Article Text

Abstract
Objective Data on asthma hospitalisations are a useful source of patient morbidity information. In Ghana, the length of stay (LoS) and sociodemographic factors of patients hospitalised for asthma and its exacerbation are understudied. We aimed to investigate the time to discharge and assessed factors associated with length of hospital stays of asthmatics in Ghana.
Methods Retrospective analysis of hospitalised patient with asthma records between 2012 and 2017 from the nationwide Ghana Health Service District Health Information Management System 2 database. We calculated the cumulative incidence function for discharge stratified by age group and sex. Multivariable Cox regression was used to investigate the association of sociodemographic characteristics with the LoS.
Results Of 19 926 asthma-associated hospitalisations, 730 (3.7%) were due to asthma exacerbation. Overall mean age was 34 years (SD=24.6), in 12 000 (60.2%) hospitalisations, patients were female. There were 224 deaths (1.1%). Median LoS was 2 days (IQR: 1–3) with almost 90% of all patients discharged by the seventh day. Age and region were among the covariates showing significant association with LoS. Age below 10 years (HR: 1.39 (1.11 to 1.78)) was associated with early discharge while comorbidity and health insurance ownership were associated with late discharge (p<0.001). LoS did not vary by sex. Compared with the Greater Accra region, patients in other regions had shorter LoS, especially the Ashanti and Upper West regions (p<0.001). LoS increased annually, but was highest in 2016 (HR: 0.94 (0.90 to 0.98)).
Conclusion Disparities in LoS across regions, and an overall increasing annual trend in Ghana call for tailored healthcare resource allocation. Longer LoS implies that patients are often absent from school or work leading to substantial financial and emotional costs to individuals and families.
- asthma
- asthma epidemiology
- COPD exacerbations
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data used is published with this article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
How can routinely collected administrative health services data be used to shed light on factors determining hospitalisation duration for patients with asthma and asthma exacerbation?
Our results indicate that age and geographical region are associated with length of hospital stay in Ghana, allow for better hospital resource allocation, and more targeted measures in the outpatient setting to prevent hospitalisation.
We were able to use a large database on hospitalisations with nationwide coverage that includes information on sociodemographic factors, thus allowing targeted outpatient measures to prevent resource-intensive hospitalisations.
Introduction
Asthma is a chronic respiratory disease that is heterogeneous in nature with patients exhibiting different phenotypes.1 It is characterised by inflammation of the airways which reduces the amount of airflow into the lungs resulting in hyper-responsiveness causing wheezing, coughing and dyspnoea.2 The diagnosis of asthma can be based on medical history, physical examination and spirometry3 which are equally available in low-income and lower-middle-income countries (LMICs) health facilities. Management of the condition is usually done to prevent asthmatic attacks.4 Asthma is a complex condition with no single cause, having different risk factors.1 5 Asthma forms a major part of non-communicable diseases6 and has contributed to the increase in global deaths and disability. Asthma also contributes substantially to the global economic burden and reduction of quality-adjusted life years.7–10 It is estimated that over 339 million people were asthmatic globally in 2016 with 417 918 associated deaths,6 corresponding to about 1000 people dying each day.6 8 Moorman et al11 reported some geographic variations in asthma morbidity and its prevalence across the USA. Similarly, there exist seasonal variations in the prevalence of asthma exacerbations as well.12
In LMIC regions like Sub-Saharan Africa, the prevalence of asthma is increasing steadily and has significantly contributed to mortality in the region. The number of asthma cases in Africa in 1990 was estimated to be 74.4 million, increasing to 94.8 million and 119.3 million cases in 2000 and 2010 respectively.5 13
In recent years, there has been worldwide recognition of the healthcare utilisation due to asthma, especially in low-income and middle-income countries with a very high treatment-associated cost.5 14
The concept of measuring the length of stay (LoS) for hospitalised patients with a particular disease is a useful tool in assessing the disease morbidity and mortality in a population. It could also be used as an indicator for asthma severity, and as a key factor influencing hospital capacity utilisation. There is a relatively small body of literature on the prevalence and length of hospitalisations due to asthma and asthma exacerbation in Africa.14–16 This is due to limited funding for research on non-communicable diseases in the region compared with other WHO regions.17 Independent cross-sectional studies conducted between 2001 and 2018 in Africa have shown that the prevalence of asthma varies within the region with estimates between 2.7% and 20.3%.18 19 However, the extent of the observed increase or heterogeneity could be explained by the differences and changes in diagnostics. Nevertheless, this is only assessable through increased research on asthma and its comorbidities on the continent.14 20 21
Literature on the incidence, prevalence and risk factors (such as age, sex, educational attainment, comorbidities) of asthma in Ghana and other LMICs is rare.22 Existing studies focused on young populations aged 5–16 years5,5 13 16 20 as well as women21 with nearly no studies on asthma exacerbation.5 Risk factors for developing asthma have already been widely reported in Ghana.5 However, while studies in high-income countries have identified risk factors for hospital LoS due to asthma such as increasing age, female sex, educational attainment and income level22 23 such studies are currently not available in Ghana or other LMICs. Hospital LoS is especially important for patients who are still in school or for those working. Understanding the hospitalisation duration of hospitalised patients with asthma and patients who were asthma exacerbated is vital for planning and informing care but requires a comprehensive national health database. Ghana lacks comprehensive population-based registries or national LoS estimates on asthma using local data.5 However, its routine health database of in-patient records from both public and private hospitals (DHIMS-2) has nationwide coverage making it a useful resource. It is against this background that we sought to quantify hospital LoS for patients with asthma and patients who were asthma exacerbated, and analyse sociodemographic factors that influence LoS using data from the DHIMS-2 database from 2012 to 2017.
Methods
Study design and setting
In this retrospective study, routinely collected healthcare data of hospitalised patients in Ghana were used.
This study was conducted in Ghana with a land area of 2 38 537 km2 and a population density of 103 persons per km.2 The population of Ghana in 2010 was 24.7 million with 51% urban dwelling. Life expectancy at birth was estimated at 60 years for males and 63 years for females in 2010.24 Ghana was divided into 10 administrative regions at the time of this study. Health services are delivered in public and private health facilities which are supervised by the Ghana Health Service. The provision of health services in Ghana ranges from the highest of tertiary hospitals to the lowest of Community-Based Health Planning and Services. Currently, there are about 6000 health facilities providing health services in Ghana with approximately 75% being government owned. The two largest cities Accra (national capital) and Kumasi (regional capital of the Ashanti Region) have the highest concentration of health facilities and doctors in the country. It is estimated that about 66.2% of persons who report ill or injured consult a health practitioner in Ghana. Overall, 67.6 % of the population is registered or covered by the health insurance scheme.25 Most health facilities report on health indicators into the DHIMS-2. Hospital admissions usually in district hospitals and above.
Data source
Data for this study were extracted from the DHIMS-2 database of the Ghana Health Service for a 6-year (2012–2017) period. The system has data on all patients admitted to public and private health facilities except for the two premier teaching hospitals which report specific indicators. It is currently the most comprehensive national database on routine health data in the country.26
Participants and variables
All patients having asthma International Statistical Classification of Diseases and Related Health Problems (ICD) codes version 10 codes (ICD-10 codes: J45.0–J45.9) and status asthmaticus (exacerbation), (ICD-10 code: J46) as their principal diagnoses were considered for this study. Diagnoses were extracted primarily based on the ICD-10 codes, and additionally from analysing a free-text comment field. We used the search terms asthma or status asthmaticus in STATA regular expressions to extract asthma diagnoses without ICD-10 codes. Additional variables analysed in this study included several self-reported comorbidities recoded as (yes, no), date of admission and discharge, the outcome of admission (alive, dead, transferred) recoded as alive or dead, surgical procedure during hospitalisation (yes, no), health insurance ownership (yes, no) and sociodemographic characteristics of patients (5-year age groups, sex, educational level (none, below secondary, secondary and above) and occupation (employed, unemployed, unspecified)). The LoS was calculated in days as the difference between dates of admission and discharge plus 1 such that patients admitted and discharged on the same date had an LoS of 1 day.27
Data extraction and cleaning
The required data were extracted from the DHIMS-2 database in a spreadsheet and exported to STATA V.14 (Stata Corp, College Station, Texas, USA) for cleaning and analysis. The dataset was restricted to records of patients who had asthma or status asthmaticus as their principal diagnosis. Patients with missing data on relevant variables such as age, sex and date of admission were excluded from the analysis as these variables form the basis of our study. Missingness was assumed to be at random. To determine any seasonal pattern and its association with LoS, we partitioned the 10 regions of Ghana at the time of this study into two climate zones according to the Ghana Demographic and Health Survey (GDHS) demarcation.25 Climate zone 1 comprised of the southern and middle regions (Greater Accra, Eastern, Volta, Central, Western, Ashanti and Brong Ahafo), while climate zone 2 was made up of the three northern regions (Northern, Upper East and Upper West). There are varied rainfall patterns in these two climate zones, climate zone 1 has two wet and two dry seasons, while climate zone 2 has only one season each. There is also the harmattan season, noted for its dry dusty desert wind, which blows from the northeast and covers much of the country between December and March across both climate zones.25
Statistical analysis
We used frequencies to describe the annual number of hospitalisations due to asthma and exacerbation stratified by sex. Continuous variables such as age and LoS were described using means with SD and medians with IQRs. We investigated possible sex differences for continuous measures using t-tests for independent samples. For estimating the LoS distribution, the cumulative incidence function (CIF) from the Fine-Gray model28 was employed. Our outcome was discharged alive with in-hospital death as a competing risk event. A patient transferred to other hospitals for which the outcome of that patient cannot be linked in the DHIMS-2 database was considered to be discharged alive. We fitted the Fine-Gray model using the stcrreg command with a robust option to provide the CIF stratified by age group (0–4, 5–9, 10–14, 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80 and above) and sex. Group differences were evaluated using the Wald test. We then executed the stcurve command after the stcrreg command to plot the cumulative incidence of discharge. Our choice of the CIF compared with the traditional Kaplan-Meier (KM) method for LoS was influenced by the fact that KM cannot consider continuous covariates and does not consider competing risks. However, due to the relatively small case fatality of 224 (1.1%), we analysed the sociodemographic and other health-related factors associated with LoS using the Cox proportional regression model also with the robust option given by stcox. Furthermore, the Cox model is a better option for investigating causal relationships, while the CIF is better for estimating cumulative incidence under competing risk.28–31 The HRs with the 95% CI and p values were reported.
Patient and public involvement
We analysed anonymized secondary data from hospital admission and discharge records without patients and public involvement.
Results
Population characteristics
There were 19 926 records of hospitalised patients with asthma between 2012 and 2017 of which 730 (1.2%) were due to asthma exacerbation. Females constituted nearly two-thirds (12 000) of the patients hospitalised during the 6-year period. The mean age of females was 5 years higher than the mean age of males (36 years (SD=23) vs 31 years (SD=27)). Overall, the annual number of hospitalisations increased almost twofold from 2313 (11.2%) in 2012 to 4235 (21.3%) in 2016. Patients less than 10 years old constituted one-fifth of the admissions, while admissions for patients above the age of 40 years were few. Most patients were either unemployed (10 367, 52.0%) or had no formal education (9778, 49.1%). Health insurance ownership was very high among the patients 16 907 (84.9%). About one-third of patients admitted reported some comorbidities 6535 (32.8%) (table 1).
Sociodemographic characteristics and multivariate Cox proportional model of hospitalised patients with asthma and patients who were asthma exacerbated in Ghana, 2012–2017
Covariates with an indication for sex trends
Of all the sociodemographic factors assessed for sex differences, we found the age of the patient, educational attainment, occupational status, and outcome at discharge showing a significant trend (p<0.001). The region in which a patient is hospitalised and patients with comorbidity also had (p<0.05) sex differences although less pronounced.
Seasonal effects
Eighty per cent (16 014) of all admissions occurred in climate zone 1 (table 2). Thirty-one per cent (5034) of the admission occurred in December–March, corresponding to the dry season in climate zone 1, and 56% of admissions in climate zone 2 in October–April dry season. Northern Ghana, climate zone 2, experiences dry season between October and April. Middle and Southern Ghana, climate zone 1, experiences dry season between December and March. Most patients with asthma or exacerbated asthma were admitted during dry season.
Correlation of seasonality with asthma and asthma exacerbation among hospitalised patients in Ghana, 2012–2017
Cumulative incidence of discharge of hospitalised asthmatics
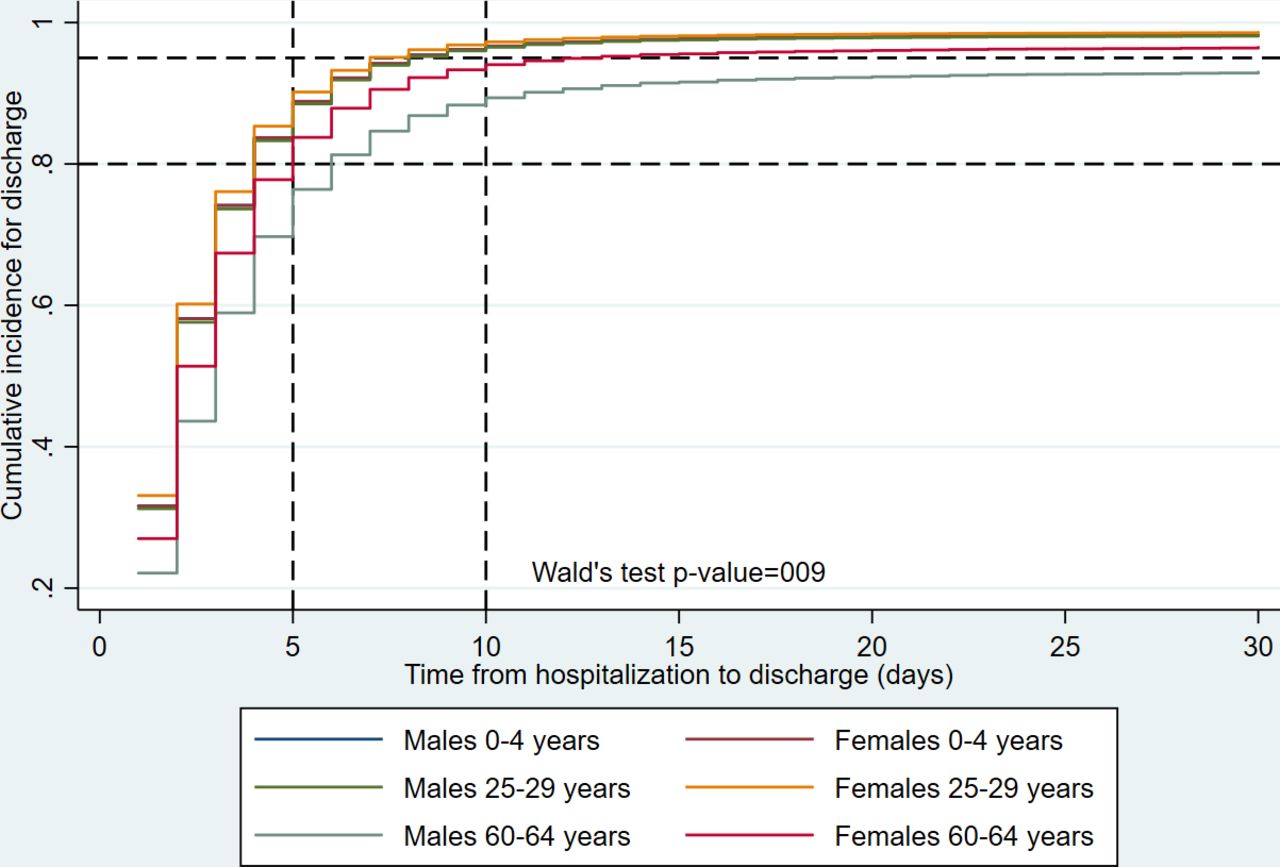
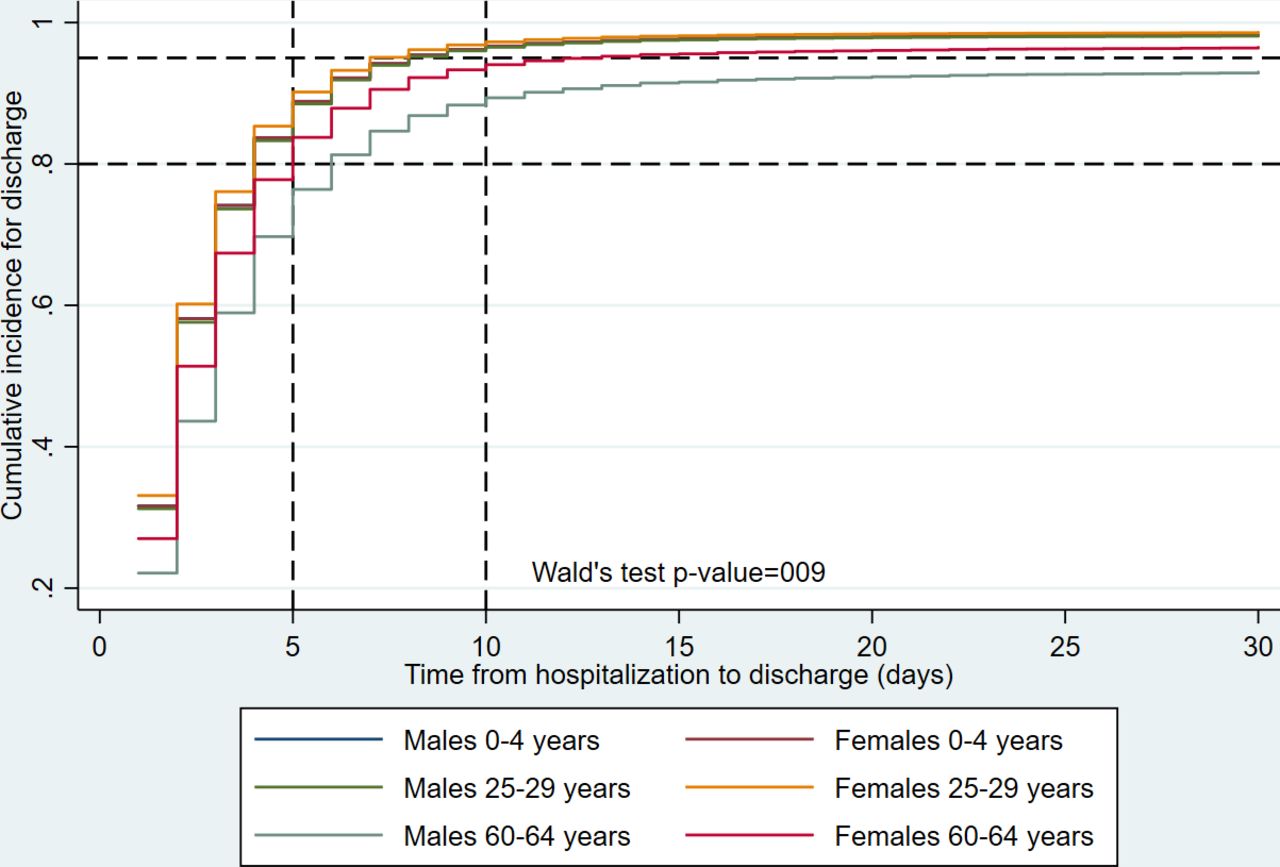
Figure 1 shows the cumulative incidence of discharge of asthmatics hospitalised in Ghana. The cumulative incidence of discharge was 90% for males aged 0–4 years by the fifth day, while it was 95% for females aged 25–29 years on the same day. However, the cumulative incidence of discharge was lower among females aged 60–64 years (75%) and males of the same age group (65%). These group differences in cumulative incidence for discharge were statistically significant (Wald test p=0.009).
{kind=link}
Cumulative incidence function curve of discharge of asthmatics hospitalised in Ghana from 2012 to 2017 by males 0–4 years vs females 0–4 years, males 25–29 years vs females 25–29 years and males 60–44 years vs females 60–64 years.
Sociodemographic factors associated with LoS
Results of the multivariable Cox regression descriptively showed earlier discharge for the years 2013 and 2014 and longer stays from 2015 to 2017 compared with 2012. Only hospitalisation stays in 2016 were significantly longer compared with the year 2012 (HR: 0.94 (0.90 to 0.98)). We also found age-dependent patterns of LoS with shorter stays for patients aged 50–54 years (HR: 1.02 (0.73 to 1.43)) and 15–19 years (HR: 1.49 (1.15 to 1.93)) compared patients aged 25–29 years. Patients aged 64 years and above spent significantly longer time in hospital (HR: 0.66 (0.46 to 0.94). In terms of the regions in which patients were admitted, the Ashanti (HR: 1.50 (1.23 to 1.84)), Northern (HR: 1.33 (1.07 to 1.66)), Upper West (HR: 2.09 (1.69 to 2.58)) and Western (HR: 1.32 (1.07 to 1.61)) regions were associated with early discharge after hospitalisation compared with the Greater Accra region. On the contrary, ownership of health insurance (HR: 0.92 (0.89 to 0.95)) and the presence of comorbidities (HR: 0.87 (0.85 to 0.89)) were associated with longer hospital stays. Patients with the educational attainment of secondary level or more were discharged earlier (HR: 1.08 (1.03 to 1.12)) compared with those without formal education (table 1). Climate seasons were not found to be associated with LoS. The HRs for interaction effects are summarised in online supplemental table 1.
Supplemental material
Discussion
We discuss results from a large nationwide retrospective study of 19 926 records on hospitalisations of patients with asthma and asthma exacerbation in Ghana between 2012 and 2017. We examined the temporal trends in LoS and its associated sociodemographic and health-related factors.
Our study reports a steady increase in the annual hospitalisation durations due to asthmatics mainly driven by very young children and female population growth. We found the age of the patient, educational attainment, occupational status, the outcome at discharge, region of admission and comorbidity of these asthmatics with or without exacerbation to differ by sex. The higher proportion of females hospitalised for asthma in our study is consistent with the global asthma distribution which is slightly dominated by females which mainly affects both men and women aged 35 years and above as previously reported by Bereza et al32 and Leynaert et al.33 Additionally, we found a trend of females being hospitalised more than males depending on whether it is the rainy or dry season.
The crude median LoS was 2 days (IQR: 1–3). In the CIF curve of discharge, accounting for patients who died during admission, nearly 90% of all patients were discharged by the seventh day of admission. Ninety-five per cent of patients less than 30 years were discharged by day 10. Overall, the cumulative incidence of discharge varied significantly by sex at age 0–4 years, 25–29 years and 60–64 years. This variation is not surprising as asthma manifests usually in young older people which might result in frequent hospital visits.
The multivariable Cox model for LoS showed a very wide range of times from admission to discharge depending on the age of the patient. Age groups 0–4 years, 5–9 years and 15–19 years had shorter LoS when compared with other patients aged 25–29 years. These age groups also accounted for the majority of asthma prevalence as previously reported in.5 13 32–34 On the contrary, the very old patients (80 years and above) stayed the longest during hospitalisation although this trend started from age 55 years. This association could be because patients of higher age are more prone to respiratory diseases and have longer recovery periods in general. This finding is supported by the finding of Aheto et al35 regarding patients in the 60–69 years age group’s independent association with asthma in Ghana according to their study. Although we found that all regions had an earlier discharge of patients with asthma compared with the Greater Accra region, the regions most strongly associated with early discharge were Ashanti, Northern, Upper West and Western regions. The earlier discharge noted in the Northern and Upper West regions could be an artificial effect due to the transfer of patients to other regions with well-resourced facilities, whereas those of the Ashanti and Western regions could be due to improved facilities in these regions. The inequitable distribution of health facilities and provision of care in these poor regions was earlier reported by the GDHS.25 Our finding regarding longer LoS due to the presence of comorbidities is comparable with other studies.20 36 37 As expected, young children hospitalised in the Upper West region having the longest hospital stay is not surprising as this region is one of the poorest in Ghana.25
Limitations
The main limitation of our study was the absence of unique identifiers to account for multiple hospital visits by the same patient. Nevertheless, since each episode of hospital admission requires completely new management of that episode, our conclusions remain valid irrespective of the possible multiple visits per patient. Finally, information on patient health history, type of diagnoses and the treatment received while on admission were not available for our study. However, all diagnoses were confirmed as required by the Ghana Health Service.
Conclusion
This is one of the largest studies on hospitalised asthmatics of all ages from a nationally representative cohort of patient episodes from 2012 to 2017 in Africa. One of the most relevant findings was that on average children less than 10 years tended to be discharged earlier, whereas older patients 60 years and above stayed longer compared with the age group 25–29 years. However, there were region-specific variations of LoS for this age groups. Although this study focused on hospitalisation records of asthmatics, the findings may well have a bearing on the burden of asthma among the general Ghanaian population resulting in estimated hospitalisation rates and associated risk factors in our study. Therefore, ensuring appropriate health systems, services and support for asthmatics should be a priority target for these children, the elderly and the most affected regions. Health facilities in these regions should be resourced as part of the mitigation process of averting longer LoS.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data used is published with this article.
Ethics statements
Patient consent for publication
Ethics approval
We received ethical approval from the Ghana Health Service Ethics Review Committee (GHS-ERC: 002/12/17) as part of the first author’s doctoral research.
Acknowledgments
The first author was supported by a scholarship of DAAD and the Government of Ghana, and the Mainzer Vereins zur Förderung der Epidemiologie, Biometrie, Informatik und der Krebsregister e.V. (VEBIK), but the views expressed in this paper are that of the authors. This paper is a part of the first author’s PhD dissertation. We acknowledge the Ghana Health Service for providing us with the patient data and the Ghana Statistical Service for also providing us with the population projections.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CTN and MB contributed to the study conception and design. CTN and AO helped with the acquisition of data. CTN, MA and JBD participated in the analysis and interpretation of data. CTN and JBD drafted the article and reviewed it while joining. AO, MB and DW in revising it critically for important intellectual content. DW supervised the analysis and interpretation of data and MB cosupervised the study. The final approval of the version to be published was agreed upon by all authors. CTN is acting as the
guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.