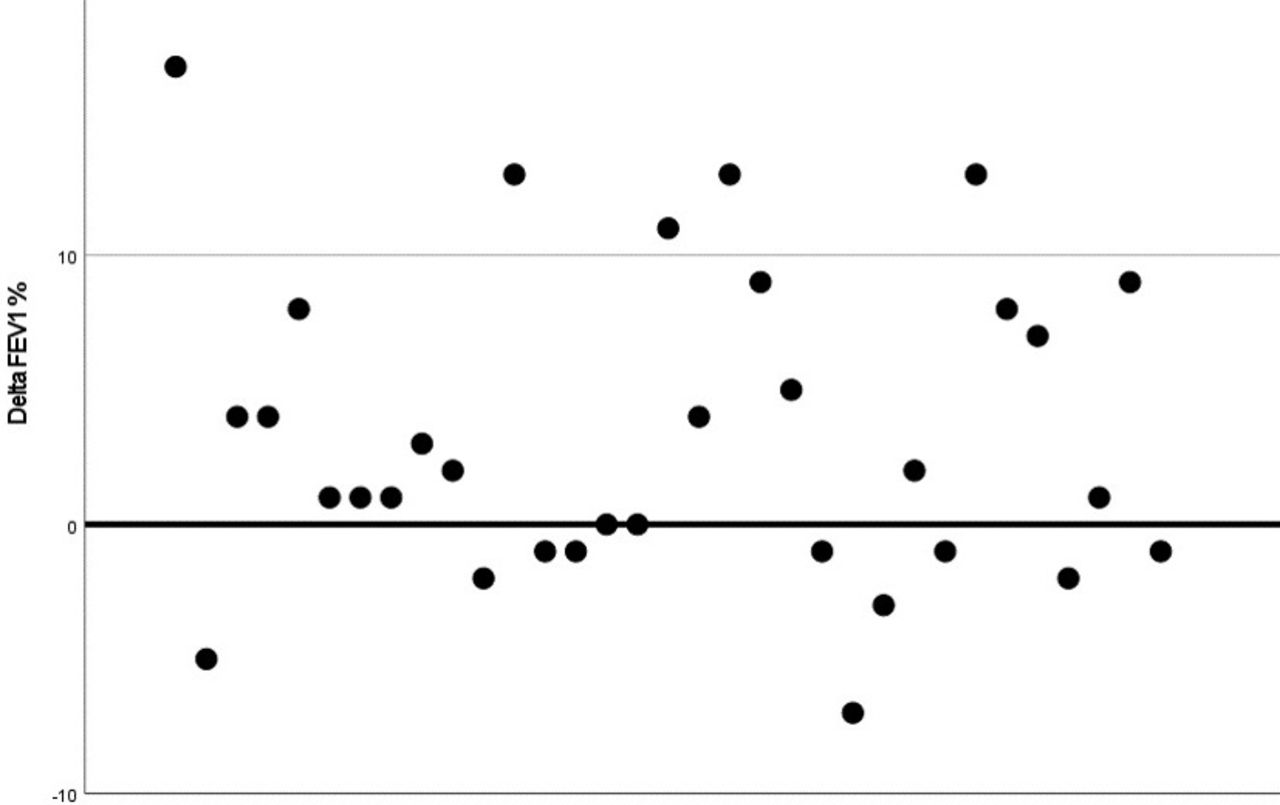
There was statistically significant improvement of FEV1% pred. after ssBACE in all patients (p value=0.004) (shown in figure 2). Patients with FEV1 <40% pred. showed improvement in 71% (p value 0.007) vs 64% of all patients. There was no statistically significant change in BMI before and after ssBACE (p value=0.17). Patient data are given in table 1.

{kind=link}
{kind=link}
Delta FEV1% pred. is the difference of FEV1% pred. before and after super selective bronchial artery coil embolisation; black dots represent the delta values of each of the 34 patients. Dots above the bold base line of 0 show improvement in FEV1% pred. after super selective bronchial artery coil embolisation. Dots below represent deterioration of FEV1% pred. FEV1% pred., functional end-expiratory volume in 1 s in % predicted.
Patient data
Super selective bronchial artery coil embolisation
Aortography with selective bronchial angiography was carried out in all cases, and hypertrophied bronchial arteries leading to the affected lobe were selectively embolised with coils. Fourteen patients received one single intervention (41.2 %). Reinterventions were carried out in case of recurrence of haemoptysis. In two cases reinterventions were primarily planned 3 and 10 days later but counted as two interventions. Twenty patients received at least one reintervention (58.8 %). Thirteen patients (38.2 %) received two interventions; 2 patients (5.9%) received three interventions; 3 patients (8.8 %) received four interventions; and 2 patients (5.9 %) received six interventions. Bronchial artery-to-pulmonary artery shunting was visible in all 34 patients.
Reintervention in the same lobe was carried out in 12 patients (35.3%). At selective angiography for reintervention during the 5-year observation period, recanalisation of a formerly treated vessel was found in three patients after 5, 14 and 24 months, respectively, with recanalisation of one bronchial artery in two patients and of one NBSA in one case. The other nine patients had to undergo reintervention due to neovascularisation in nine cases with additional incomplete embolisation in one case as shown in figure 1B.
No severe complications as defined by the Society of Interventional Radiology occurred.27 Intraprocedural transient minor stinging pain and mild coughing were noted in some patients. In 64.7% (22 of 34) of patients, ssBACE was carried out during fall and winter months, from October to March. Localisation of haemoptysis based on patient’s perception and angiography was correct in all cases. At first intervention, the right upper lobe was embolised in 56%, the middle lobe in 35%, the right lower lobe in 35%, the left upper lobe in 24%, the lingula in 15% and the left lower lobe in 21%. Procedural data are listed in table 2.
Super selective bronchial artery coil embolisation procedural data
Bacterial carrier status
Bacterial sputum colonisation is listed in table 3. Burkholderia cepacia was found in one patient.
Bacterial carrier status at the time of intervention
Discussion
To our knowledge, this is the first publication of BAE using only coils in patients with massive haemoptysis and CF. In the literature, coil embolisation is often not recommended as it is believed to show high rates of recanalisation on the one hand and to preclude any more peripheral access in case of recanalisation on the other.23 28–31 We could not find robust evidence for this theory and our recanalisation rate was low with 8.8%. Incomplete embolisation of NBSA was the cause of recurrence in the same lobe in only one case, and recanalisation of NBSA was found in one case. Hypertrophied NBSA were found in 50% of patients, but only 24% of NBSA were embolised. Neovascularisation seems to play an important role in recurrence in the same lobe as this was the cause in 69% of patients.
In a recent study by Ishikawa et al, ssBACE was both safe and long-term effective in patients with haemoptysis.21 However, patients in this study suffered from a variety of underlying diseases and emergency interventions were excluded. Our data show that ssBACE is safe and effective as immediate and long-term treatment in massive haemoptysis in patients with CF including emergency interventions.
Henig et al raised concern about overall benefit as 14% of patients with CF who undergo m-BAE died within 5 months after intervention without conclusive explanation of this excess mortality.32 Martin et al reported a 30-day mortality rate of 14% after m-BAE20; Sweezey and Fellows reported a 3-month mortality rate of 30%.23 Five months after embolisation, only two patients (6%) had died in our study group, one of uncontrollable haemoptysis and the other of respiratory failure with FEV1% pred. of 19% before intervention. In our study group, 24-hour immediate success rate was 97%; intermediate outcome is good with 88.2% of our patients alive after 1 year as opposed to 64.8%–68% after m-BAE.5 23 Of our total number of patients, 72.8% were alive after 5 years as opposed to 24%–50% after m-BAE.5 22 23 This is especially important, considering that 39% of our patients had severely impaired initial FEV1 <40% predicted. After m-BAE, patients showed deterioration of lung function and higher risk of death and lung transplant.22 23 33 Massive haemoptysis itself causes significant deterioration of lung function over the year following massive haemoptysis.5 Interestingly, our study group showed significant improvement of FEV1% pred. after ssBACE, and especially in severely compromised patients with FEV1 pred. <40%. The 9-month non-recurrence rate of 64.7% in our cohort meets the suggested threshold of 65% success rate 9 months after BAE set by the Society of Interventional Radiology Standard of Practice Committee.27 Our reintervention rate of 58.8% is higher than 25%–55% of studies using m-BAE, but our observation interval was longer and mortality was lower, which both influence reintervention rate.13 21 34 Embolisation of hypertrophied bronchial arteries, be it selective or more radical, will immediately produce higher flow in other vessels. This mechanism, together with continuous inflammation in CF and concomitant upregulation of serum vascular endothelial growth factor, may promote hypertrophy of other vessels in the same region.32 Kato et al found control of inflammation caused by the underlying disease as the most significant factor affecting long-term results and recurrence rates after m-BAE.14 Thus, in CF, embolisation of all hypertrophied bronchial arteries at one point may not prevent future hypertrophy of other bronchial arteries and possible bleeding. Extensive occlusion of entire arterial territories might even harm patients suffering from CF, explaining accelerated respiratory failure after m-BAE.5 6 11 18 23 32 Vidal et al described patients who had undergone m-BAE to be more likely to die than to present with recurrent major haemoptysis.22 Considering these data, many patients will not suffer from recurrence but from respiratory failure after m-BAE. m-BAE might cause ischaemia of larger areas of lung tissue in an already compromised lung in CF and might impede antibiotic exposure of infected tissue in advanced CF lung disease. In ssBACE, the embolised territory is smaller and collateral vessels remain open for blood supply as we followed a protocol of restricting intervention to the culprit vessel only and to a maximum of three lobes per intervention. Preservation of more vital lung tissue and herewith possibly better antibiotic access to the affected lung tissue might explain the striking difference in FEV1% pred. development after ssBACE compared with m-BAE.20 22–24 35 In our cohort, ssBACE not only achieved sufficient haemostasis but, as important, also provided excellent long-term outcome. However, PVA being the most commonly used microsphere embolic material, we could not differentiate between different microsphere materials in the literature. We therefore cannot directly compare coils with a specific microsphere material.
In advanced CF lung disease, bronchial artery-to-pulmonary artery shunting is common.6 8 14 36 One hundred per cent of our patients showed shunting, suggesting this to be part of the pathogenesis of haemoptysis in CF. The use of small embolisation particles in the presence of shunting may cause severe complications such as microembolisms to lung tissue, spine and brain with dysphagia, bronchial necrosis, bowel ischaemia, paraplegia, myocardial infarction and cerebral stroke with complication rates up to 6.6% in m-BAE.6 23 36–39 In our study group, no severe complications were reported despite the presence of shunts in all patients. Bronchopulmonary anastomoses are approximately 325 µm in size,28 why several authors advise the use of particles not smaller than 500 µm or even 2 mm in case of visible shunting.6 8 20 Inadvertent embolisation of pulmonary arteries with microspheres might therefore be discussed as explanation for deterioration of FEV1% pred. in m-BAE but not in ssBACE. Perhaps the use of larger microspheres 900–1200 µm in size should be considered. Adverse events with ischaemia of different organ systems seem to be a major risk worth taking into consideration when carrying out BAE. Coils are at least 2 mm in size, ruling out direct inadvertent embolisation and embolisation through shunts. The prevention of severe complications due to the large size of coils and at the same time only flow reduction and not complete flow cessation in the affected lung territory might be valuable arguments for the use of coils.
Chronic hypercapnic respiratory failure is a common finding in advanced CF. Arterial blood is delivered to alveolar capillaries through these bronchopulmonary anastomoses transporting arterial hypercapnic blood. In animal models, 30% of CO2 elimination is through a hypertrophied bronchial circulation.40 Henig et al postulate that in abnormal ventilation/perfusion distribution in CF, increased bronchial flow delivers arterial blood with high PaCO2 providing a second opportunity for gas exchange. This effective recirculation of blood with increased PaCO2 augments the elimination of carbon dioxide.32 At the same time, oxygen exchange might be impaired as arterial blood is shunting into pulmonary vessels. The role of bronchial artery-to-pulmonary artery shunting and its contribution to pathogenesis and gas exchange is not yet well understood.
Microbiology
Chronic infection with Pseudomonas aeruginosa and B. cepacia is associated with more rapid decline in lung function but with reduced association with massive haemoptysis.5 In our cohort, record of P. aeruginosa and B. cepacia was as well associated with reduced lung function as 92% of patients with FEV1 <40% pred. showed positive sputum cultures. However, we cannot confirm a reduced association with haemoptysis as 79% of patients had positive sputum cultures for P. aeruginosa compared with 58% normal prevalence in this age group.41 The prevalence of 44% of Staphylococcus aureus is lower than the normal prevalence of 68% at this age.41 Chronic infection with Aspergillus fumigatus was higher with 47.1% in our cohort compared with 35% normal prevalence at this age. The role of fungi in the CF lung is still not well elucidated, but evidence of a harmful and complex role is getting stronger.42
Nine per cent of patients presented with liver cirrhosis as opposed to 4.2% in the American CF population, and 17.6% of patients had concomitant diabetes mellitus compared with 30.6%.41
Summary
In adult patients with CF and massive haemoptysis, ssBACE has good short-term and excellent long-term outcomes in our cohort. ssBACE might bear important advantages as embolisation is less radical, leaving smaller vessels to not only supply the lung tissue to remain vital but possibly also antibiotic therapy to better access inflamed territories. Since the primary aim of the embolisation is to achieve short-term haemostasis, long-term survival and non-recurrence, our data support the use of coils and a prudent restricted protocol.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Ethics approval
This study complies with the guidelines for human studies and was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. It was approved by the ethical committee related to the institution (AEKNO approval file number 2016/181).
References
Footnotes
Contributors MD: conception and design of the study, acquisition, analysis and interpretation of data, and writing of the original draft. DMR: revision and editing of the original draft. CD-S: formal analysis/statistics, revision and editing and figures. FS: revision and editing, data acquisition. SS, CN, PK, HW, OE, JG-O, AS, VS and KP: data acquisition. FW: revision and editing, ensuring accuracy and integrity of the study. MJM: supervision, revision and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.