Article Text

Abstract
Background Breathlessness is prevalent in severe disease and consists of different dimensions that can be measured using the Multidimensional Dyspnea Profile (MDP) and Dyspnea-12 (D-12). We aimed to evaluate the feasibility of MDP and D-12 over telephone interviews in oxygen-dependent patients, compared with other patient-reported outcomes (modified Medical Research Council (mMRC) and Chronic Obstructive Pulmonary Disease Assessment Test (CAT)) and with completion by hand.
Methods Cross-sectional, telephone study of 50 patients with home oxygen therapy. Feasibility was assessed as completion time (self-reported by patients and measured), difficulty (self-reported) and help required to complete the instruments (staff). Completion time was compared with mMRC and CAT, and feasibility was compared with completion by hand in cardiopulmonary outpatients (n=182). Feasibility by age and gender was analysed using logistic regression.
Results Of 136 patients approached, 50 (37%) participated (mean age: 72±10 years, 66% women). Completion times (in minutes) were relatively short for MDP (self-reported 6 (IQR 5–10), measured 8 (IQR 6–10)) and D-12 (self-reported 5 (IQR 3–8), measured 3 (IQR 3–4)), and slightly longer than mMRC (median 1 (IQR 1–1)) and CAT (median 3 (IQR 2–5)). Even though the majority of patients required no help, more assistance was required by older patients. Compared with patients reporting by hand, completion over the telephone required somewhat longer time and more assistance.
Conclusion Many patients with severe oxygen-dependent disease were unable or unwilling to assess symptoms over the telephone. However, among those able to participate, MDP and D-12 are feasible to measure multiple dimensions of breathlessness over the telephone.
- perception of asthma/breathlessness
- respiratory measurement
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Can breathlessness be measured over telephone using the Multidimensional Dyspnea Profile (MDP) and Dyspnea-12 (D-12)?
In participating patients, breathlessness can be measured over telephone using the MDP and D-12 for patients with oxygen-dependent disease.
Follow-ups of patients with severe illness, who are often limited to their home and can have a hard time or be unable to attend clinical visits, can be difficult and using telephone could possibly increase compliance.
Introduction
Breathlessness is a common symptom in patients with cardiorespiratory and other advanced diseases.1 The symptom is defined as the perception of breathing discomfort and consists of distinct sensations that vary in intensity.1 Breathlessness associates strongly with impaired physical performance, health-related quality of life (HrQoL),2 increased anxiety and depression, and increased risk of hospitalisation and death.1 3–7 Despite its importance, breathlessness is often under-reported, unmeasured and undertreated in clinical practice.8 9
Measurement of breathlessness should optimally be through self-report of the relevant aspects (dimensions) of the symptom, as breathlessness pertains to the personal perception of abnormal and distressing internal states.1 Assessment to date has often been through unidimensional instruments, which are short, feasible and with few instructions, such as the modified Medical Research Council (mMRC) scale and the Chronic Obstructive Pulmonary Disease Assessment Test (CAT).10 However, these instruments pertain to the symptom’s impact on physical function and HrQoL and do not measure breathlessness itself, nor associated dimensions such as its emotional impact (ie, anxiety, depression or fear). Multiple dimensions of breathlessness can be assessed through the instruments Multidimensional Dyspnea Profile (MDP)11–13 and Dyspnea-12 (D-12).13–15
Many patients with severe illness, such as respiratory failure treated with home oxygen therapy, are limited to their home and can have difficulties or be unable to attend clinical visits—a situation aggravated by the COVID-19 pandemic. There is an increasing need to convert physical outpatient visits to remote contacts such as telephone calls, both for clinical and research purposes. However, knowledge on the feasibility of MDP and D-12 for remote monitoring is limited, and no study has evaluated use of the instruments through telephone interviews.
The primary aim of this study was to evaluate the feasibility of assessing breathlessness using the MDP and D-12 over the telephone in patients with home oxygen therapy. Secondary aims were to compare the completion times of MDP and D-12 to those of mMRC and CAT (for reference), and to compare the feasibility of completing MDP and D-12 over telephone to completion by hand using a manual hard copy.16
The aims of this study translate into the following research questions:
How long does it take for instruments to be completed (estimated by patient vs measured by investigator)?
How difficult are the MDP and D-12 perceived to be and how much assistance is required administering these instruments over telephone?
Do age and gender predict more need for assistance?
Do completion times and difficulty differ between administration modes (telephone interview vs manual hard copy)?
Materials and methods
Study design and population
This was a cross-sectional telephone study with cross-linkage to registry data. The responsible oxygen nurse at five different cities in Sweden (Gävle, Halmstad, Karlshamn, Karlskrona and Lund) provided a potential list of patients, and these were all approached by telephone.
Inclusion criteria (all required) were age 18 years or older, chronic cardiorespiratory disease, treated with home oxygen therapy and an oral consent to participate over telephone. Exclusion criteria were inability to understand Swedish, cognitive impairment as judged by the researcher, not wanting to participate or not being reachable by telephone.
Patient and public involvement
Patients were not involved in the development, design, recruitment and conduct of the present study. Results will not be disseminated to study participants.
Procedures and assessments
Patients were approached through interview-led telephone assessment and structured surveys were conducted by three medical student (TB, MEkl and ES). A standardised script was read to patients including information on the study aim and procedures, and informed oral consent to participate was obtained before any assessments. The validated Swedish versions of MDP, D-12, mMRC and CAT were read to patients through telephone without the patients having a hard copy to refer to.17 18 The time frame for all patient-reported outcomes were ‘during the past 2 weeks’16 and is previously validated in studies for MDP and D-12.12 14 16 17
Multidimensional Dyspnea Profile
The MDP measures overall breathing discomfort and the intensities of five sensory qualities (5SQs) and emotional impacts (depression, anxiety, frustration, anger and fear) of breathlessness.11 19 MDP was recorded as an A1 overall unpleasantness score (range 0–10), perception score (sum of A1 and sum of 5SQ scores (range 0–60)) and an emotional response score (sum of A2 (range 0–50)). Higher scores indicate worse breathlessness. The instrument is rated highly for usefulness and clarity, is easily understood and quick to complete.16 20 MDP can compare breathlessness in laboratory and clinical research across underlying diseases and settings.11 12 It can be completed by a healthcare provider or self-completed, but the investigator must define a specific time frame or event.20 MDP is translated into Swedish17 and is deemed valid in terms of factor analysis and test–retest reliability in outpatients with COPD (24.7%), asthma (21.4%), heart failure (19.2%) and idiopathic pulmonary fibrosis (IPF) (18.7%).12 13
Dyspnea-12
D-12 is validated for quantifying different aspects of breathlessness across several cardiorespiratory diseases such as COPD, chronic heart failure or interstitial lung disease.13 15 It is easy to understand and is usually completed within 5 min.10 15 16 The instrument provides an overview of overall breathlessness severity with regard to breathlessness intensity, unpleasantness and psychological response.15 21 D-12 is validated linguistically and clinically into Swedish.14 18 The D-12 total score (range 0–36), as well as subdomain scores, were recorded and analyses were conducted. A higher score represents worse breathlessness.
Use of the MDP and D-12 was approved by the copyright holders of MDP (Professor Robert Banzett, USA) and D-12 (Professor Janelle York, UK). All data were first recorded in a password-protected Excel document (MS Office V.2010) and thereafter only coded, non-identifiable data were processed and presented.
The order of MDP and D-12 were randomised using www.random.org22 to facilitate unbiased comparison. Directly after completing each of the MDP and D-12, feasibility related to the instruments was assessed using the questions (1) ‘How long did you perceive the instrument took to complete?’ (in minutes) (self-reported time); (2) ‘Did you need any help understanding and completing the instrument?’ (yes/no); and (3) ‘How difficult was the instrument to understand and complete?’ (1: not at all, 2: a little, 3: moderate and 4: very difficult) (perceived difficulty). Thresholds for feasibility were not prospectively proposed. Researchers recoded the actual completion time for each instrument (measured time) and rated ‘How much help was required by researchers to complete the instrument’ (1: none, 2: a little, 3: moderate and 4: a lot) (help required). For mMRC and CAT, only self-reported time and measured time were recorded.
The data from the telephone survey were cross-linked with data from the Swedish Registry for Respiratory Failure (Swedevox).8 Swedevox includes data on patients starting home oxygen therapy in Sweden since 1987, with coverage of about 85%.8 23 Registry data included demographics and physiological variables, date starting and type of oxygen therapy, diagnosed disease, height and weight, spirometry forced expiratory volume in 1 s and vital capacity.8 The registry data from Swedevox were entered into the register when the patient’s oxygen therapy was initiated.
Statistical analyses
Baseline patient characteristics were presented as mean±SD for continuous variables and frequency (%) for categorical variables. Feasibility data (self-reported time and measured completion time, perceived difficulty and help required) were presented as median score with IQR due to skewed distributions. The differences in feasibility between MDP and D-12 were compared using the non-parametric Wilcoxon signed-rank test.
Factors associated with patients requiring more help by staff members to complete MDP and D-12, separately, were analysed using logistic regression models. Age and gender were independent variables, analysed separately and concurrently. For the analysis, help required was recoded as a dichotomous variable: 0=‘none’ or ‘a little’; 1=‘moderate’ or ‘a lot’. Estimates were presented as odds ratios (ORs) with 95% confidence intervals (CIs).
Feasibility was also compared with a recently published study where the instruments MDP, D-12, mMRC and CAT were self-reported by hand at a clinical visit by 182 outpatients with cardiopulmonary disease.16 The same rating scales and instructions were provided for both patients interviewed over telephone and patients self-completing the instruments by hand with a manual hard copy. A two-sided p value of <0.05 was considered statistically significant. All statistical analyses were conducted using the software package IBM SPSS Statistics for Macintosh V.27.0.
Results
Population
Between 6 May 2019 and 17 March 2021, 136 patients were approached over the telephone, of whom 50 (37%) were included (figure 1). Of the non-participants, 39 (29%) did not want to participate, for example, due to hearing problems or feeling too ill; 15 (11%) did not answer the telephone; 18 (13%) had closed numbers; 8 (6%) were listed with the wrong number; and 6 (4%) did not meet the inclusion criteria. Three (6%) of the participants did not provide data on all four instruments.
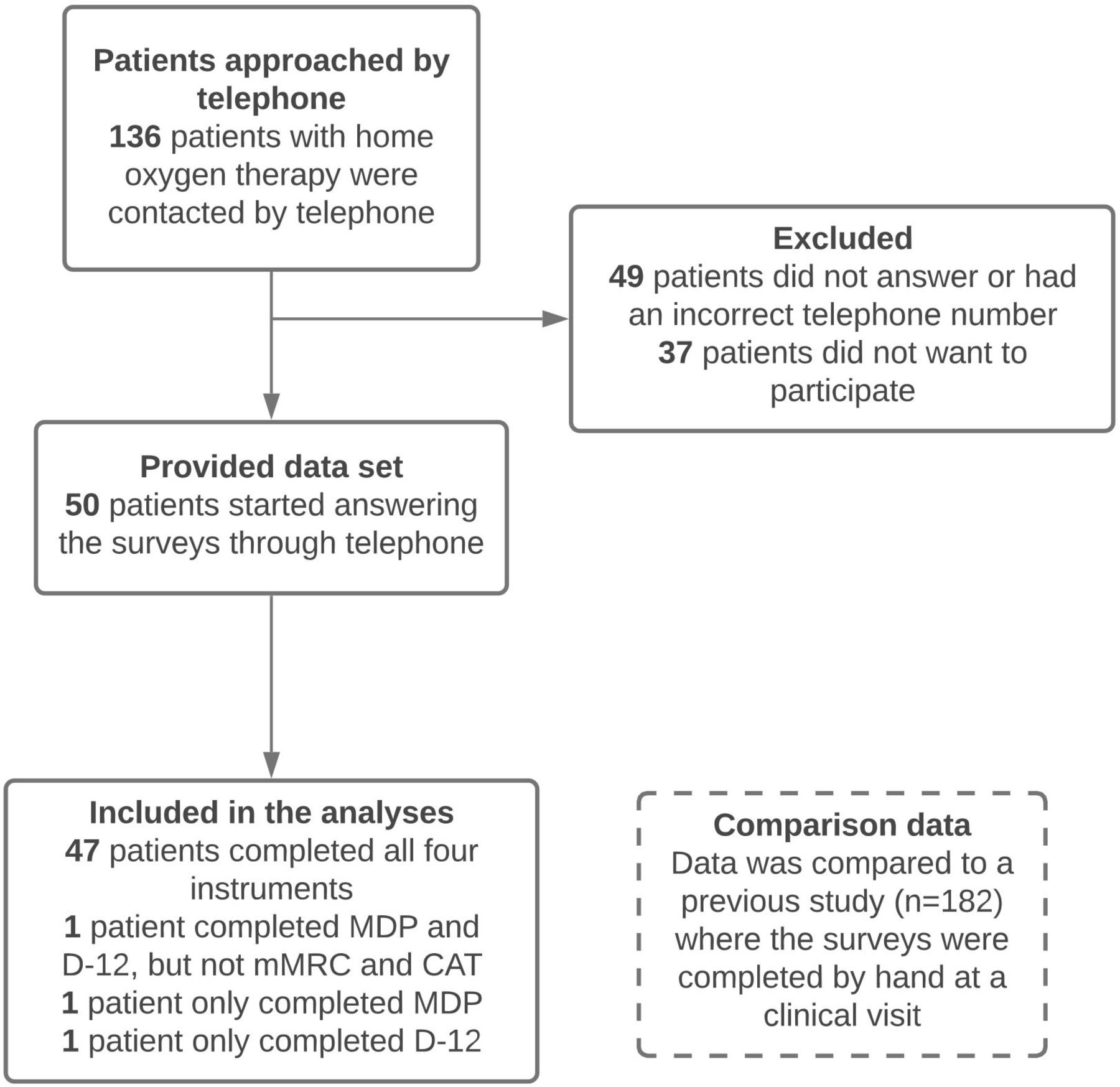
Flowchart of study population enrolment. CAT, Chronic Obstructive Pulmonary Disease Assessment Test; D-12, Dyspnea-12; MDP, Multidimensional Dyspnea Profile; mMRC, modified Medical Research Council.
Included participants had a mean age of 72.0±9.6 years; 66% were women and had received oxygen therapy for a median of 2 years (IQR 1–3, range 1–13) (table 1). There were 29 (58%) patients randomised to answer MDP before D-12, and 21 (42%) patients answered D-12 before MDP.
Characteristics of 50 participants with home oxygen therapy
Completion time
Completion times (self-reported and measured) for each instrument are presented in figure 2. Completion time for MDP was self-reported to a median of 6 min (IQR 5–10, range 1–60), whereas measured to a median of 8 min (IQR 6–10, range 4–28) (figure 2). Thus, patients tended to perceive the MDP required less time than the measured actual time, although the difference was not statistically significant (p=0.054). Completion time for D-12 was self-reported to a median 5 min (IQR 3–8, range 1–15), whereas the measured time was a median 3 min (IQR 3–4, range 2–9). Thus, patients perceived the D-12 to take slightly longer than the actual time taken (p<0.001). MDP required more time to complete than D-12 with consideration of both self-reported time (p=0.001) and measured time (p<0.001). The mMRC (median 1 (IQR 1–1)) and CAT (median 3 (IQR 2–5)) were both self-reported and measured to require less time to complete than MDP and D-12, respectively (p<0.05 across all analysis) (figure 2). There was a tendency that D-12 was often completed in less time than CAT, even though this was not statistically significant.

Completion times for different instruments through telephone interviews. Completion times of the instruments MDP, D-12, mMRC and CAT, respectively. Outliers are represented with circles. Extreme outliers are represented with x. One extreme outlier for ‘DP self-reported’ was 60 min and is not presented in this figure. Self-reported: as assessed by patients; measured: timed by researchers. CAT, Chronic Obstructive Pulmonary Disease Assessment Test; D-12, Dyspnea-12; MDP, Multidimensional Dyspnea Profile; mMRC, modified Medical Research Council.
Perceived difficulty and help required
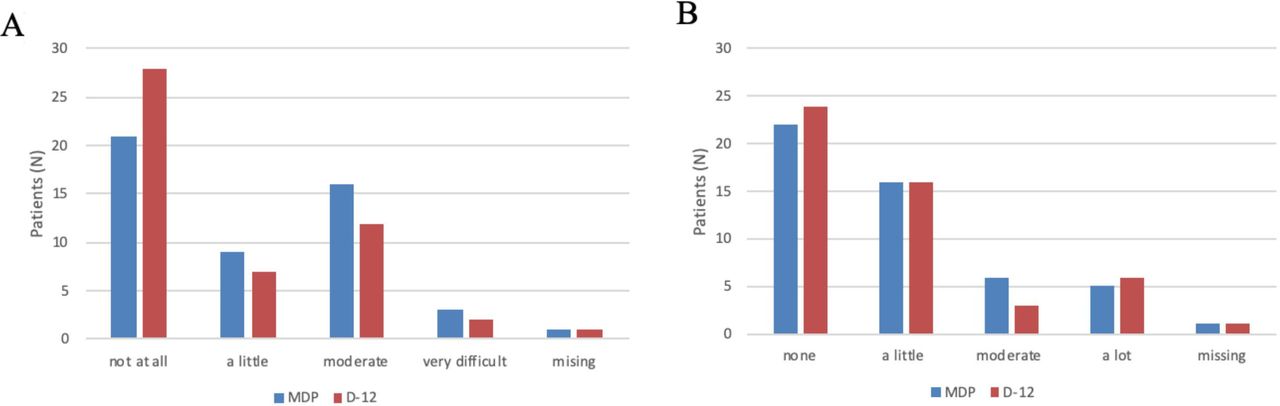
Perceived difficulty (by patients) and help required to complete the instruments are presented in figure 3. Patients reported the perceived difficulty of MDP to the median category 2 ‘a little’ (IQR 1–3), whereas patients’ perceived difficulty of D-12 was the median category 1 ‘not at all’ (IQR 1–3) (figure 3A). Patients tended to report MDP as more difficult than D-12, although the difference was not statistically significant (p=0.056). The median help required for both MDP and D-12 was the category 2 a little (IQR 1–2) (figure 3B), hence why there was no statistically significant difference between the two (p=0.305).

{kind=link}
{kind=link}
{kind=link}
Difficulty completing MDP and D-12 over the telephone in patients (n=50) with home oxygen therapy. (A) Perceived difficulty by patients. (B) Required help reported by researchers. Of the total of 50 patients, 1 patient (A,B) completed only MDP and 1 patient (A,B) completed only D-12. MDP, Multidimensional Dyspnea Profile. D-12, Dyspnea-12.
Older age, but not gender, was associated with greater need for assistance to complete the instruments MDP and D-12 over telephone (table 2).
Factors associated with requiring more help by researchers completing the MDP and D-12
Comparison to self-report by hand
The comparison cohort comprised 182 stable outpatients: mean age 67±14 years, 53% women, main diagnosis: COPD (24.7%), asthma (21.4%), heart failure (19.2%) and IPF (18.7%). All 50 patients in the telephone study had home oxygen therapy, whereas only 9 patients in the comparison study were oxygen dependent. In line with having more severe disease, the oxygen-dependent patients in the telephone survey also reported having worse breathlessness scores (table 3).
Feasibility and scores of MDP and D-12 completed over telephone versus by hand
Compared with the patients reporting by hand with a manual hard copy, completing the instruments over telephone interview required longer time and more assistance (table 3). MDP was self-reported to ≤10 min by 80% of patients reporting by hand vs 74% of patients answering over telephone (table 3). D-12 was self-reported to <5 min by 75% of patients reporting by hand vs 36% of patients answering over telephone (table 3).
Discussion
Main findings
MDP and D-12 are feasible and valid instruments that can measure breathlessness through telephone interviews in chronic cardiorespiratory patients with home oxygen therapy. D-12 was completed faster than MDP, but there was no difference regarding the perceived difficulty or help required to complete MDP compared with D-12. Older patients required more assistance with answering MDP and D-12, whereas men and women required a similar amount of assistance. Compared with the study completed by hand,16 patients in the telephone study perceived the instruments to have a higher completion time, greater difficulty and reported higher subdomain scores.
What this study adds
This is the first study to investigate the feasibility of using telephone interviews to measure the multidimensional aspects of breathlessness. The measured completion times for MDP and D-12 were consistent with those of previous reports.10 16 The present study’s measured completion time of MDP was a median of 8 min, and 80% were reported to have completed in ten minutes or less, in accordance to a previous study.16 D-12 had a median measured completion time of 3 min and 88% of patients had completed the instrument in less than 5 min, which compared well with all previous results.10 16
In the study completed by hand, perceived difficulty for both MDP and D-12 was reported as ‘not any’ or ‘a little’ by more patients than in the telephone study. This could suggest that MDP and D-12 are easier to fill in by hand compared with over telephone. However, compared with the patients completing by hand, the patients reporting over telephone were older and with more severe diseases. This study population difference can explain the longer time and somewhat lower feasibility seen in patients reporting over telephone. However, the present findings show that among people who were able to participate over the telephone, MDP and D-12 were easy to use, responsive and feasible in evaluating breathlessness.
Strengths and limitations
Strengths of the present study are the high completion rate of the four instruments and the randomisation of MDP and D-12 to avoid order bias. All patient reported outcomes used the same time frame and the telephone survey was conducted in a structured way using standardised assessments.
Limitations include the relatively small sample size, which however was prespecified in the study protocol. Many patients approached were not reachable, felt too sick or did not want to participate. The large number of non-participants likely reflects the severe underlying disease, which could have created a selection bias as those feeling too sick did not participate. Second, the inclusion criteria of ‘adequate cognitive ability’ is hard to reliably evaluate over telephone, wherefore some patients with impaired cognition may have been included and thereby affected the feasibility estimates, but would reflect the ‘real-life’ conditions. Third, a potential time bias could be present as many patients required questions repeated several times due to hearing problems or because they did not understand the question. Finally, compared with the patients self-completing by hand, the patients reporting over telephone were all chronically ill patients with oxygen therapy and hence more severely ill patients. The difference in study population suggests that the feasibility of completing the instruments over telephone could be higher than reported. The more severely ill study population could also explain why the patients participating over telephone reported higher completion difficulty and higher breathlessness scores compared with the patients self-completing the instruments by hand.
Implications and suggested improvements
For the clinician and researcher alike, the present findings support further research into measurement of breathlessness using telephone interviews. Even though the sample size was small (making generalisation hard) and the recruitment of patients was difficult (creating a selection bias), the results of this study imply that follow-ups of oxygen-dependent cardiorespiratory patients could be conducted over telephone in the future with several advantages as the instruments were relatively quick, easy and feasible to use. A consideration necessary to take into account is that many patients do not have the energy or ability to talk over telephone, so measurement of breathlessness over telephone should only be chosen for patients suitable for this type of follow-up.
Another implication of the study’s results, is more easily deciding if MDP or D-12 is the preferable instrument to use. D-12 was often completed in shorter time than CAT, suggesting that even when short on time, a multidimensional instrument is possible to use.
Future research should evaluate the instruments MDP and D-12 over telephone in further patient cohorts and with larger sample sizes. Improvements could be to standardise the instructions of MDP and D-12 to telephone use and send out the instruments on paper in advance, which could potentially reduce completion time and the help required. It would be interesting to study the order effect of MDP and D-12, look at additional predictors for completion difficulty such as years with home oxygen therapy or high breathlessness scores, and see if any predictors exist for patients with high completion time.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Personal information is protected by the Swedish law of personal record. The study protocol was approved by the regional ethical review board at Lund University (DNr: 2016/16), and an informed oral consent to participate was obtained from all patients.
Acknowledgments
The authors thank all nurses for dedicating their time to this study and for providing lists with possible candidates. Nurses contributing were from the following hospitals: Gävle; Lena Mårtensson Respiratory Nurse (RN), Halmstad; Susanne Andersson (RN), Karlshamn; Kirsten Johansson, Karlskrona; Elisabeth Witte (RN), Lund; and Jonas Einarsson, MD. We thank all patients for taking their time to participate in this study.
References
Footnotes
Contributors MEks designed and supervised the work, accepts full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish. MEkl and AP acquired the data. ES, MEkl and TWB collected the data. TWB analysed the data, designed figures and tables, and drafted the article. MEks and TWB interpreted the data. MEks, AP and MEkl commented and revised the article. All authors gave the final approval of the manuscript.
Funding ME was supported by unrestricted grants from the Swedish Society for Medical Research and the Swedish Research Council (Dnr 2019-02081).
Competing interests None declared.
Patient and public involvement Patients and the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.