Article Text

Abstract
There have been a few reports of successful lung transplantation (LTx) in patients with SARS-CoV-2-induced acute respiratory distress syndrome (ARDS); however, all reports were with rather short follow-up. Here we present a 62-year-old man without prior lung diseases. Following SARS-CoV-2-induced ARDS and 6 months of extracorporeal membrane oxygenation, he underwent LTx. 3 months post-transplantation he developed acute hypoxia requiring emergency intubation. Chest imaging showed acute rejection, and de novo DQ8-DSA was discovered. He was treated with a high dose of corticosteroids and plasmapheresis and was extubated 4 days later, yet the de novo DQ8-DSA remained. After sessions of plasmapheresis and rituximab, the levels of de novo DQ8-DSA remained unchanged. Nine months post-transplantation the patient died of respiratory failure. We herein discuss the decision to transplant, the transplantation itself and the postoperative course with severe antibody-mediated rejection. In addition, we evaluated the histological changes of the explanted lungs and compared these with end-stage idiopathic pulmonary fibrosis tissue, where both similarities and differences are seen. With the current case experience, one might consider close monitoring regarding DSA, and gives further support that LTx should only be considered for very carefully selected patients.
- COVID-19
- lung transplantation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Despite major clinical advances in treating SARS-CoV-2-induced acute respiratory distress syndrome (ARDS), a large proportion of patients still experience severe and life-threatening conditions. Similar to ARDS, extracorporeal membrane oxygenation (ECMO) can be life-saving in patients with SARS-CoV-2-induced ARDS. Of these ECMO patients, a small proportion will progress to end-stage lung disease and ECMO weaning will not be possible. There have been reports of successful lung transplantation (LTx) in patients with SARS-CoV-2-induced end-stage lung disease, but with rather short follow-up and in most of the cases shorter time on ECMO support before transplantation.1–5 The worldwide experience with this matter is however limited and it is unknown if and when such a treatment should be offered.6 Given the poor long-term survival outcome in LTx, in combination with donor lung shortage and ethical questioning of graft allocation, all healing potentials need to be excluded before taking the decision to transplant.7
Case
Here we present a 62-year-old man with a history of diabetes mellitus, minor myocardial infarction with preserved ventricular function, with ejection fraction of >55% (documented using echocardiography 3 months before the SARS-CoV-2 infection), and without prior lung diseases. He presented to the emergency room with 7 days of dyspnoea, cough and fever and tested positive for SARS-CoV-2 at the time of admission. He received treatment with Veklury. Within 4 days he deteriorated and was transferred to the intensive care unit (ICU) and intubated. He was treated with lung protective ventilation and placed on prone position. On hospital day 17 he was placed on venovenous extracorporeal membrane oxygenation (VV-ECMO) and a percutaneous tracheostomy was also placed. At the time he was put on VV-ECMO support, he was SARS-CoV-2 negative. Despite aggressive supportive care, with repeated doses of both cortisone and dornase alfa, his condition progressed to end-stage lung disease along with the development of cor pulmonale. Interval chest imaging and CT scan revealed progressive lung disease (figure 1A). During 6 months of VV-ECMO support, the patient suffered numerous complications, including minor cerebral haemorrhage without neurological sequels, cor pulmonale and bloodstream infections. The ECMO cannulation strategy, femoral-jugular VV-ECMO, was kept during the entire treatment course. The patient suffered from being on mechanical ventilation and was therefore weaned off mechanical ventilation after 3 months and was spontaneously breathing while on VV-ECMO support.

{kind=link}
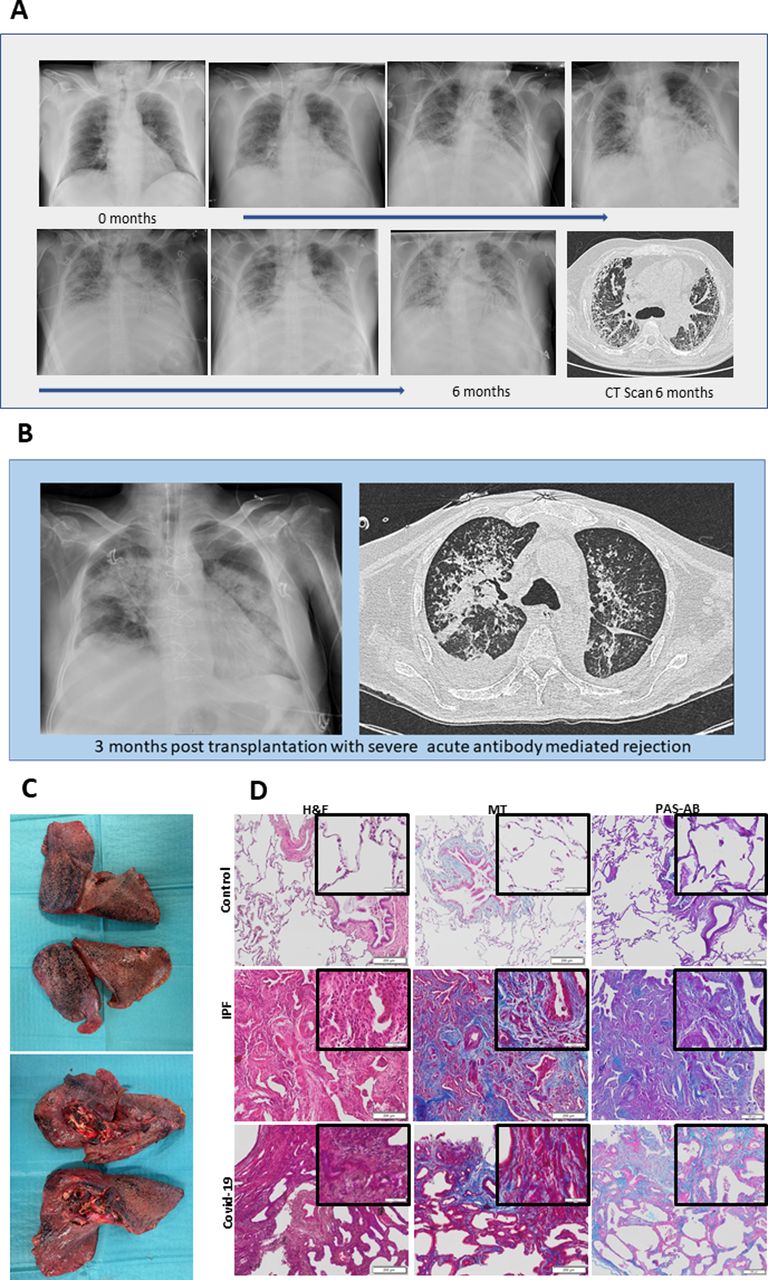
(A) Serial chest X-rays from time of presentation and diagnosis to just prior to transplantation (CT scan). Imaging displays progression of disease with increasing bilateral airspace opacities, diffuse consolidation and air bronchograms. (B) A chest X-ray and a CT scan 3 months post-transplantation with signs suspicious for acute rejection with ground-glass opacities, consolidation and interstitial thickening. (C) Gross images of explanted native lungs at the time of lung transplantation. Both lungs were small with cobblestoned visceral pleura. (D) All lungs were subjected to standard tissue processing followed by paraffin embedding. Sections from a healthy control (normal donor lung tissue), a patient with idiopathic pulmonary fibrosis (IPF) and from the current patient with COVID-19 (SARS-CoV-2-induced end-stage lung disease) were stained in parallel with H&E, Masson’s trichrome (MT), and periodic acid Schiff and Alcian blue (PAS-AB) and were compared.
Decision to transplant
The network within the European Cardio Thoracic Transplant Association, a part of the European Society for Organ Transplantation, was consulted prior to the decision to transplant. Given the relative contraindications for LTx, the decision for LTx was mainly based on the ethics with a neurologically intact, awake patient in combination with the lack of experience of LTx outcome in SARS-CoV-2-induced end-stage lung disease. At the time of transplantation, the patient was mobilised on a daily basis and was able to stand for a short while with a mobiliser and with extensive help from healthcare workers. He was communicable and was able to give consent for transplantation. At the time of transplantation the patient had a normal kidney function with Pt-eGFR of 83 mL/min/1.73 kvm. He had no pretransplant HLA antibodies. With regard to his heart function, echocardiography showed cor pulmonale with an HK/HF gradient of 63 mm Hg.
Surgical description
Suitable donor lungs, with a negative crossmatch, were allocated. With ongoing ECMO support, the patient underwent median sternotomy. No major signs of adherence between the chest wall and the lungs were seen and therefore central cannulation and conversion to cardiopulmonary bypass (CPB) were done. Hilar dissection was completed and the lungs were explanted. Donor lungs were then implanted in sequential standard fashion. The patient was separated from CPB, without the need to reinitiate ECMO support.
Postoperative course
The patient received standard triple immunosuppressive therapy with ciclosporin, prednisone and mycophenolate mofetil and induction therapy with antithymocyte globulin (ATG). The ATG was given as an infusion 8 hours post-transplantation at 1.5 mg/kg bodyweight (100 mg) in combination with hydrocortisone, clemastine and paracetamol according to local clinical guidelines. He had no signs of primary graft dysfunction and was extubated 3 days after the transplant. Post-transplant he suffered a long (2.5 months) postoperative course in the ICU with post-transplant heart failure related to cor pulmonale, infectious diseases and kidney insufficiency. He was treated with levosimendan, temporary haemodialysis and diverse types of antibiotics. He had stable levels of ciclosporin at 200–300 ng/mL and Mycophenolate mofetil (MMF) at 40–50 mg/L/hour, even during haemodialysis. At the time of transfer from the ICU to the ward, he was not dependent on oxygen support.
Acute antibody-mediated rejection
Three months post-transplantation, the patient without considerable prior signs shocked down at the hospital ward with acute hypoxia requiring emergency intubation and transfer back to the ICU. Chest imaging showed signs suspicious for acute rejection (figure 1B). De novo DQ8-DSA (mean fluorescence intensity 5000) was discovered. No C1q binding could be confirmed. He was successfully treated with a high dose of corticosteroids and plasmapheresis and was extubated 4 days later, yet the de novo DQ8-DSA remained. After 10 initial sessions of plasmapheresis, the levels of de novo DQ8-DSA remained unchanged. Immunosuppression was changed to tacrolimus and he received Intravenous immunoglobulin (IVIG) and corticosteroids. He received additional 10 sessions of plasmapheresis due to the refractory antibody-mediated rejection (AMR) and rituximab. To determine the nature of histological involvement, a transbronchial biopsy was done 6 months after transplantation and showed non-specific inflammation, scattered fibrosis deposits and 50% C4d positive staining. No transbronchial biopsy was done earlier due to the frailty of the patient and fear of complications. Eight months post-transplantation the patient’s level of de novo DQ8-DSA has increased despite aggressive therapy, which overlapped with a progressive decline in lung function. A spirometry was done 6 and 8 months post-transplantation and revealed VC of 1.7 (39% of expected) at 6 months and 1.2 (29% of expected) at 8 months, and FEV1 of 1.1 (predicted 3.3) at 6 months and 0.7 later at 8 months. Nine months after the transplant, the patient died of respiratory failure. Given the family’s request no autopsy was done.
Histology findings
Gross morphology of the explanted lungs is shown in figure 1C. The explanted lungs were fixed within 1 hour and subsequently processed for routine histology. Similar to other recent reports, we observed noticeable interstitial fibrosis in the distal lung tissue of the explanted COVID-19 lungs (figure 1D). However, unlike other recent histological reports,1 we did not observe significant infiltration of immune cells in the airspaces, major evidence of diffuse alveolar damage or signs of organising pneumonia. This is likely due to the fact that the patient was beyond the acute phase of the disease and was not known to have any secondary pulmonary infection around the time of transplantation, as reported in the previous cases. The histological changes observed in the distal regions of the present COVID-19 explanted tissue had both histological similarities and differences to end-stage idiopathic pulmonary fibrosis (IPF) tissue. Parenchymal remodelling in IPF is characterised by interstitial fibrosis from mostly collagenous protein deposition, as well as deposition of both Alcian blue (AB) (acidic) and periodic acid Schiff (PAS+) (neutral) mucopolysaccharides (eg, mucins and glycoproteins) in fibroblastic foci. In contrast, alveolar thickening in this patient with COVID-19 was characterised by deposition of both collagenous and non-collagenous proteins and a pronounced increase of mostly AB positive staining.8 9 Interestingly, we observed little to no evidence of PAS+ staining in the distal lung, but the proximal lung tissue processed at the same time from this patient did contain both AB and PAS+ staining (data not shown), suggesting that alterations in mucopolysaccharides occurred in the distal lung only. We also observed evidence of abnormal epithelial repair with the appearance of honeycomb cysts lined with cuboidal epithelial cells, similar to what is observed in IPF. Taken together, this indicates that the patient did not have significant ongoing inflammation in the airspaces at the time of transplantation, but that the lung had undergone dysregulated repair resulting in significant interstitial fibrosis and aberrant re-epithelialisation (figure 1D).
Conclusions
LTx is feasible for SARS-CoV-2-induced end-stage lung disease; however, long-term results are unknown. Knowledge will increase with increasing number of patients transplanted and longer follow-up data. Only then we will know if these patients are more predisposed to AMR, and if so if it is caused by the long preoperative ECMO support or it is the systemic inflammatory response induced by COVID-19 itself. With the current case experience, one might consider close monitoring regarding DSA, and gives further support that LTx should only be considered for very carefully selected patients. The explanted lungs of this patient demonstrated some of the stereotypical histological changes seen in patients with IPF, including collagen deposition and honeycombing. Whether or not currently approved antifibrotic therapies could be used in these patients to slow down disease progression remains unknown but will be important to explore in the future.10
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors contributed to the study design and acquisition of data. SL, EG, HL, PE, IS, DW and RG contributed to the analysis and interpretation of data and drafted the manuscript. All authors read and approved the final manuscript.
Funding This work was supported by Knut and Alice Wallenberg (2018SLDEW) and Marcus Wallenberg Foundation (2018SL).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.