Article Text

Abstract
Introduction Obstructive lung diseases (asthma and chronic obstructive pulmonary disease (COPD)) and smoking are associated with greater risk of respiratory infections and hospitalisations, but conflicting data exist regarding their association with severity of COVID-19, and few studies have evaluated whether these associations differ by age.
Objectives To examine the associations between asthma, COPD and smoking on the severity of COVID-19 among a cohort of hospitalised patients, and to test for effect modification by age.
Methods We performed a retrospective analysis of electronic health record data of patients admitted to Massachusetts General Hospital, assigning the maximal WHO Clinical Progression Scale score for each patient during the first 28 days following hospital admission. Using ordered logistic regression, we measured the association between maximal severity score and asthma, COPD and smoking and their interaction with age.
Measurements and main results Among 1391 patients hospitalised with COVID-19, we found an increased risk of severe disease among patients with COPD and prior smoking, independent of age. We also found evidence of effect modification by age with asthma and current smoking; in particular, asthma was associated with decreased COVID-19 severity among older adults, and current smoking was associated with decreased severity among younger patients.
Conclusions This cohort study identifies age as a modifying factor for the association between asthma and smoking on severity of COVID-19. Our findings highlight the complexities of determining risk factors for COVID-19 severity, and suggest that the effect of risk factors may vary across the age spectrum.
- COPD epidemiology
- tobacco and the lung
- viral infection
- asthma epidemiology
Data availability statement
Data are available upon reasonable request. Data requests will be reviewed by the MGH COVID Registry.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
How does age affect the severity of COVID-19 in patients with a history of obstructive lung disease and smoking?
Asthma is associated with decreased COVID-19 severity among older adults, and current smoking is associated with decreased severity among younger patients.
To our knowledge, this is the first study to specifically examine how age might affect the relationship between the most common lung diseases, smoking and COVID-19 severity. Our findings suggest that the effect of commonly identified risk factors may vary across the age spectrum.
Introduction
The majority of severe COVID-19 and COVID-19-related deaths occur among those with comorbidities, including those with chronic respiratory disease.1 2 The United States Center for Disease Control and Prevention currently classifies chronic obstructive pulmonary disease (COPD, moderate-to-severe asthma and current and former smoking as associated with increased risk of severe COVID-19 complications.3 4 Though the majority of deaths due to COVID-19 occur among older adults, chronic respiratory diseases may increase the risk of severe outcomes even among younger patients. In the spring 2020 surge, chronic respiratory diseases were present in 20.9% of people under age 65 who died of COVID-19 in the USA through 18 May 2020,5 and a large study in the UK found that 20.9% of patients aged 16–49 and 44.4% of those aged 50–69 hospitalised with COVID-19 were diagnosed with asthma.6 By contrast, in a large cohort of hospitalised patients with COVID-19 in China, only 2.8% of patients had chronic respiratory disease.7
Since viruses (including non-SARS coronaviruses) are associated with both asthma and COPD exacerbations,8 9 patients with either obstructive lung disease would be expected to have a higher rate of severe outcomes due to COVID-19. Despite initial reports of low prevalence of asthma among patients hospitalised with COVID-19 in China,10 investigators have reported prolonged intubation course among asthmatics,11 increased risk of death among asthmatics with recent oral corticosteroid use,2 and worse clinical outcomes, especially among those with non-allergic asthma.12 Multiple studies have also reported increased risk of death among patients with COPD, with an even greater risk among men.13
Smoking increases the risk of acquiring respiratory infections14 15 by impairing macrophage and cytokine responses and upregulating pathogen receptors.16–20 It is the primary risk factor for developing COPD, and contributes to development and exacerbations of asthma.21–24 Smoking is also associated with upregulation of the ACE-2 receptor in airways, raising concerns early in the pandemic regarding increased entry of SARS-CoV-2 into host cells.25–28 An initial report from patients in Wuhan in December/January 2019 noted that patients with a history of smoking had significantly increased odds of disease progression,29 but subsequent meta-analyses have reported lower-than-expected prevalence of smoking among hospitalised patients with COVID-19.30 31
To better understand the relative contributions of obstructive lung disease and smoking on the severity of COVID-19 across the age spectrum, we analysed data from the first 1391 patients admitted to Massachusetts General Hospital (MGH) with COVID-19. We hypothesised that obstructive lung diseases and smoking would be associated with severe COVID-19 disease, and that these associations would be greater among older patients.
Methods
Study design and data sources
We performed a retrospective analysis of electronic health record data of patients admitted to MGH between 11 March and 3 June 2020. Demographic, hospitalisation, laboratory and body mass index (BMI) data were extracted from the MGH Enterprise Data Warehouse using structured query language procedures. Clinical data, including medical history, treatments in the hospital and outcomes were manually abstracted by trained chart reviewers and entered into a Redcap (Research Electronic Data Capture) database hosted on a MassGeneral Brigham server.32
Population
We included all patients in the MGH COVID-19 Registry, a cohort of children and adults with positive SARS-CoV-2 PCR testing who were inpatients during the study period and had 28-day outcome data available at the time of the analysis.33 The inclusion criteria for the cohort were (1) any positive SARS-CoV-2 PCR test, infection flag that indicates COVID-19 infection, or ICD-10 diagnosis of U07.1, and (2) at least one hospitalisation at MGH with an admission date within 45 days after criterion (1). Patients who did not satisfy these criteria were excluded.
Variable definitions
Demographic data and medical history (including prior diagnoses of asthma and COPD) were obtained from the health record. BMI was calculated from height and weight measured within ±14 days of hospitalisation. We used results of laboratory testing closest to the time of admission to the hospital.
The primary outcome used for this analysis is the WHO Clinical Progression Scale (WHO CPS), which was developed to measure the full range of disease severity and progression in COVID-19 disease.34 While the scale as created ranges from 0 (uninfected) to 10 (dead), our analysis focuses on severity of illness among hospitalised patients and therefore only includes WHO CPS scores 4 and higher (moderate and severe disease, see table 1). We calculated the maximal WHO CPS for each patient during the first 28 days following hospital admission using the highest oxygen flow rate, fraction of inspired oxygen (FiO2), or mode of ventilatory support; and the presence of haemodialysis, vasopressor or extracorporeal membrane oxygenation (ECMO) use reported in the registry. Because concurrent arterial partial pressure of oxygen (PaO2), arterial oxyhaemoglobin saturation (SpO2) and FiO2 data were not consistently available in the registry, we approximated the minimum SpO2/FiO2 ratio35 by using the maximal reported FiO2 and assuming an SpO2 of 90% based on the target SpO2 in the hospital’s standard mechanical ventilation order set and usual target for oxygen supplementation.
WHO CPS among hospitalised patients
Statistical/analytic methods
After calculating descriptive statistics for major variables of interest, we measured the unadjusted association between potential predictors of disease severity (including the CDC underlying conditions on which data were available) and the WHO CPS using ordered logistic regression. We then constructed a multivariable model that included the variables of interest as well as demographic variables and cardiometabolic comorbidities. We also tested for effect modification creating two-way interaction terms between age and asthma, age and COPD and age and smoking. We estimated predicted probabilities of each WHO CPS level across age, at the mean level of each covariate, using the Stata margins and marginsplot commands. Standard errors and 95% CI were calculated using the delta method.36 37 Finally, we compared biomarkers of disease severity and host response between patients with and without asthma, between patients with and without COPD and among patients with varying exposures to smoking, using Wilcoxon rank-sum and Kruskal-Wallis tests as appropriate. All analyses were performed in Stata V.16.1 (StataCorp, College Station, Texas, USA).
Human subjects approval
The MGH COVID-19 registry was reviewed and approved by the MassGeneral Brigham Human Research Committee (#2020P000829). The present analysis was reviewed and determined to be exempt.
Patient and public involvement
Patients were not directly involved in the design of this data analysis, though the question of how obstructive lung diseases and smoking affect COVID-19 outcomes was raised by many of our patients and their families.
Results
We analysed data from 1391 patients who were hospitalised with COVID-19 and had complete 28-day outcome data. Baseline characteristics of the study population are summarised in the first column of table 2. Patients ranged in age from newborn to 99 years (mean age: 59 years), were predominantly men (57%), and were primarily white or Hispanic. The majority (78%) of patients were overweight or obese and 76% had a cardiac or metabolic disorder. Among all admitted patients, 22% (301/1391) had a prior diagnosis of obstructive lung disease: asthma (158/1391), COPD (119/1391) or both (24/1391). The majority of patients were either never (55.9%) or previous smokers (29.0%); 102 (7%)/1391 reported currently smoking. Six (0.4%) patients reported current use of electronic nicotine delivery systems. Inhaled corticosteroid use was common among both patients with asthma (40.1%) and COPD (43.4%).
Demographic and clinical characteristics by WHO Clinical Progression Score
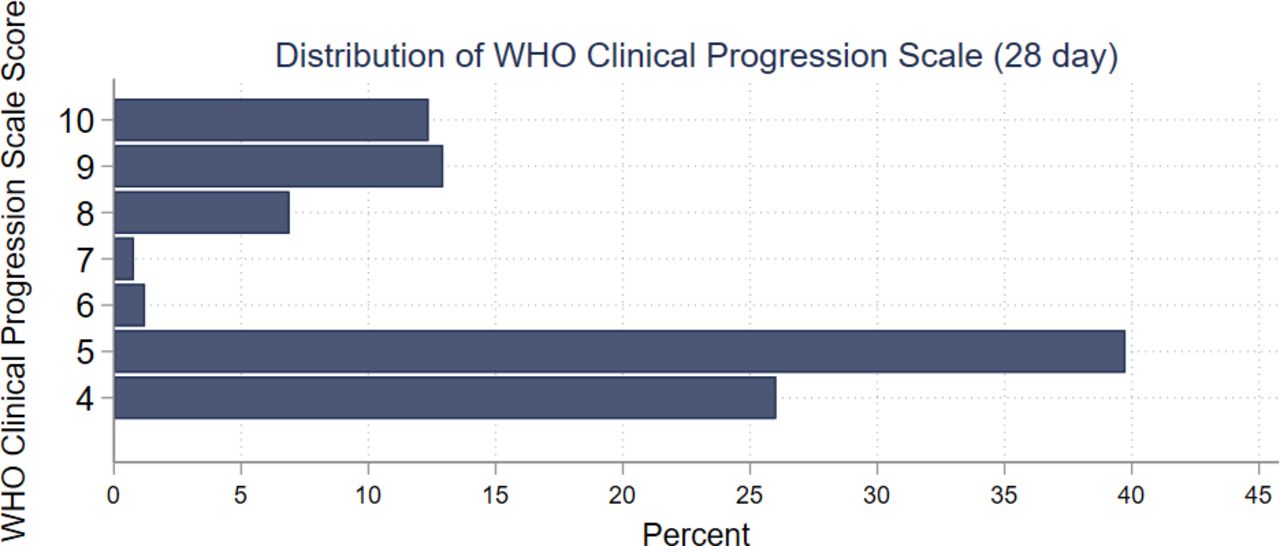
Figure 1 demonstrates the distribution of the WHO CPS among the study population. Most patients (74%) required oxygen or other ventilator support during hospitalisation, and 12% died during the 28-day period of data review. The majority (69%) of patients were treated on hospital floors; 31% were admitted an intensive care unit (ICU) during their hospitalisation. On univariate analysis (table 2), we found a strong positive association between WHO CPS score and age, male sex, BMI, previous smoking, COPD, coronary artery disease (CAD), heart failure, hypertension, diabetes and chronic kidney disease. We found a negative unadjusted association between WHO CPS score and Hispanic ethnicity, asthma and current smoking. We did not find any significant association between WHO CPS score and prior use of inhaled bronchodilator medications, inhaled corticosteroids or montelukast.
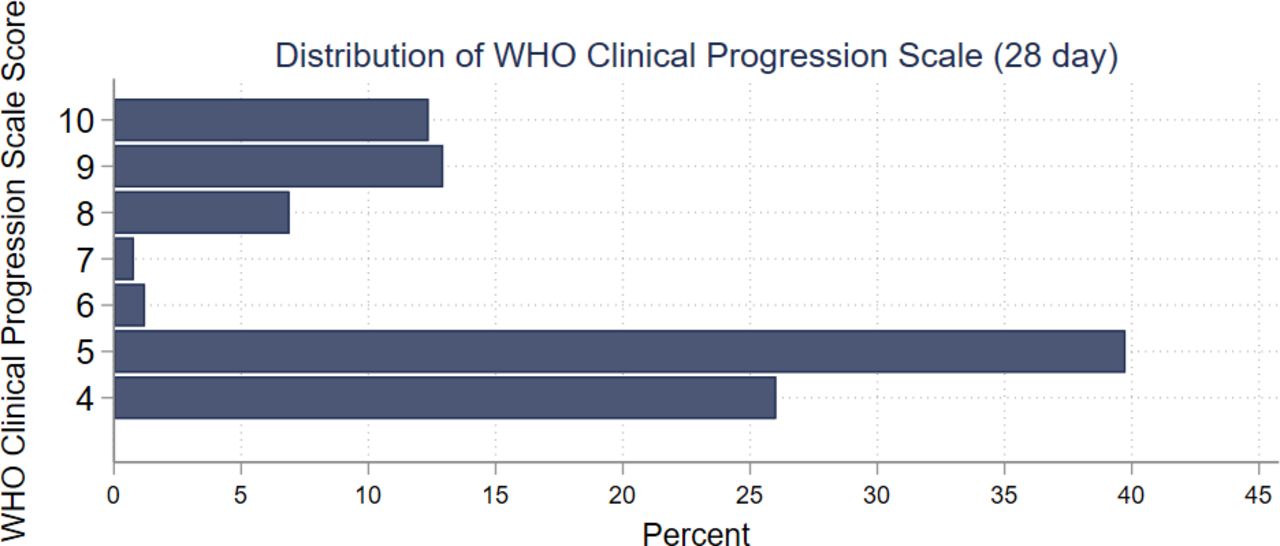
Distribution of WHO clinical progression scale.
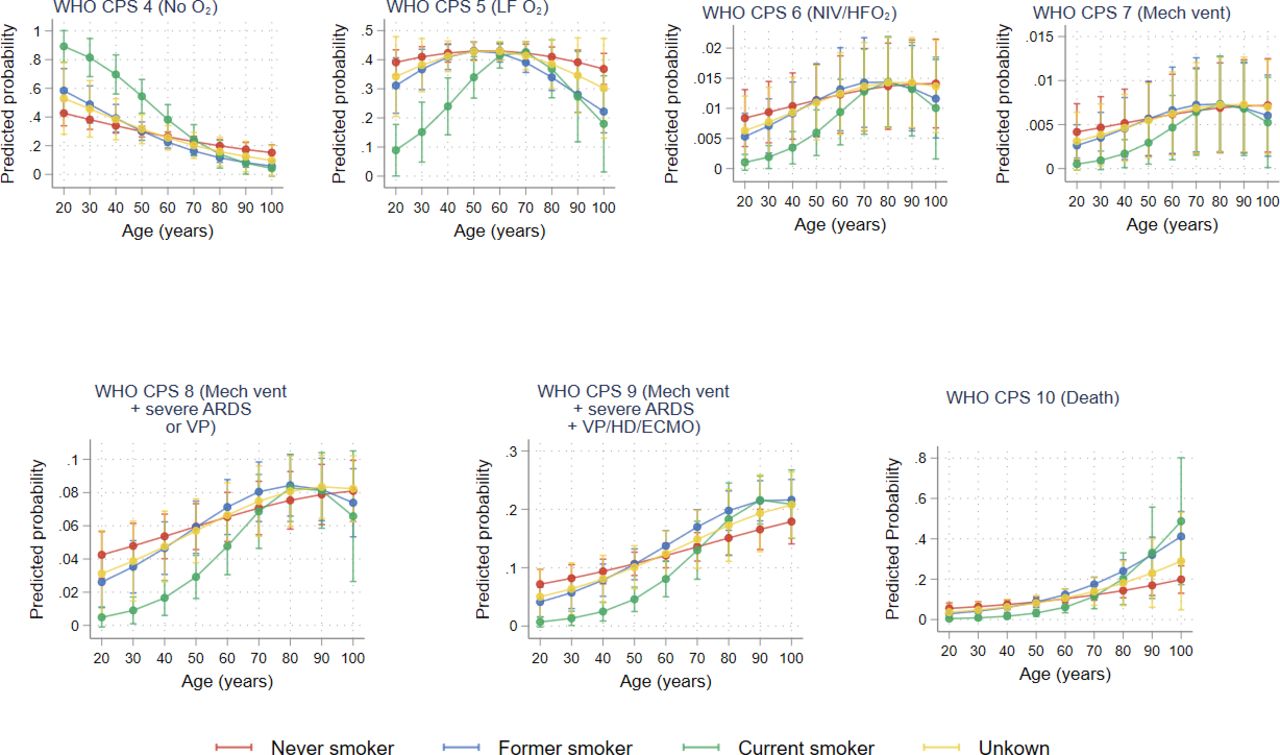
We then estimated the association between asthma, COPD and smoking status with WHO CPS score in a multivariable model adjusting for relevant demographic and comorbidity covariates and interaction terms by age for the three risk factors of interest (online supplemental table 1). We found that a history of asthma was associated with an increased risk of requiring oxygen among younger patients and a reduced risk of severe disease among older patients (figure 2, pinteraction=0.006), that no significant effect modification was observed by age with COPD (figure 3, pinteraction=0.61), and that current smoking was associated with a reduced risk of severe disease among younger patients but not among older patients (figure 4, pinteraction=0.002). The effect of asthma on WHO CPS ranged from OR 1.51 (95% CI: 0.76 to 2.99) at age 20 to OR 0.44 (95% CI: 0.26 to 0.74) at age 80, and the effect of smoking ranged from OR 0.07 (95% CI: 0.02 to 0.26) at age 20 to OR 0.375 (95% CI: 0.66 to 3.59) at age 80 (see table 3). Other significant covariates in the multivariable model included age (OR: 1.02 (95% CI: 1.01 to 1.03)), female sex (OR: 0.71 (95% CI: 0.55 to 0.90)), BMI (OR: 1.06 (95%: 1.04 to 1.08)) and diabetes (OR: 1.37 (95% CI: 1.05 to 1.79)).
Supplemental material
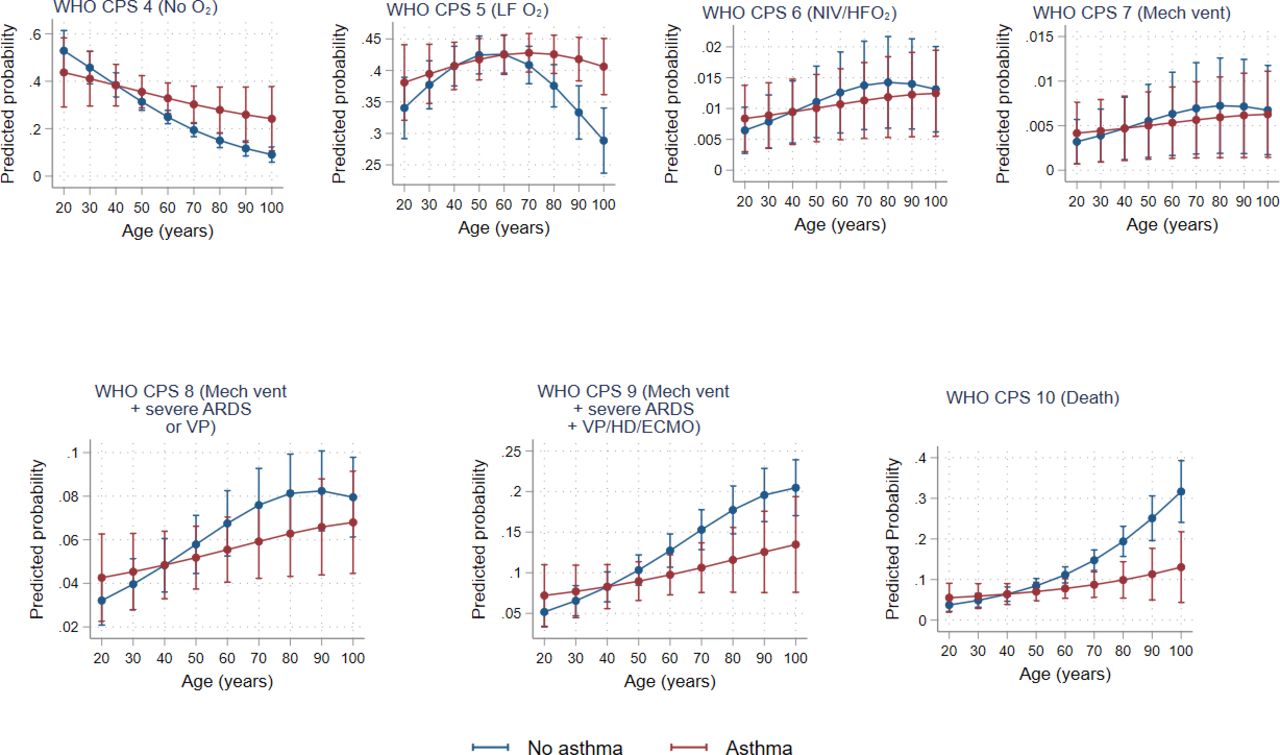
Predicted probability of WHO CPS score levels by age and asthma. ARDS, acute respiratory distress syndrome; ECMO, extracorporeal membrane oxygenation; HD, hemodialysis; VP, vasopressors; WHO CPS, WHO Clinical Progression Scale.
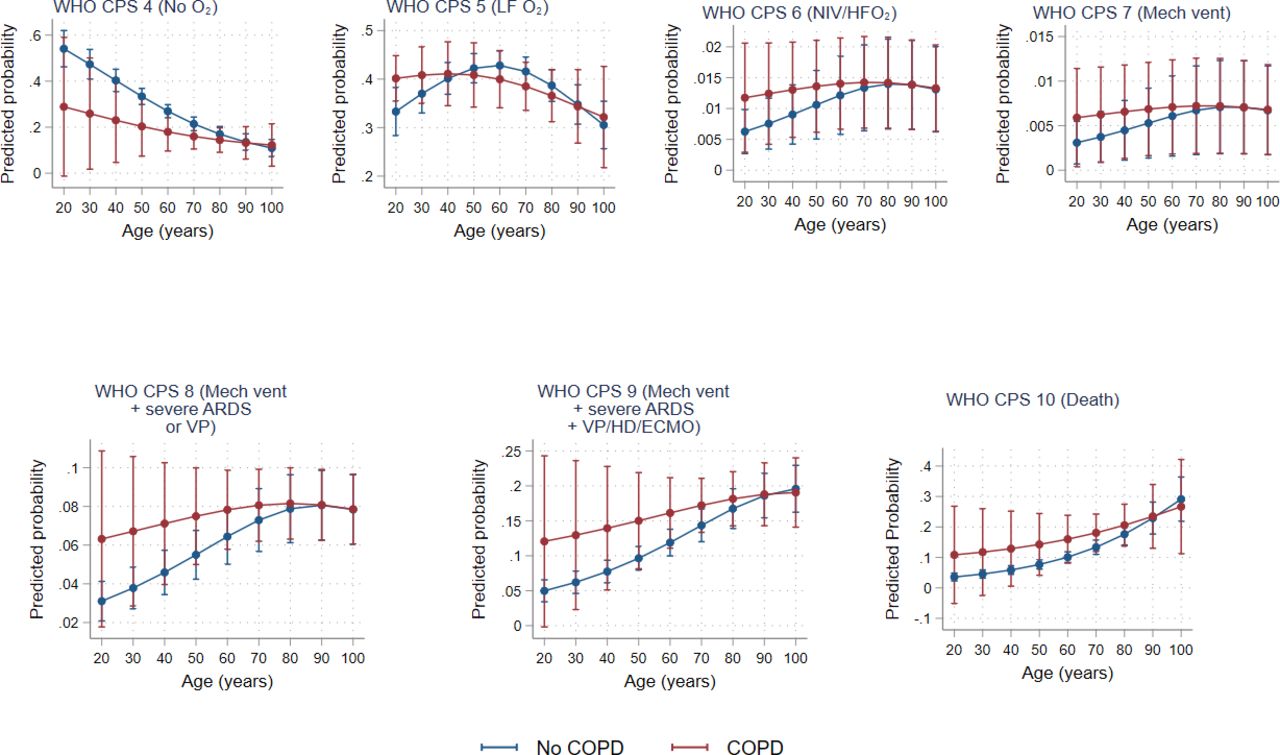
Predicted probability of WHO CPS score levels by age and COPD. COPD, chronic obstructive pulmonary disease; ARDS, acute respiratory distress syndrome; VP, vasopressors; HD, hemodialysis; ECMO, extracorporeal membrane oxygenation; WHO CPS, WHO Clinical Progression Scale.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted probability of WHO CPS score levels by age and smoking status. ARDS, acute respiratory distress syndrome; VP, vasopressors; HD, hemodialysis; ECMO, extracorporeal membrane oxygenation; WHO CPS, WHO Clinical Progression Scale.
OR for WHO CPS score for asthma, COPD and smoking across levels of age
To further characterise the effects of asthma, COPD and smoking on the host response to SARS-CoV-2 infection, we compared laboratory testing at the time of hospital admission between patients with and without asthma, between patients with and without COPD and among patients across categories of smoking history (table 4). We observed an increased absolute lymphocyte count and reduced levels of inflammatory markers (ferritin, CRP, ESR and procalcitonin) among patients with asthma and among patients who reported currently smoking. Patients with COPD also had reduced levels of inflammatory markers but increased markers of cardiovascular stress (troponin, D-dimer and NT-proBNP).
Laboratory test values at the time of admission
Discussion
In this cohort of 1391 hospitalised patients with COVID-19, we found evidence of significant effect modification of the association between asthma, smoking and COVID-19 severity by age. In particular, we found that asthma was associated with decreased COVID-19 severity among older patients, and that current smoking was associated with decreased severity among younger patients. We found an increased risk of severe disease among patients with COPD and prior smoking, independent of age. We also noted differences in inflammatory biomarkers between patients with and without asthma and across smoking statuses. We did not find any evidence of association between use of bronchodilators, inhaled corticosteroids or montelukast prior to hospitalisation and COVID-19 severity.
Our findings extend prior studies that have evaluated the relationship between obstructive lung diseases, smoking and COVID-19 outcomes. While other studies have reported associations between both asthma and COPD and severe COVID-19,6 7 to our knowledge this is the first analysis to specifically test for and identify effect modification by age. Our analysis may explain the variability of reports of the effects of asthma and smoking on COVID-19 severity. These findings raise the possibility of subgroup-specific effects of these risk factors and suggest that generalised statements regarding increased risk may be incomplete.
Several studies have suggested that asthma may be protective in some patients, including a Chicago study of 1003 patients with COVID-19 that reported lower rate of ARDS and death among those with asthma,11 and an analysis of a smaller cohort of patients with COVID-19 at our hospital that found a lower risk of ICU admission among those with asthma but no significant difference in risk of death compared with control patients without asthma.38 Two recent meta-analyses confirmed the lack of an association between presence of asthma and mortality,39 40 but two large studies in Korea and the UK reported that while asthma in general was not a risk factor for disease severity, asthma exacerbation within the past year was associated with an increased risk for death.2 41
The mechanism of the observed protective effect of asthma is unclear, and may be in part related to increased care seeking or a lower threshold for hospitalisation among patients with asthma. For example, patients with asthma may be more likely to be hospitalised for milder symptoms and therefore have lower WHO CPS scores. The effect of asthma on the severity of COVID-19 disease may likely be also determined by the underlying asthma phenotype and immunology of the host.42 Several investigators have postulated that the allergic phenotype may increase the risk of viral infection43 but may decrease the risk of the hyperimmune response that characterises severe disease.44 45 The severe asthma phenotype that is associated with worse COVID-19 outcomes may vary by atopy, age of onset, race/ethnicity and obesity.46 Obesity is associated with more severe and non-allergic asthma, through mechanisms that include altered pulmonary mechanics, adipokine changes, Th-1 and ILinterleukin-17-related airway inflammation,47–49 and our analysis confirmed the previously reported association between obesity and COVID-19 severity.50–52
The observed inverse correlation between current smoking status and COVID-19 severity adds to the existing literature regarding the association between current smoking and risk of SARS-CoV-2 infection, disease severity and mortality.53–57 Our findings contrast with observations from other common respiratory pathogens, including Middle East Respiratory Syndrome, in which smoking has been associated with increased risk of both infection and mortality,58 59 influenza, in which history of smoking is associated with increased risk of hospital admission,60 and respiratory syncytial virus, in which maternal smoking is associated with increased risk of acute lower respiratory infection in children.61 Compared with former smokers and never smokers, current smoking is associated with an increased risk of death from pneumococcal pneumonia.62
Postulated mechanisms for a protective effect of current smoking include an inhibitory effect of nicotine on the production of proinflammatory cytokines and increased tolerance of airway or lung injury among current smokers.63–65 The clinical relevance of these hypotheses cannot be fully tested without accounting for potential confounders, including differences in behaviours leading to SARS-CoV-2 exposure, differences in thresholds for seeking testing, and access to healthcare. While we found evidence of age-specific effects of smoking, it is likely that the effects of smoking are also modified by other host factors that we did not examine, including amount of smoking, type of smoking, race/ethnicity and genetics.
Our study does not address several important questions relating to the effects of obstructive lung disease and smoking on COVID-19 outcomes. First, our cohort is limited to inpatients with COVID-19 and is therefore unable to assess the effect of these risk factors on becoming infected with SARS-CoV-2 or developing mild disease. The small number of children included in the sample (n=16), all of whom were non-smokers, also limits our ability to draw conclusions about children. Second, because the WHO CPS focuses on supportive measures provided during hospitalisation, decisions to forgo life-sustaining treatment including mechanical ventilation, vasopressor support or renal replacement therapy may bias the score downward for some severely ill patients.34 Because of institutional infection control practice patterns, few patients were treated with high-flow oxygen or non-invasive ventilation (WHO CPS 6), and most patients with cute respiratory distress syndrome (ARDS) ultimately developed either severe ARDS or required vasopressors (WHO CPS 8 or higher), which limits our ability to draw conclusions regarding WHO CPS scores 6 and 7. Third, our analysis relies on accurate reporting and abstraction of data from the medical record; these data may inaccurate or incomplete, especially for patients who did not previously receive their care within the MassGeneral Brigham system. Finally, the presence or absence of obstructive lung disease was determined based on diagnoses present during chart review, which is subject to underdiagnosis, overdiagnosis and misdiagnosis.66 67 In addition, we were unable to characterise or stratify by severity of obstructive lung disease or duration and amount of smoking, which may affect the severity of COVID-19. Further studies are required to evaluate these factors and to test for other potential effect modifiers, including asthma phenotype, the nature of inflammatory responses, and the effects of asthma/COPD treatment. In addition, future studies should examine the effects of these risk factors on the long-term sequelae of COVID-19.
Conclusion
In summary, this study identifies age as a modifying factor for the association between asthma and smoking on severity of COVID-19. Our findings highlight the complexities of determining risk factors for COVID-19 severity, and suggest that predicting disease severity based on single risk factors may not be appropriate.
Data availability statement
Data are available upon reasonable request. Data requests will be reviewed by the MGH COVID Registry.
Ethics statements
Patient consent for publication
Acknowledgments
The authors wish to thank the dedicated manual chart reviewers and data managers for their efforts in creating the MGH COVID-19 Registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Drafting of the manuscript and statistical analysis was done by PPM, who is also guarantor of the study. Conception and design was done by PPM, DH, and TBK. Acquisition of the data was done by VAT, ASF, IB and ML. Critical revision of the manuscript for important intellectual content was performed by ML, DH, LMY, JL, ET, AAB, VAT, ASF, IVB, PLH and TBK.
Funding The authors report the following funding sources: The National Institutes of Health: K23ES030399-03 (PPM), R37AI058736-16S1 (IVB), 5K08HL143183 (LY); Weissman Family MGH Research Scholar (IB); the Cystic Fibrosis Foundation (YONKER18Q0 to LMY); and R01HL132786 and R01AG062393 (VAT). This work was conducted with support from Harvard Catalyst, The Harvard Clinical and Translational Science Center (National Center for Advancing Translational Sciences, National Institutes of Health Award UL 1TR002541) and financial contributions from Harvard University and its affiliated academic healthcare centers. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University and its affiliated academic healthcare centers, or the National Institutes of Health.
Competing interests Dr Moschovis is a member of an adjudication committee for Pfizer.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.