Article Text

Abstract
Introduction COVID-19 pandemic has had a huge impact on global health to date, with 5.6 million cases in the UK since its emergence. The respiratory symptoms largely mimic those of pneumonia’ with symptoms ranging from mild to severe. The effects on respiratory physiology are not yet fully understood, but evidence is emerging that there is much dysfunctional breathing reported but little information on tidal ventilation from the acute phase of the infection. Structured light plethysmography (SLP) is a contactless technique of respiratory function testing that measures tidal breathing parameters by assessing thoracoabdominal displacement.
Methods In a postdischarge clinic, SLP was performed routinely on 110 hospitalised patients recovering from COVID-19 who had been screened for respiratory symptoms to confirm any respiratory changes occurring after the disease. Patients were categorised based on their hospital treatment in (1) the intensive therapy unit (ITU) (requiring intubation) (n=65) or (2) respiratory wards only (n=45). Data from these two patient cohorts were compared with preacquired data from healthy controls (n=30).
Results We have found a significantly increased respiratory rate (p=0.006) in ITU patients compared with the healthy cohort and also a significant decrease in the inspiratory time (p=0.01), expiratory time (p=0.005) and the total breathing cycle (p=0.008). There were no significant differences between ITU and ward patients and no significant differences in healthy compared with ward patients. We examined the variability of breathing (‘entropy’) both in terms of the breath-to-breath interval and the volume-to-volume change. The breath-to-breath interval alone was significantly lower in ITU patients compared with healthy cohorts (p=0.02).
Conclusion Our findings suggest that abnormalities in tidal breathing can be detected in COVID-19 recovery patients, and SLP may be a promising tool in assessing the aftermath of diseases such as COVID-19, particularly if more intensive management strategies such as mechanical ventilation are required.
- respiratory measurement
- COVID-19
- ARDS
- lung physiology
Data availability statement
Data are available upon reasonable request. The data for the study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
We know that patients who have had COVID-19 can have abnormal lung function, and we wanted to examine whether there were abnormal breathing patterns in patients who had been in hospital and recovered from COVID-19, but after 3 months had persisting respiratory symptoms. We wanted to see whether patients treated on wards had different breathing abnormalities compared with those who had recovered from having more severe disease and had been intubated and mechanically ventilated for long periods in intensive therapy unit (ITU). Furthermore, we wanted to see whether detecting abnormal breathing patterns in patients with COVID-19 could be a useful method to screen those with COVID-19 respiratory impairment.
Although we have not found any significant differences in breathing patterns between ITU and ward patients, but when compared with healthy subjects, ITU patients had a significantly higher respiratory rate and a lower inspiratory time, expiratory time and total cycle of the breath. This could be a result of either severity of the disease or the subsequent effect of mechanical ventilation and different management approaches.
We sought to investigate what changes could be detected and perhaps act as a surrogate or screening test for further lung function testing using structured light plethysmography and if a novel wave analysis of the tidal breathing trace could be used to detect an abnormality.
Introduction
The novel COVID-19 or SARS-CoV2 belongs to the family of single-stranded RNA viruses that include the previously identified Middle East Respiratory Syndrome virus and SARS-CoV.1 2 Important differences with SARS-CoV2 include the higher capacity of the virus to spread by aerosolisation and the mutations rate, which lead to infecting over 183 million people globally, with 49 million in the UK alone.3 4
The angiotensin-converting enzyme 2 receptor appears to be the primary route of infection in the lungs,1 5 and expression in other tissues may help to explain some of the systemic effects of infection.6 Infiltration results in pathophysiological complications such as shortness of breath, coughing and, subsequently, an acute respiratory distress syndrome (ARDS), pneumonia and acute respiratory failure, which is commonly seen in severe cases that require complex ventilatory support.7 8 Breathing may be altered in patients with post-COVID-19, either as a result of the infection, intensive therapy or sepsis. Thus, it is essential to assess respiratory functionality as part of the recovery process and patient management.
Respiratory function testing (RFT) is a vital tool to assess the functionality of breathing and identify physiological abnormalities and defects. There are many tests available, but spirometry RFT is the most common and usually the first-line test; however, spirometry is a volitional, highly effort-dependent test and may not be achievable by all patients’ groups. In our study, we used structured light plethysmography (SLP), which is a novel optophysiological RFT technique to measure breathing patterns. The working principle is based on the recording of the thoracoabdominal (TA) displacement by motion capture. The device projects a chessboard-like grid of light onto the anterior trunk, and two cameras record movement and then generate a three-dimensional image of the chest and the abdomen.9 10 It is non-invasive, contactless, self-calibrating and easy to perform, requiring only quiet tidal breathing. SLP produces many parameters associated with the tidal ventilation trace and TA contribution and synchronicity. SLP viability and use have previously been investigated in young patients with asthma recovering from exacerbations,11 12 patients with chronic obstructive pulmonary disease (COPD) 13 and children diagnosed with neuromuscular disorders such as Duchenne Muscular Dystrophy.14 In addition to the commonly used respiratory parameters, we have also investigated the variability or ‘entropy’ of breathing using waveform analysis. The simple quantification of entropy has been a targeted method to assess the differences or fluctuations in breathing15–17 and could potentially provide valuable insight into dysfunctional breathing that may present in our patients with post-COVID-19.
We have used SLP to determine whether there are any detectable differences in breathing patterns in a cohort of patients previously described18 recovering from COVID-19 and whether these are related to the severity of disease determined by whether the patients were admitted to intensive therapy unit (ITU) and ventilated or remained on respiratory wards.
Methods
Study participants
Between 16 June and 30 November 2020, at least 3 months after hospital discharge, 110 COVID-19 recovery patients attended an outpatient RFT appointment at the University Hospitals Birmingham NHS Foundation Trust, UK. All patients had SLP measurements made as part of their physiological assessment with other techniques and devices with work and protocol published elsewhere.19 SLP data from healthy subjects were recorded prior to the COVID-19 pandemic and retrieved retrospectively.
Patients were grouped according to their admission and symptoms. Ward cohort was patients with mild to moderate cases admitted to the medical wards, required supplemental oxygen (FiO2 >40%) but did not need invasive mechanical ventilation. ITU cohort was patients with severe symptoms who were admitted to the ITU and were sedated, intubated and ventilated as part of their treatment.
Underlying chronic conditions such as diabetes, respiratory disorders, cardiac disorders were not noted for the purposes of this study. The exclusion criteria used were (1) the inability to perform an interpretable SLP test or (2) patients who were not admitted to either ITU or wards.
Study device and process
SLP measurements were all recorded using the Thora-3Di device (Pneumacare, Ely, UK). While the procedure was explained to the patient before each recording, they were seated and able to relax in order to mitigate any prior exercise changes or activity. A tight-fitting white compression t-shirt was fitted to assure an optimum SLP signal with all the measurements taken while the participants were seated on a chair with back support and instructed to remain still (movement artefacts can result in erroneous SLP data). If a face mask was worn, patients were instructed to remove it. The SLP head unit angle was adjusted for each patient, with the midpoint of the projected grid aligned medially at the xiphoid process. The size of the projected grid was changed to fit and cover as much of the anterior trunk area as possible. SLP data were collected during 5 min of relaxed tidal breathing by the same operator under the same testing environment.
Tidal breathing parameters
Timing indices
The SLP recording allowed calculation of the respiratory rate (RR), inspiratory time (Ti), expiratory time (Te), total time for a full cycle of breath (Ttot), the ratio of Ti to Te (Ti/Te), ratio of Ti to the total time of breathing (Ti/Ttot) and the ratio of the inspiratory flow at 50% of the tidal breathing to the expiratory flow at 50% of the tidal breathing (ie, 50).
Regional parameters
These parameters are obtained from the regional displacement signals of the TA area after dividing them into lower and upper compartments. The contribution of each compartment to the overall ventilation is calculated, giving the relative thorax (rCT) and relative abdomen (rAB) as a percentage of the total. Breath phase angle (PA) is calculated and represents the degree of synchrony between the two compartments. PA ranges from 0° (fully synchronous) to 180° (fully asynchronous or ‘paradoxical’).
Entropy analysis
SLP tidal breathing recordings were exported as raw data and subsequently imported into LabChart 8 (AD Instruments, Oxford, UK) for analysis. Breath to breath interval (B-B interval) was calculated between consecutive tidal breath peaks. The SD of the B-B interval (SDBB) and the root mean square of the successive differences of the breaths (RMSSD) were then calculated to assess the total variability of breathing and the short-term variability between breaths. The peak height (max to min) was calculated for each breath as a surrogate for tidal volume, and the volume to volume interval (VT-VT interval) was then identified, and the mean was calculated (VT-VT Interval), with both the SD of the VT-VT interval (SDVT) and RMSSD calculated subsequently. All data were calculated using Excel (Microsoft UK) for all groups, and these measurements were used as measures of breathing entropy (variability).
Statistical analysis
The distribution of data was checked with the Shapiro-Wilk test. Normally distributed data were expressed as mean±SD, data that were not normally distributed were expressed as median ±IQR. Comparisons between the three groups were performed using the non-parametric Kruskal-Wallis test followed by Dunn’s multiple comparison test. The χ2 test was used to compare categorical data between groups. A value of p<0.05 was considered statistically significant. GraphPad Prism V.9.0.1 for Windows (San Diego, California, www.graphpad.com) was used for both statistical analyses and graphical representation.
Patient and public involvement
This study was conducted to assess the changed breathing pattern outcomes of patients hospitalised with COVID-19 in medical wards and ITU after at least 3 months of discharge, which was part of a scheduled post-COVID-19 RFT appointments and healthy subjects data were retrieved retrospectively. Patients were not involved in the design and conduct of the study. The results will be disseminated via publication of the study findings and social media.
Results
Subjects
All demographic data are summarised in table 1. Thirty healthy subjects with previously recorded SLP data were compared with a total of 110 COVID-19 recovery patients. Fourty-five patients were treated in wards and 65 patients were treated in the ITU. The ward group was 62% men (similar to the healthy subject group); however, the ITU group comprised 74% men. Healthy subjects were significantly younger than both ward and ITU patients. BMI was significantly higher in both the ITU and ward group compared with the healthy subjects, with a significantly higher proportion of ITU patients and ward patients being categorised as obese compared with healthy subjects. There were no significant differences in smoking history, with the majority of healthy subjects and patients with COVID-19 having never smoked.
Summary of the demographic characteristics of healthy and patients with post-COVID-19 previously admitted to wards and ITU
Tidal breathing parameters
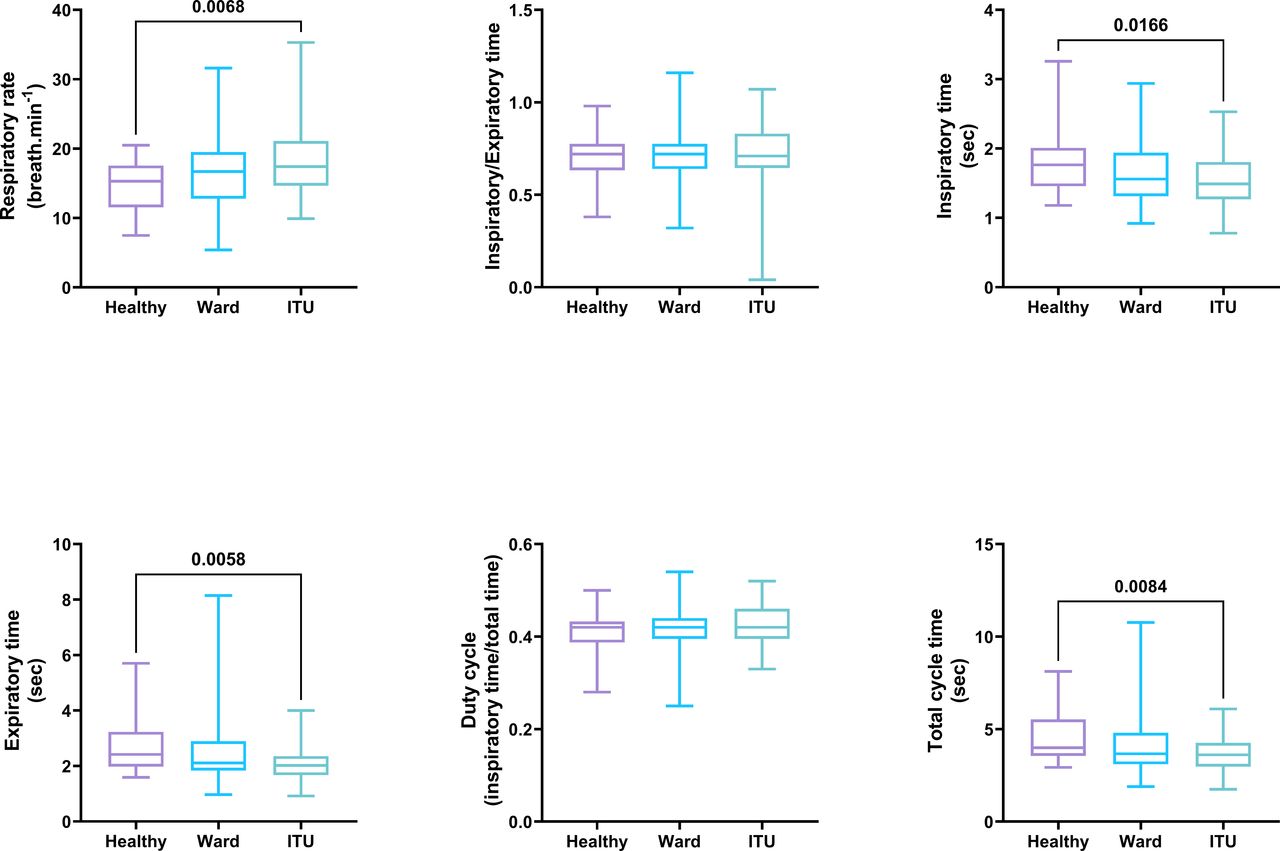
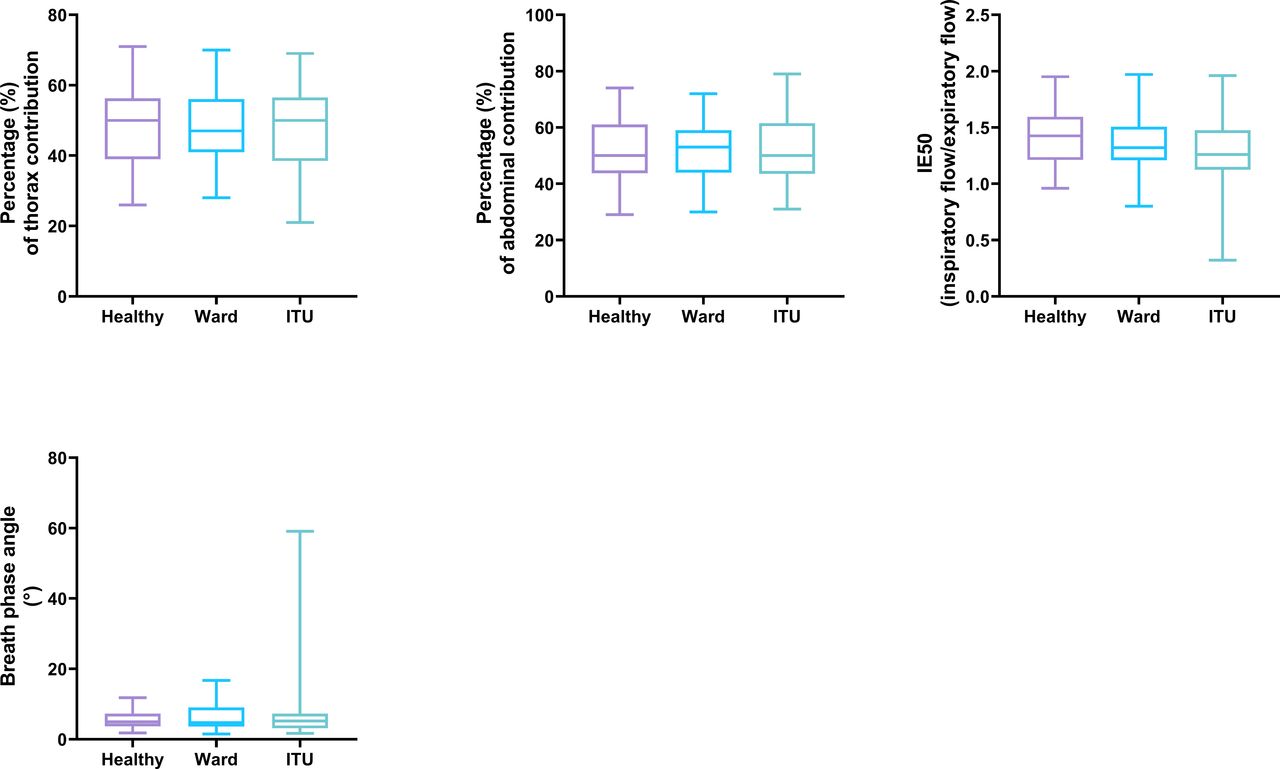
A significantly higher RR was observed in ITU patients compared with healthy subjects, but no significant difference was observed between the healthy subjects and ward patients or ITU compared with ward patients (figure 1). This corresponded to a similar pattern in Ti, which was significantly shorter in the ITU patients compared with healthy subjects (figure 1), with the ward patients being in between these. The pattern continued with a significantly lower Te in the ITU patients compared with the healthy cohort (figure 1). Unsurprisingly, there was also a significant decrease in Ttot of the ITU patients compared with the healthy cohort (figure 1). Duty cycle was not different between groups showing proportionate changes in both Ti and Te. Figure 2 details additional tidal breathing parameters that show no significant difference between any groups in IE50. Furthermore, there were no significant differences in the relative contribution of either the thorax and abdomen (rCT, rAB) to breathing or the breath PA, denoting the degree of synchrony.

A box and whiskers plot of a Kruskal-Wallis test of the compared tidal breathing parameters (respiratory rate (RR), the ratio of inspiratory time to expiratory time (Ti/Te), inspiratory time (Ti), expiratory time (Te), duty cycle or the inspiratory to total time ratio (Ti/Ttot) and the total time for a full respiratory cycle (Ttot) between healthy, intensive trauma care patients (ITU) and the ward admitted patients of structured light plethysmography (SLP) recording during seated position. Median ± IQR with minimum and maximum points presented. p<0.05 considered significant.

A box and whiskers plot of Kruskal-Wallis test of the compared tidal breathing parameters (total time for a full respiratory cycle (Ttot), and inspiratory to expiratory flow at 50% tidal volume (IE50)), the relative contribution of the thorax and abdomen to breathing (rCT, rAB) and breath phase angles (PA) between the healthy, intensive trauma care patients (ITU) and the ward admitted patients of structured light plethysmography (SLP) recording during seated position. Median ± IQR presented with minimum and maximum points. p<0.05 considered significant.
Measurement of entropy
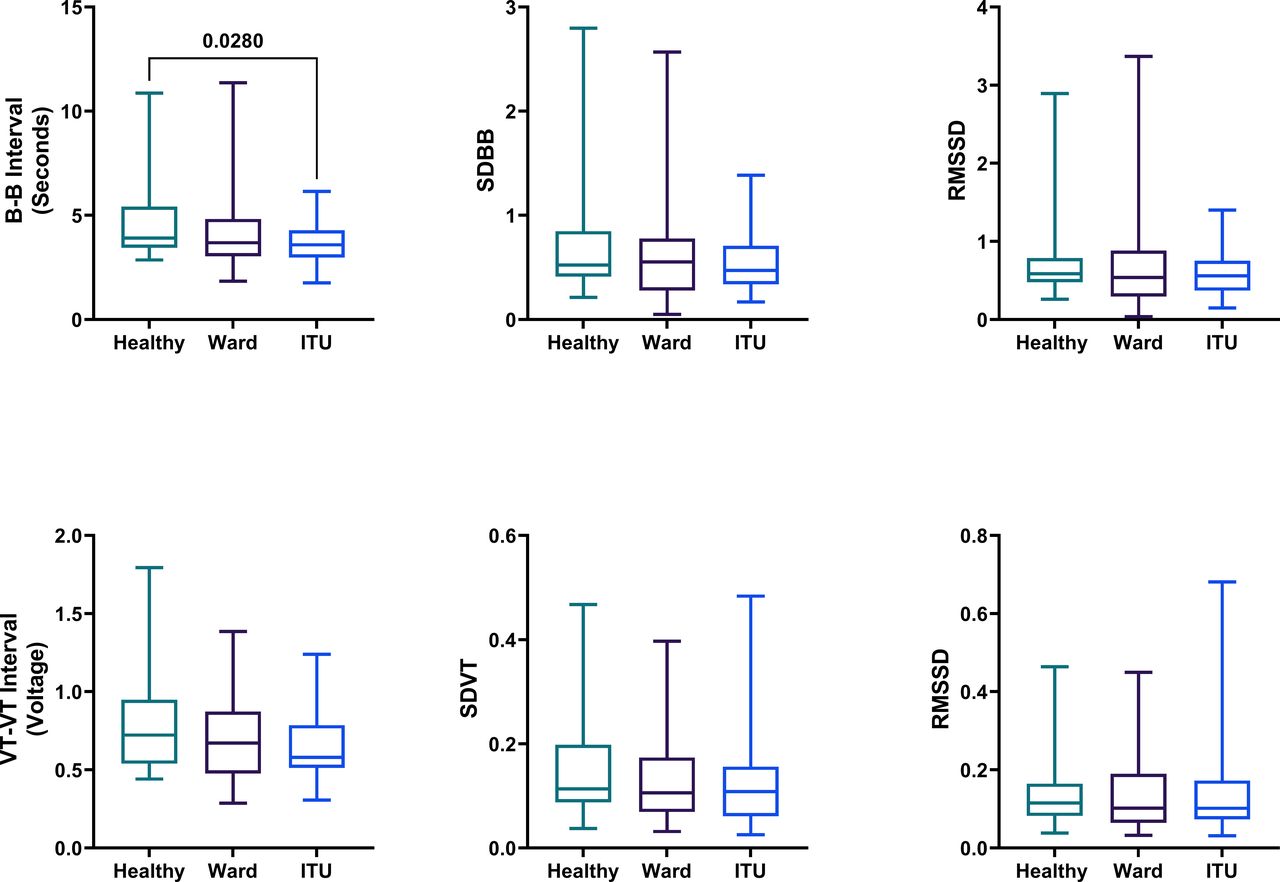
The B-B interval of ITU patients was significantly lower compared with healthy subjects (figure 3), and even though the mean interval was low, the SDBB and RMSSD were not significantly different. However, no significant differences in the healthy subjects compared with ward patients or between ward patients and ITU patients. No differences in the VT-VT interval or its calculated SDVT and RMSSD between all groups when compared.
{kind=link}
{kind=link}
{kind=link}
A box and whiskers plot of Kruskal-Wallis test for the variability of breathing measurement parameters through counting the breath to breathe interval and the volume to volume Interval of the whole breathing cycle (the mean of B-B interval, the mean of the VT-VT interval, SDBB, SDVT, RMSSD. Median ± IQR with minimum and maximum points presented p<0.05 considered significant. B-B interval, breath to breathe interval; ITU, intensive therapy unit; RMSSD, root mean square of the successive differences of the B-B interval and VT-VT interval; SDBB, SD of the breath to breath interval; SDVT, SD of the volume to volume interval; VT-VT interval, volume to volume interval.
Discussion
Main findings
The present study shows that measurement of breathing patterns during normal quiet tidal breathing is easily accomplished in a non-invasive, non-contact manner using SLP. The data recorded can be analysed using the traditional breathing parameters; however, using entropy analysis may provide a window to detect changes in breathing patterns otherwise obscured. In this study, we report that patients with COVID-19 who were admitted to ITU and required ventilatory support had a reduced variability in their resting respiratory frequency when compared with healthy controls.
COVID-19 infection and breathing
Despite having systemic effects, COVID-19 is considered to be a respiratory infection.20 As the pulmonary infection progresses, it can promote epithelial and pulmonary vascular damage resulting in more severe symptoms such as pulmonary oedema and potentially ARDS.21–23 Susceptible patients may require multiple medications, supplemental oxygen and also mechanical ventilation in intensive care,7 22 23 helping to mitigate a decreased efficiency of oxygen transfer—globally, the COVID-19 pandemic has already caused millions of deaths.4 The wide range of responses to COVID-19 infection in patients may consequently result in a range of differences during the recovery from infection and may have some link into the determination of a long-COVID syndrome.18 24
In our COVID-19 patient group, there was a higher proportion of men being hospitalised and admitted to ITU (74% ITU, 60% ward male patients) compared with women. This is consistent with previous findings,25 suggesting that gender differences can play a role in the disease severity and outcomes.
Dysfunctional breathing does not have a fixed definition but is rather, a generic term used to describe any abnormal breathing pattern.26 It is commonly observed in hospitalised patients and, hence, we used SLP to quantify entropy as part of assessment of dysfunctional breathing in COVID-19 recovery patients approximately 3 months postdischarge.
Damage from COVID-19 has been seen in various organs and not only the lungs, with a particular emphasis on the lungs, kidneys and brain. If some aspect of damage is seen in the brainstem, this may contribute to abnormal breathing patterns,27 while effects on the cardiovascular system may also impact breathing patterns28 observed during quiet tidal breathing.
Recovery of the respiratory system from COVID-19 has previously been investigated the following discharge from the hospital using other RFT techniques such as spirometry or gas transfer testing, which shows a decreased diffusion capacity with raised transfer coefficient and a restrictive pulmonary pattern as defined by an abnormally low total lung capacity.24 29–32 Spirometry results are very dependent on patient compliance and cooperation alongside the skills of the healthcare professional in promoting this increasing the chances of human errors or affecting the quality of the test13; however, SLP measurements just require natural resting tidal breathing reducing the potential impact of patient compliance and eliminating the mouthpiece effect. Thus, results obtained by spirometry (representing the limits of lung function with forced manoeuvres) and SLP (representing quiet tidal breathing) may well show differing results.
SLP is non-invasive and effort-independent and contactless—it may minimise COVID-19 cross-contamination risk in lung function laboratories by not generating aerosols that can act as either a surrogate for the other more traditional RFTs33 34 or at least act as a screening test to highlight patients requiring RFTs. In addition to measuring traditional respiratory parameters such as tidal volume and RR, we determined any changes in breathing patterns in post-COVID patients using SLP.
In our analysis, we found no significant differences between ITU and ward patients. This might seem surprising since, by definition, the ITU patients developed more serious conditions as a result of their COVID-19 infection. All patients were successfully recovering from infection regardless of the severity of their initial condition; however, it is also worth noting that the more invasive treatment required in ITU did not in itself induce any long-lasting effects that were measured in this study.35 There is also evidence to suggest that internal damage to the lungs in the form of pulmonary fibrosis29 can result from prolonged mechanical ventilation.
ITU patients did have a significantly higher RR—both shorter inspiratory and Tes with a reduced tidal volume and lower IE50 compared with healthy controls. This supports previously reported results where patients with COVID-19 demonstrated a restrictive pattern.31 32 ITU patients showed a higher work of breathing, with an increase in the duty cycle. The increased contribution from the abdomen to breathing may be the effect of the respiratory muscle weakness after invasive mechanical ventilation.36
Obesity is a contributing factor in either acquiring the virus or even worsening the disease’s condition in patients with COVID-19 .37 38 In our study, there was a higher proportion of obese patients in ITU (63%) and wards (53%) patients compared with healthy (16.6%) cohorts. Obesity can lead to extrapulmonary restriction by limiting chest wall mechanics, resulting in reduced lung volumes.39 Thus, the differences we observed might also relate to obesity itself as well as the after-effects of COVID-19.
Entropy analysis
Entropy is a measure of randomness in a system that can be used to quantify complexity.15 The concept of assessing the variability of a parameter has been explored in different disciplines, and the entropy or variability of breathing was adapted from the concept of heart rate variability40 and may provide a valuable measure to recognising patterns of dysfunctional breathing. While SLP cannot directly measure lung volumes, differences between breaths from a rate domain and volume domain can be determined with waveform analysis from SLP raw data.
We analysed SLP data to get measures of entropy to detect potentially dysfunctional breathing with a particular focus on the severity of the disease (ITU vs ward patients).
We did not observe any significant differences in the variability of breath intervals in ward patients. However, we noted that the SDBB as a measure of the distribution of the data around the mean representing changes of the total variability of the whole breath cycle and RMSSD that measures the differences in the adjacent breaths that shows short-term variability between breaths, which showed lower VT voltage changes and frequency changes in the ITU group and a significantly higher B-B interval changes especially when compared with the healthy subjects contributed to the significantly increased RR.
We can see from this trend in breathing patterns that the patients who come from ITU have a more controlled breathing pattern, with significantly reduced B-B variability and a tendency for reduced VT-VT variability also (figure 3). This is mentioned above and might be due to the effects of the COVID-19 virus on the breathing centres in the brain, but this has proven difficult to confirm,41 42 and it is beyond the scope of this study. Comparing the data to breathing patterns in other diseases or further follow-up of the same patient could help in establishing a starting point to follow these changes, and it may be a helpful tool to assess pulmonary rehabilitation progress in patients with COVID-19 with different severities of disease during recovery.
In summary, our finding suggests that SLP can be used to detect some differences in tidal breathing during recovery from COVID-19, particularly those who were treated in the ITU with invasive ventilation, indicative that changes and long-lasting effects of COVID-19 are linked with the severity of the disease as manifested by the ward compared with ITU patients. In addition, we have successfully managed to elicit breathing entropy parameters using the waveform analysis of raw data extracted from the SLP, which is a novel and informative technique. SLP data can be successfully used in conjunction with traditional respiratory function tests such as spirometry, gas transfer and lung volumes to provide a greater understanding of a patient’s breathing.
Limitations
The COVID-19 pandemic prevented routine access to make recordings. Data used for the healthy cohort were acquired prior to the pandemic, and, as such, it was impossible to match the patient demographics. Consequently, differences in age or BMI may contribute to the observed differences in breathing between the healthy subjects and COVID-19 recovery patients. However, as the breathing rate decreases with age,43 this suggests that age alone is not the cause.25 The exact effects of the COVID-19 virus on breathing regulation may be difficult to elicit since patients were treated according to medical need, and so variations in symptom severity and subsequent therapeutic interventions may have induced greater variability in the data analysis. The COVID-19 recovery patients had no previous RFT measurements on record and were assumed to be healthy prior to the infection; however, this cannot be determined with absolute confidence since this was not a prospective study. SLP reference ranges are only recently derived and may not discriminate well between normal healthy and abnormal. The inclusion of a healthy cohort helps to mitigate this potential issue.
Conclusion
SLP is able to assess the short-term physiological effects of COVID-19 on breathing patterns, particularly in combination with the other assessments of pulmonary function. Patients admitted to the ITU exhibited more residual changes in their breathing 3 months after hospital discharge.
Surprisingly, patients with COVID-19 treated in ITU patients and ward patients appeared to have similar breathing patterns, suggesting that more severe symptoms and invasive ventilation did not further influence physiological outcomes at least 3 months after discharge. SLP and entropy analysis can provide useful clinical information on COVID-19 recovery patients at least in the short term and, potentially, to monitor recovery long-term.
Data availability statement
Data are available upon reasonable request. The data for the study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This work uses data provided by patients and collected by the NHS as part of their care and support at University Hospitals Birmingham NHS Foundation Trust. The requirement for written informed consent and ethical approval has been waived by University Hospitals Birmingham NHS Foundation Trust Clinical Audit Registration and Management System (Audit Code: CARMS-16371). All relevant guidelines have been followed for the study.
Acknowledgments
Our thanks go to Dr. Nandan Gautam, Dr. Shyam Madathil, Dr. Natascia Tahani, Shaun Bolton, Dr. Dhruv Parekh, Dr. Shuraddah Goyal, Hannah Qureshi, Sadhika Yasmin, Dr. Jennifer Short, Dr. Tarekegn Geberhiwot and the staff of the Lung function and Sleep Department at University Hospitals Birmingham for the teamwork and the coordination in the data collection process.
References
Footnotes
Contributors Experimental concepts and method design were devised by EA, JS, AC and BC. Data were collected by EA assisted by JS. Data were interpreted and analysed by EA. Original drafting of the manuscript was done by EA and was reviewed and edited by all authors. The project was supervised by AC and BC. AC is the guarantor for the study. Funding acquisition by EA. All authors have read and agreed to the published version of the manuscript.
Funding A scholarship from King Saud bin Abdulaziz University for Health Sciences (KSAU-HS) (Riyadh, Saudi Arabia) was provided to EA through the Saudi Arabian Cultural Bureau in London (SACB) grant number (KSHU250) and AC was funded by University of Birmingham, UK.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.