Article Text

Abstract
Background Inhaled therapies are key components of asthma and chronic obstructive pulmonary disease (COPD) treatments. Although the use of pressurised metered-dose inhalers (pMDIs) accounts for <0.1% of global greenhouse gas emissions, their contribution to global warming has been debated and efforts are underway to reduce the carbon footprint of pMDIs. Our aim was to establish the extent to which different scenarios led to reductions in greenhouse gas emissions associated with inhaler use, and their clinical implications.
Methods We conducted a series of scenario analyses using asthma and COPD inhaler usage data from 2019 to model carbon dioxide equivalent (CO2e) emissions reductions over a 10-year period (2020–2030) in the UK, Italy, France, Germany and Spain: switching propellant-driven pMDIs for propellant-free dry-powder inhalers (DPIs)/soft mist inhalers (SMIs); transitioning to low global warming potential (GWP) propellant (hydrofluoroalkane (HFA)-152a) pMDIs; reducing short-acting β2-agonist (SABA) use; and inhaler recycling.
Results Transition to low-GWP pMDIs and forced switching to DPI/SMIs (excluding SABA inhalers) would reduce annual CO2e emissions by 68%–84% and 64%–71%, respectively, but with different clinical implications. Emission reductions would be greatest (82%–89%) with transition of both maintenance and SABA inhalers to low-GWP propellant. Only minimising SABA inhaler use would reduce CO2e emissions by 17%–48%. Although significant greenhouse gas emission reductions would be achieved with high rates of end-of-life recycling (81%–87% of the inhalers), transition to a low-GWP propellant would still result in greater reductions.
Conclusions While the absolute contribution of pMDIs to global warming is very small, substantial reductions in the carbon footprint of pMDIs can be achieved with transition to low-GWP propellant (HFA-152a) inhalers. This approach outperforms the substitution of pMDIs with DPI/SMIs while preserving patient access and choice, which are essential for optimising treatment and outcomes. These findings require confirmation in independent studies.
- inhaler devices
- asthma guidelines
- asthma
Data availability statement
Data used in this analysis are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
In asthma and chronic obstructive pulmonary disease (COPD) patients using metered-dose inhalers (pMDIs) containing high global warming potential (GWP) propellant, what is the best option to both reduce greenhouse gas emissions while also ensuring patients’ health and treatment choice?
The transition to low-GWP propellant pMDIs outperforms switching to a different device type while also preserving patient access and choice, thus giving better treatment and outcomes.
This study provides a detailed analysis of multiple scenarios, providing healthcare systems and governments with data demonstrating how investing in sustainable innovation can reduce the environmental impact of alternative therapies while preserving safety, health and choice for patients with asthma or COPD.
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are the most common chronic respiratory diseases and are among the leading causes of morbidity and mortality, worldwide.1 It is estimated that there are at least 300 million patients with asthma and 328 million patients with COPD.2 3 Inhalers are important devices that reduce morbidity and mortality associated with these diseases and significantly improve quality of life.4 5
International recommendations advocate a tailored, personalised approach for choosing the most suitable inhaler for each patient.2 6 The two main classes of inhaled medications are bronchodilators (short-acting and long-acting β2-agonists and antimuscarinic agents) and inhaled corticosteroids (ICS), each delivered as single agents or in combination via a handheld inhaler. New therapeutic approaches administered through the inhaled route are also in development.
Inhaled therapies are necessary as key components of asthma and COPD treatment, but currently their contribution to greenhouse gas emissions, and hence global warming, is being discussed.7 8 The three principal types of inhalers are: pressurised metered-dose inhalers (pMDIs; used with or without holding chambers or spacers, some are breath-actuated), dry-powder inhalers (DPIs; reservoir, multi-dose and single-dose rechargeable) and soft mist inhalers (SMIs). For all these device types, carbon footprint can be calculated throughout the life cycle of the product, including raw materials, production, transport, use and waste disposal.7 8 The use of pMDIs relies on the driving force of propellants to atomise droplets containing drugs for deposition in the lungs.9 The propellants used in pMDIs are hydrofluorocarbons (HFCs), which are greenhouse gases and for this reason the carbon footprint of a pMDI is higher than a DPI or SMI, with the use and disposal phases providing the larger contribution.7 8 However, even after considering this, it is calculated that the use of pMDIs accounts for <0.1% of total global greenhouse gas emissions.10–13 In contrast, drug delivery with DPIs and SMIs occurs without a propellant, and thus their carbon footprint is mainly dependent on the raw materials and manufacturing process.7 8
Carbon dioxide equivalent (CO2e) is the unit for comparing the radiative forcing of a greenhouse gas (GHG) to that of CO2. The mass of a GHG is converted into CO2e by multiplying by the corresponding global warming potential (GWP).14 In some countries, there is a drive to reduce CO2e emissions by restricting the use of pMDIs and encouraging the use of DPIs.15 However, changing inhaler class has important implications for patients, since pMDIs are more suitable for many patients because of, for example, inhaler type, insufficient inspiratory flow rate, or handling capabilities and individual preference.16 Moreover, switching from pMDIs to DPIs could have other environmental impacts, including human toxicity, marine eutrophication and fossil depletion.8 Therefore, there is an unmet need to ensure that patients continue to receive the most effective and appropriate treatment while also reducing the negative impact of inhalers on the environment.
Deciding on the optimal choice of inhaler for each patient is essential to maximise treatment outcomes; such complex decisions are shared between the healthcare practitioner and patient.4 5 Changing treatment to a different type of inhaler class can have negative impacts on patients and may lead to reduced medication adherence.17 Conversely, simplifying treatment strategies and minimising inhaler options may have a positive effect on disease control in some patients; therefore, it is important to consider a patient’s individual circumstances before initiating a switch.18 The European Respiratory Society (ERS) acknowledges the environmental impact of pMDIs, but stresses the need for a multifaceted approach, focusing on patient safety and choice rather than just focusing on the device.19
Novel approaches are being considered to reduce the carbon footprint of pMDIs, to balance environmental goals with patient health and well-being.9 The development of pMDI devices that contain low-GWP propellants, while optimising the quality of patient care, is one focus.20 21 The hydrofluoroalkane (HFA) propellant, HFA-152a, has a substantially reduced GWP100 (GWP over 100-year time horizon) of 138.13 Replacing the current propellants in pMDIs, HFA-134a (GWP100, 1300) and HFA-227ea (GWP100, 3350) with HFA-152a (GWP100, 138), which would reduce GWP by 89% and 96%, respectively,13 would result in carbon emissions within the range of DPIs.8 Consideration should also be given to inhaler recycling since environmental impact can be reduced through recovery of leftover propellant.22
To understand the extent to which different courses of action could lead to reductions in greenhouse gas emissions associated with pMDIs, thereby decreasing their carbon footprint, we conducted a series of scenario analyses using asthma and COPD inhaler sales data from 2019 to model emissions reductions over a 10-year period for five reference markets: the UK, Italy, France, Germany and Spain.
Methods
Analyses
This was an exploratory study to evaluate the potential impact on asthma and COPD inhaler-associated GHG emissions for four possible reduction scenarios: (1) Imposing a switch from pMDIs to DPI/SMIs; (2) Replacing current propellants used in pMDIs with a low-GWP propellant (for this scenario, HFA-152a was the candidate selected because it is at an advanced stage of development for pharmaceutical use, and due to the amount of publicly available data); (3) Clinical optimisation of asthma maintenance therapy to reduce short-acting β2-agonist (SABA) inhaler use; and (4) Inhaler end-of-life recycling.
All four scenarios were examined in five reference markets: the UK, Italy, France, Germany and Spain. For each market, total inhaler-associated GHG emissions (measured in CO2e emissions) were defined as the ‘current case’. Where specified, total inhaler-associated emissions were from asthma and COPD inhalers, excluding SABA inhalers. With the different type of use, ‘as needed’, and different posology to other classes, emissions of SABA inhalers were assessed in a separate scenario, with the carbon footprint evaluated in terms of canister usage. The ‘current case’ (2019 emissions data) served as the framework against which emission reductions over a 10-year period from 2020 to 2030 were estimated.
The primary objective of the study was to establish the extent to which the different scenarios led to reductions in GHG emissions associated with inhaler use. Data used in this study were internally verified and provided by the sponsor (Chiesi Farmaceutici, Italy) or were retrieved from peer-reviewed publications or recognised databases by Aequilibria (Venezia, Italy) (see online supplemental information). All analyses were performed by Aequilibria.
Supplemental material
Principal assumptions
As DPIs and SMIs do not require a propellant and have similar carbon footprints,7–9 SMIs were modelled as DPIs and aggregated into one category that included both DPI and SMI products (termed DPI/SMIs). To develop the current case for each market, data for individual units sold over the full year 2019 were combined with information on posology and number of actuations for each inhaler to derive a total equivalent-months of treatment for each product (online supplemental table 1). This was subsequently combined with the carbon footprint for 1 month of treatment with each product (online supplemental table 2) to calculate total CO2e emissions. To calculate the carbon footprint per month of treatment (kg CO2e), the carbon footprint values related to the single puff (for pMDIs) or actuation (for DPI/SMIs) were multiplied by the number of daily puffs/actuations needed, multiplied by 30 (days per month), using carbon footprint values previously published.9 22–25 For each of these published values, the GWP100 of the different propellants was taken from Intergovernmental Panel on Climate Change fifth assessment report.13 Product sales in 2019 were assumed to remain constant throughout the assessment period. This was to avoid including an additional layer of uncertainty and complexity to the modelling by requiring a further assumption on product/class forecasts that may be challenged.
Further details for each scenario are provided in the online supplemental material.
Scenario analysis
Scenario 1: switch from pMDIs to DPI/SMIs
This scenario analysed the impact of switching inhaler types, from pMDIs to DPI/SMIs, to reduce emissions due to the propellant gas in pMDIs. SABA inhalers were excluded from this analysis and are analysed separately in the following scenarios. A clinical correspondence between products was defined (online supplemental table 3). To reflect a realistic market behaviour, a transition period of 10 years (2020–2030) for switching from pMDIs to DPI/SMIs was considered.
Three strategies for switching from pMDIs to DPI/SMIs were evaluated: (1) Forced case: Imposed substitution of 80% of pMDI products with DPI/SMI products by 2030, assuming a linear trend for the transition; (2) Forced accelerated: As for the Forced case strategy, but with an accelerated transition that achieves 50% substitution of pMDIs with DPI/SMIs by 2025; and (3) Clinically feasible (that is based on historical data of clinically-driven switch): Each year the switch from pMDIs to DPI/SMIs affects 5% of the previous year’s pMDI sales, resulting in approximately 40% substitution by 2030 (non-linear trend).
Scenario 2: transition to low-GWP propellant
The second scenario for reducing inhaler-associated emissions considered the replacement of current pMDIs (ie, with a high-GWP propellant such as HFA-227ea or HFA-134a with a GWP100 of 3350 and 1300, respectively) with pMDIs containing a low-GWP propellant, HFA-152a (GWP100 of 138).13 The transition is assumed to occur as a replacement of the product on the market with the new one containing HFA-152a propellant, rather than a switch and thus is assumed to occur within 1 year. Two subscenarios were considered for the inhaler transition—one involving only the study sponsor’s products (those with the greatest patient use): beclometasone/formoterol/glycopyrronium bromide (‘Trimbow’), beclometasone/formoterol (‘Foster’ (or other brand names in different countries)) and beclometasone (‘Clenil’ (or other brand names in different countries)) and one involving the whole market. Assumptions for the whole market case included that all non-study sponsor products applied the low-GWP propellant transition to the whole pMDI market (SABA excluded), and that non-study sponsor products followed the same transition periods as the study sponsor products in the same class. Long-acting β2-agonist pMDIs were excluded in the transition due to their limited market share in the considered countries. With announcements setting first approvals in 2025, a roll-out period was assumed for the different products over 2 years (2026–2027).
A subscenario considered the inclusion of SABA pMDIs in the whole market transition to the low-GWP propellant HFA-152a (SABA pMDIs represent 94%, 73%, 99%, 97% and 89% of total SABA sales in the UK, Italy, and France, Germany and Spain, respectively).
Scenario 3: optimisation of asthma maintenance therapy to reduce SABA use
This scenario analysis evaluated the potential for reducing inhaler emissions through clinical optimisation of asthma maintenance therapy (to obtain disease control and prevent exacerbation and lung function impairment) leading to a reduction in SABA inhaler use.
The main assumption was that for patients with moderate/severe asthma (as per steps 3–5 of the clinical recommendations2), clinical optimisation of maintenance therapy could lead to elimination of SABA inhaler use exceeding two inhalers/year. For patients with intermittent or mild asthma (as per steps 1 and 2 of the clinical recommendations2), likely not receiving any maintenance treatment, two modes of treatment optimisation were considered: Option 1: two SABA canisters/year with the excess substituted with four ICS inhalers/year; and Option 2: all SABA inhalers substituted with two ICS/formoterol inhalers/year. Both options are proposed in the clinical recommendations2 and were applied here, considering ICS maintenance therapy (Option 1) as being within-label. The number of SABA products that should theoretically be avoided each year, and the number of replacement ICS or ICS/formoterol inhalers for patients with mild disease, were considered in conjunction with their respective carbon footprint to quantify the total reduction of GHG emissions. A transition period of 10 years from 2020 to 2030 was considered (assuming a linear trend).
Scenario 4: inhaler end-of-life treatment
This scenario analysis considered the implementation of an inhaler recycling scheme of different levels of ambition to reduce inhaler end-of-life emissions. It was assumed that the carbon footprint of security doses (leftover propellant) was constant and equal to 25% (based on evaluations by the sponsor company on a range of available pMDI products) of the total product carbon footprint. The remaining end-of-life emissions are attributable to the actual disposal treatment. Three disposal behaviours were identified: domestic disposal, return to pharmacy and recycling, only the latter of which was assumed to correctly collect the excess propellant.
Statistical analysis
This study was exploratory, and no statistical hypotheses were evaluated. For each of the scenarios examined, emissions data for the five reference markets (the UK, Italy, France, Germany and Spain) are described as total monthly or yearly tons of CO2e emissions plotted across the 10-year assessment period (2020–2030).
Patient and public involvement
Patients were not involved in the study.
Results
Current case total GHG emissions
Including SABA inhalers, total CO2e emissions from asthma and COPD inhaled products were largest in the UK (1300 kilo tons (kt)), less than half of this in France (520 kt) and Germany (450 kt), approximately a quarter of this in Spain (330 kt) and approximately a sixth of this in Italy (190 kt) (table 1). For all five markets, more than 90% of CO2e emissions were attributable to pMDIs, with a predominance of market share for pMDIs in the UK (approximately 70%), DPIs in Italy (63%), Germany (57%) and Spain (55%), and a comparable share between device types in France (pMDIs 52% and DPIs 48%). For all five markets the greatest contribution to the total CO2 emissions comes from SABA pMDI products.
Calculated total greenhouse gas emissions from inhaled products in 2019 for each of the five reference markets. Values are given to two significant figures
Switch from pMDIs to DPI/SMIs
Excluding SABA inhalers, both forced and forced accelerated case substitution strategies would result in a substantial reduction of CO2e emissions by 2030 in all five reference markets, reductions that far exceed those observed for the clinically feasible strategy (figure 1A). Overall for the five countries studied, CO2e emissions would fall by 68% for both forced case strategies compared with 27% for the clinically feasible strategy. In the UK, CO2e emissions would fall by 71% for both forced case strategies versus 20% for the clinically feasible strategy. Similarly, for Italy, France, Germany and Spain, the forced case strategies would reduce CO2e emissions by 64%–67% compared with 32%–35% for the clinically feasible strategy (figure 1B and online supplemental figure 1).
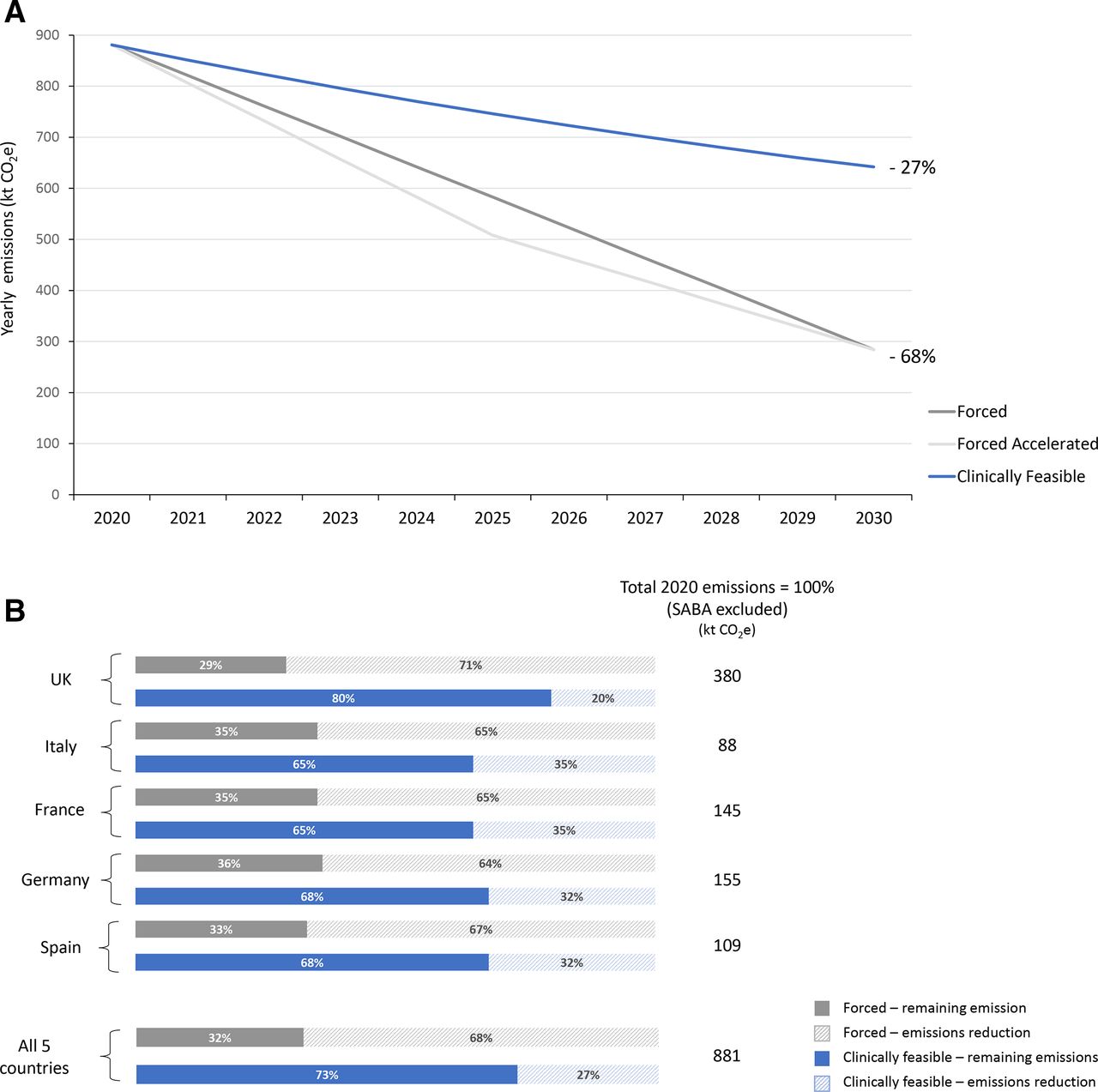
Total CO2e emissions reduction, by 2030, in the scenario of switch from pMDIs to DPI/SMIs (excluding SABA inhalers) in the three subscenarios of switch (A) % reduction trends across the five countries and (B) % reduction for the five countries + total in the case of switch to DPI/SMIs with forced or clinically feasible subscenarios (for single countries UK, Italy, France, Germany and Spain, see online supplemental figure 1). Both forced subscenario strategies result in greater yearly emissions reductions than the clinically feasible scenario across the 10-year assessment period for each reference market. Forced: substitution of 80% of pMDIs with DPI/SMIs by 2030, assuming a linear trend; forced accelerated: substitution of 80% of pMDIs with DPI/SMIs by 2030, but with 50% substitution by 2025 and the remaining 30% achieved between 2025 and 2030; clinically feasible: based on historical data, every year there is substitution of pMDIs with DPI/SMIs for 5% of the previous year’s pMDI sales, resulting in a non-linear trend and a final reduction of 40% by 2030. SABA inhalers were excluded in this scenario. CO2e, carbon dioxide equivalent; DPI, dry-powder inhaler; kt, kilo tons; pMDI, pressurised metered-dose inhaler; SABA, short-acting β2-agonist; SMI, soft mist inhaler.
Transition to low-GWP propellant pMDIs
Excluding SABA pMDIs
Across all five reference markets, a substantial reduction in CO2e emissions would be observed following the transition of the study sponsor’s pMDIs to HFA-152a products. Total monthly CO2e emissions for the UK would fall by 47% between 2020 and 2030; the proportion of emissions attributed to the sponsor’s products would drop from 53% to 11% over the same period. For Italy, the transition to HFA-152a pMDIs would result in a fall in total monthly CO2e emissions of 32% across 2020 to 2030, and for France, Germany and Spain, a reduction of 14%, 29% and 15%, respectively, with an average of 33% across all five countries (table 2). Beyond restricting the analysis to the sponsor’s products, the greatest reductions in total monthly CO2e emissions achieved by 2030 would be seen in a subscenario when the transition to HFA-152a pMDIs is carried across the whole inhaler market: 84%, 76%, 70%, 68% and 79% for the UK, Italy, France, Germany and Spain, respectively (table 2).
Total monthly carbon dioxide equivalent emissions reduction following the transition to low-GWP propellant (hydrofluoroalkane-152a GWP100, 138) in the case of column (1) only study sponsor’s products column (2) whole inhaler market, excluding SABA inhalers and column (3) whole inhaler market, including SABA inhalers
Including SABA pMDIs
In a subscenario, the inclusion of SABA pMDIs in the whole market transition to HFA-152a pMDIs was considered (without any clinical optimisation to reduce SABA use). For the UK, the SABA propellant transition would reduce monthly CO2e emissions of the SABA market by 89% in 2030; the transition of all inhalers would allow for a total reduction of GHG emissions in the inhalers market of 88%. Up to an 89% reduction in 2030 CO2e emissions from SABA inhalers would be also evident for Italy (83% total reduction) and France (89% total reduction), Germany (82% total reduction) and Spain (86% total reduction) (table 2).
SABA inhaler clinical use reduction through asthma maintenance therapy optimisation and transition to low-GWP propellant
The plots in figure 2 show estimated reductions in SABA inhaler-related emissions following clinical optimisation for all patients, separated by the optimisation strategy for patients with mild disease. For all five reference markets, optimisation would markedly reduce yearly SABA CO2e emissions by 2030: 54% and 69% for the UK, 25% and 32% for Italy, 43% and 61% for France, 39% and 52% for Germany, 58% and 65% for Spain and 48% and 63% overall with optimisation for mild disease based on Option 1 and Option 2, respectively (figure 2A). From our analysis, Option 2 (all SABA inhalers substituted with two ICS/formoterol inhalers/year in intermittent/mild asthma patients) leads to the greatest reduction of emissions. As SABA pMDIs account for a substantial proportion of total inhaler sales (44% in the UK, 22% in Italy, 34% in France, 26% in Germany and 31% in Spain), the impact of clinical optimisation to reduce SABA inhaler use was also estimated as a proportion of the whole inhaler market. By 2030, considering Option 2, clinical optimisation would result in a reduction of total yearly CO2e emissions of 48% for the UK, 17% for Italy, 44% for France, 34% for Germany, 43% for Spain and 42% overall (figure 2B).

SABA optimisation. Total CO2e emissions reduction across the five countries, by 2030, in the case of (A) % of SABA emissions reduction with Option 1 and Option 2 and (B) % of whole market emissions reduction with Option 2. Optimisation of asthma maintenance therapy to reduce SABA inhaler use results in substantial yearly emissions reductions across the assessment period for the five reference markets, with the greatest decreases evident when all SABA inhalers are substituted for two ICS/formoterol inhalers/year (SABA Option 2). Both depicted categories included: (1) all patients with asthma who properly use SABA inhalers (and are assumed to continue doing so); (2) patients with moderate/severe asthma and higher SABA use for whom clinical optimisation of asthma maintenance therapy was to reduce SABA use to two inhalers/year; and (3) patients with mild asthma for whom the clinical optimisation of asthma maintenance therapy followed one of two options: SABA Option 1: two SABA inhalers/year are maintained, while all excess is substituted with four ICS inhalers/year (within-label); SABA Option 2: all SABA inhalers consumption is substituted with two ICS/formoterol inhalers/year (currently off-label, but reported in clinical recommendations). Thus, the two plots shown differ only in the clinical optimisation strategy for patients with mild asthma. CO2e, carbon dioxide equivalent; ICS, inhaled corticosteroids; kt, kilo tons; SABA, short-acting β2-agonist.
Inhaler end-of-life recycling
Substantial reductions in CO2e emissions could be achieved with increasing levels of recycling (online supplemental figure 2). The impact of recycling would be lessened in the scenario of transition to low-GWP propellant pMDIs, due to the considerably lower end-of-life CO2e emissions of these inhalers (online supplemental figure 2).
Scenario comparisons
Direct comparison of these scenarios, implemented across the whole inhaler market (excluding SABA), show that the transition to HFA-152a propellant pMDIs would result in the strongest reduction of yearly emissions by 2030: 84%, 76%, 70%, 68%, 79%, 78% for the UK, Italy, France, Germany, Spain and overall, respectively (figure 3 and online supplemental figure 3).

{kind=link}
{kind=link}
{kind=link}
Comparison of (A) the reduction trends with switch from pMDIs to DPI/SMIs (three subscenarios) and low-GWP propellant transition (whole market excluding SABA inhalers) across the five countries and (B) differences in the % of total CO2e emissions reduction, by 2030, across the five countries, between the two most relevant scenarios (forced switch from pMDIs to DPI/SMIs and low-GWP propellant transition—whole market excluding SABA inhalers). When implemented across the whole inhaler market (excluding SABA inhalers), transition to low-GWP propellant pMDIs results in the greatest reductions in yearly emissions by 2030 for all five reference markets. DPI forced base: substitution of 80% of pMDIs with DPI/SMIs by 2030, assuming a linear trend; DPI forced accelerated: substitution of 80% of pMDIs with DPI/SMIs by 2030, but with 50% substitution by 2025 and the remaining 30% achieved between 2025 and 2030; DPI clinically feasible: based on historical data, every year there is substitution of pMDIs with DPI/SMIs for 5% of the previous year’s pMDI sales, resulting in a non-linear trend and a final reduction of 40% by 2030; Low-GWP propellant: transition from current propellant to low-GWP propellant (hydrofluoroalkane-152a). CO2e, carbon dioxide equivalent; DPI, dry-powder inhaler; GWP, global warming potential (100-year time horizon); pMDI, pressurised metered-dose inhaler; SABA, short-acting β2-agonist; SMI, soft mist inhaler.
While the recycling scenario theoretically could lead to 100% reduction in end-of-life CO2e emissions (online supplemental figure 2), the actual levels of recycling that could realistically be achieved are likely much lower. However, the transition to low-GWP propellant pMDIs without any recycling results in reductions in end-of-life CO2e emissions equivalent to the recycling of 87%, 81%, 85%, 86% and 84% of current inhalers in the UK, Italy, France, Germany and Spain, respectively.
Discussion
Despite the small contribution (<0.1%) that the use of pMDIs makes to total global GHG emissions,10–13 there is a drive to reduce the carbon footprint and increase the sustainability of life-saving inhaled medications for asthma and COPD. We demonstrate the environmental benefits of low-GWP propellant pMDIs, an approach being actively pursued by some companies with pMDI maintenance therapies, with the intention of these devices reaching the market by 2025.20 21 We show that marked reductions in yearly CO2e emissions across the whole inhaler market can be achieved by 2030 by switching from current pMDIs to pMDIs containing a low-GWP propellant (HFA-152a): 78% overall reduction excluding SABA inhalers and 89% overall including SABA inhalers. This would translate into a small absolute total GHGs emissions reduction, given the currently low contribution of inhalers. However, considering a shared accountability of fighting climate change, it is important to commit to reducing this portion of emissions, with actions that balance planet and patient health.
Reducing GHG emissions by progressively replacing the use of propellant-driven pMDIs with DPI/SMIs, which are propellant-free, is being considered in some countries as an immediate yet short-term strategy.15 However, alongside environmental considerations related to the use of inhaled medications, preserving patient well-being remains of paramount importance. Patient outcomes are directly linked to treatment success and restricting access to some treatment options has potentially detrimental effects on the quality of care that patients receive and their subsequent outcomes.16 17 26 27 Indeed, patient preference, adherence and inhalation technique are important closely inter-related determinants of clinical outcomes. As such, they may also influence healthcare costs. Other studies also advocate for the development of inhaler alternatives with lower carbon footprint while preserving patient-tailored treatments in the context of inhaler choice.9 Recently the ERS has highlighted concern about suggestions to switch therapies of stable respiratory patients from pMDI to a DPI purely for environmental reasons as the clinician duty of care is to put the patient first.19
Our data show that the substitution of pMDIs with DPI/SMIs can result in substantial yearly reductions in CO2e emissions (overall 68%) at the end of a 10-year transition period. Importantly, however, this was only realised when the substitution is imposed and is achieved for 80% of current pMDIs; this is a scenario that is unlikely to be attainable in practice due to the potential negative consequences on patient health. Furthermore, an approach that progressively phases out pMDIs has considerable clinical implications for patients, jeopardising safety and treatment outcomes.7 Studies in patients with asthma and COPD with stable disease have reported deterioration of disease control when a switch to an alternative inhaler was enforced without engaging the patient.26–28 Maintaining access to all inhaler types allows the most appropriate inhaler device for optimal asthma and COPD management to be prescribed, based on patients’ characteristics and preferences29 and a shared decision with the healthcare practitioner.30 31 The ERS highlights that restricting patient access to pMDIs would be a retrograde step for the respiratory medical community in modern times, especially for those where there is no viable alternative.19
Development of pMDIs containing a low-GWP propellant, such as HFA-152a,4 5 13 has the potential to reduce the carbon footprint of pMDIs by as much as 90%,7 to a level within the range of DPIs, with this changed encouraged by ERS.7 19 32 Critically, the development of these new pMDIs ensures that pMDIs remain a treatment option for patients and that the transition is made seamlessly. This in turn prevents deterioration of disease control, healthcare visits and adverse outcomes that might arise from an enforced switch of inhaler type.26–28 In our comparison, the emission savings for transition to low-GWP propellant in the whole inhaler market exceeded those achieved with the best-case switching scenario. However, the transition to low-GWP propellant inhalers, particularly for the whole market (and not restricted to only the study sponsor’s products), will take a longer time to be applied than switching to DPI/SMIs due to regulatory requirements and the time required for clinical development. Reduction achieved through transition to low-GWP propellant can start later, but these results can be maintained over time, according to the long-term policies and agreements that the participating countries committed to fulfil. It will be important to balance the short-term reductions in GHG emissions against the clinical risks involved with an immediate forced switch in inhaler device, ensuring switching therapies for non-therapeutic reasons does not constrain prescribers and patients in their choice for the most appropriate drug/device combination.33 Poor adherence to medications is never environmentally friendly, so a switch from a pMDI with good adherence to a different device with worse adherence is neither good for the environment nor the patient.33 34
SABA inhalers represent a considerable share of the total inhaler market in many countries and their overuse is common, with a recent analysis of UK data showing 83% of all SABA inhalers for asthma were prescribed to patients who were potentially overusing this medication (prescribed ≥3 inhalers/year).35 Clinical optimisation targeting SABA use as a marker of poor control and increased risk of poor outcome could provide clinical benefits,36 37 in addition to a reduction in CO2e emissions. By only reducing the higher use of SABA inhalers through generalised clinical optimisation of asthma maintenance therapy (if achievable), our data show that substantial yet varied yearly emissions reductions would be observed, noticeable not only for the SABA class of products but at the whole market level, with emissions savings observed proportional to the level of higher use in each country. However, including SABA pMDIs in the whole market transition to low-GWP propellant (HFA-152a) pMDIs would reduce emissions by 89% across the reference markets—this has the strongest impact of all the scenarios on CO2e emissions, thus guaranteeing the best outcome. Decreasing SABA use would require the need to improve asthma control through, for example, better diagnosis and assessment, additional maintenance treatments, medical education aimed at all stakeholders to improve patient follow-up, promotion of adherence, improvement in inhalation technique as well as digital health initiatives.36 38 39 SABA prescription practices would also need to be aligned with current treatment guideline recommendations.36 Although such changes are desired, addressing each of these hurdles remains a complex scenario, and there are no data to suggest that this is achievable in the short term.36 39 40 Therefore, the scenarios based on treatment optimisation tested in our analyses are somewhat optimistic.
Currently less than 1% of all inhalers are recycled every year.40 End-of-life recycling of inhalers has the potential to eliminate all emissions associated with inhaler disposal; however, recycling of 81%–87% of current inhalers is needed to match reductions achieved through transition to HFA-152a pMDIs. In clinical practice, such rates of end-of-life recycling may be very difficult to achieve and would require significant investment and changing behaviours—these data further advocate the introduction of low-GWP propellant pMDIs as a favoured option for reducing GHG emissions during pMDI use and end-of-life phases. Nevertheless, launching recycling schemes now would achieve short-term emission savings and result in established systems being available at the time of transition to low-GWP propellant pMDIs.
A strength of our study was the evaluation of four scenarios by which emissions reductions might be achieved in five separate reference markets, helping countries to make cost-effective and informed decisions, while also maintaining disease control. However, this was an exploratory study, a forward-looking analysis, thus relying on the quality of the model and quality of the data on which the modelling was based. Several assumptions were necessary, both overall and at the individual scenario level, in part to avoid the need to make further, potentially unreliable assumptions on product/class forecasts that would add an additional layer of uncertainty to the modelling. For example, whether it is realistic to assume the transition to the new products will take place over a short period or linearly will become apparent over time. Statistical comparisons between the different scenarios were not performed. The potential clinical impact of these emission reduction scenarios is a point for future investigation.
In conclusion, the introduction of low-GWP propellant (HFA-152a) inhalers represents an attractive and sustainable strategy to tackle the small contribution pMDIs make to global HFC emissions. The greatest reductions can be achieved through the transition from current pMDIs to those using low-GWP propellant (HFA-152a) for the delivery of both maintenance and rescue (SABA) therapies. Importantly, this approach, which in our analyses outperforms the substitution of pMDIs with DPI/SMIs, preserves current inhaler options and patient choice, which are essential for optimising treatment and clinical outcomes for individual patients. While these findings require confirmation in independent studies, it is possible to substantially reduce the adverse climate impact of pMDIs without restricting patient access to these inhaler devices.
Data availability statement
Data used in this analysis are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank Paolo Saccò (Global Public Affairs, Chiesi Farmaceutici) and Harriet Lewis (Public Affairs, Chiesi UK Ltd) for providing input to perform the analysis. This study was sponsored by Chiesi Farmaceutici. Medical writing support for the development of this manuscript, under the direction of the authors, was provided by Patrick Hoggard, of Ashfield MedComms, an Ashfield Health company, and was funded by Chiesi Farmaceutici.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SP and DP were involved in the conception and design of the study; FS, YU, RF, NR and CS were responsible for the data collection and acquisition. All authors were involved in the development of the primary manuscript, interpretation of data, critical review and revising the manuscript and have read and approved the final version to be submitted. SP acts as guarantor. All authors satisfy the criteria for authorship as established by the ICMJE.
Funding This study was funded by Chiesi Farmaceutici.
Competing interests DP was contracted by Chiesi Farmaceutici for the analysis. SP, FS, RF and YU are employees of Chiesi Farmaceutici.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.